Page 12 of 21
DR4.1 | Lichen Planus Diagnosis and Management — SDL Guide (Part 2)
Differential Diagnosis of Lichen Planus
Differential Diagnosis of Lichen Planus
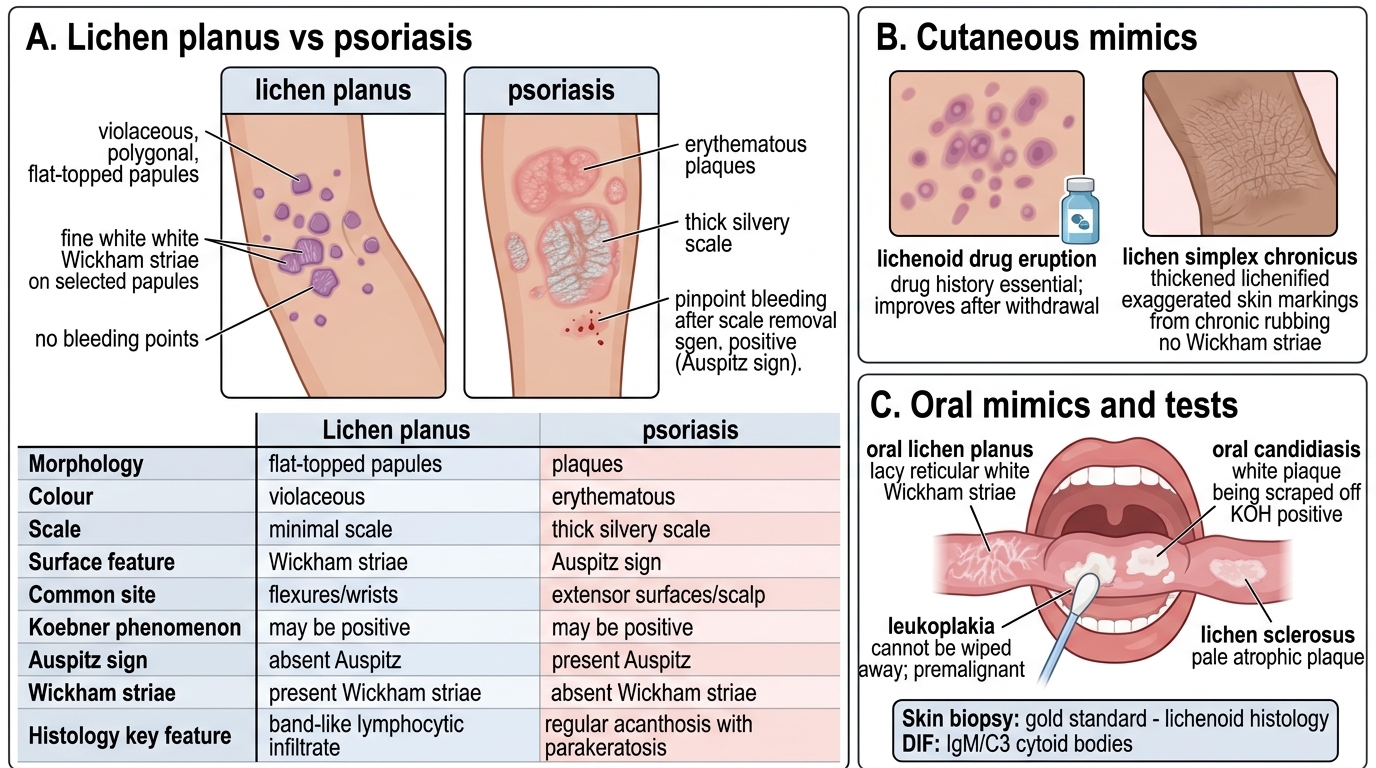
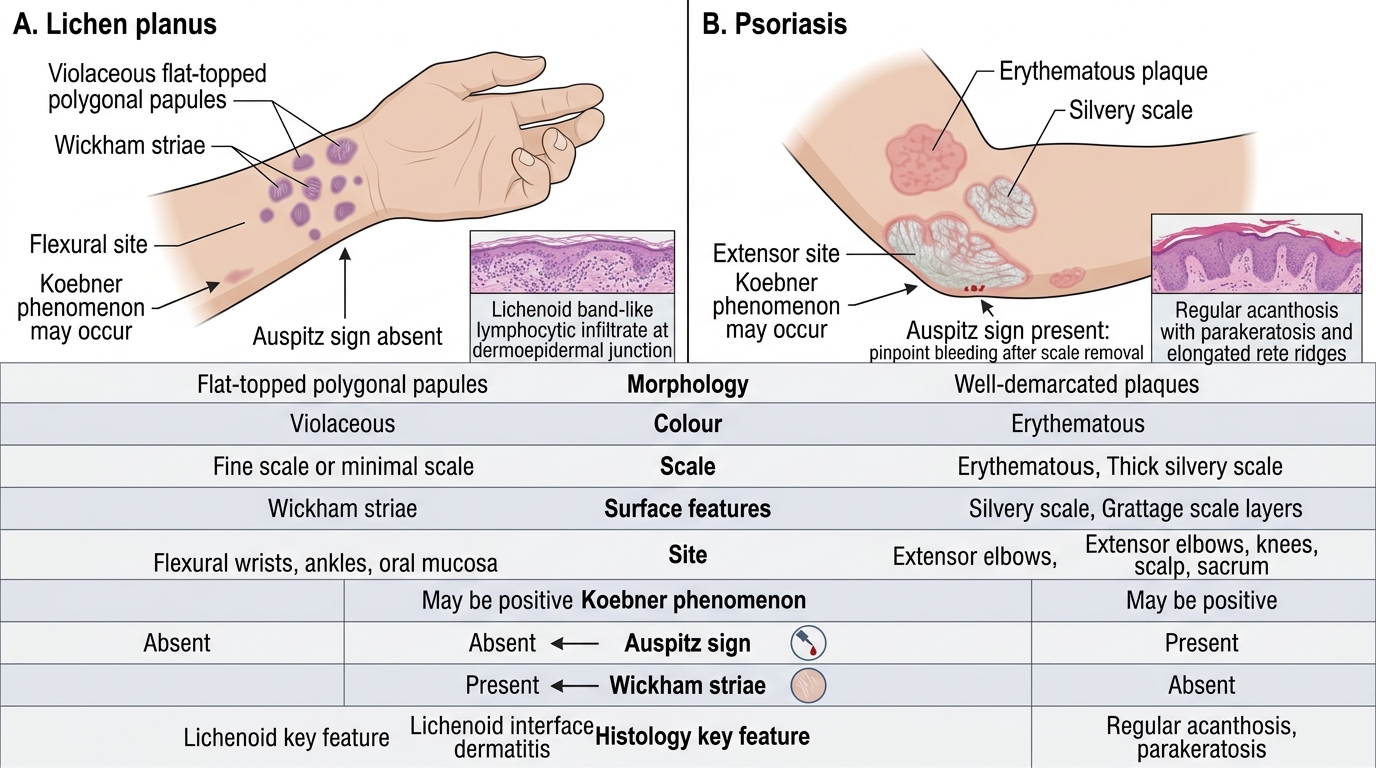
Because several conditions can mimic lichen planus on the skin and in the mouth, a structured differential — anchored on the contrast with psoriasis — is essential to avoid mismanagement. The most important cutaneous comparison is with psoriasis: psoriasis gives erythematous plaques with thick silvery scale, a positive Auspitz sign, and an extensor distribution, whereas lichen planus gives violaceous flat-topped papules with Wickham striae, no Auspitz sign, and a flexural distribution. A lichenoid drug eruption can be clinically indistinguishable, so a careful drug history is mandatory; it resolves on withdrawing the culprit. Lichen simplex chronicus shows thickened skin with exaggerated skin markings from chronic rubbing but lacks Wickham striae. In the mouth, oral lichen planus must be separated from oral candidiasis (the white plaque can be scraped off and KOH is positive), leukoplakia (a fixed white patch that cannot be wiped away and is itself premalignant), and lichen sclerosus.
Lichen Planus vs Psoriasis: Bedside Comparison
Investigations to resolve doubt:
- Skin biopsy — the gold standard, showing lichenoid histology.
- Direct immunofluorescence (DIF) — shows globular cytoid (colloid) bodies staining for IgM and C3 at the dermoepidermal junction.
- Hepatitis C serology — given the recognised association.
- Drug history review to exclude a lichenoid drug eruption.
SELF-CHECK
Which combination of features best distinguishes lichen planus from psoriasis at the bedside?
A. Erythematous plaques, silvery scale, positive Auspitz sign, extensor distribution
B. Violaceous flat-topped polygonal papules, Wickham striae, no Auspitz sign, flexural distribution
C. Greasy yellow scale on the scalp and eyebrows with a negative grattage test
D. A single herald patch followed by a Christmas-tree distribution on the trunk
Reveal Answer
Answer: B. Violaceous flat-topped polygonal papules, Wickham striae, no Auspitz sign, flexural distribution
Lichen planus is characterised by violaceous, flat-topped, polygonal papules bearing fine white Wickham striae, in a flexural distribution, and crucially WITHOUT the Auspitz sign. Psoriasis, by contrast, gives erythematous plaques with silvery scale, a positive Auspitz sign, and an extensor distribution. Greasy scale with a negative grattage describes seborrhoeic dermatitis, and a herald patch with Christmas-tree distribution describes pityriasis rosea.
Management of Lichen Planus
Management of Lichen Planus
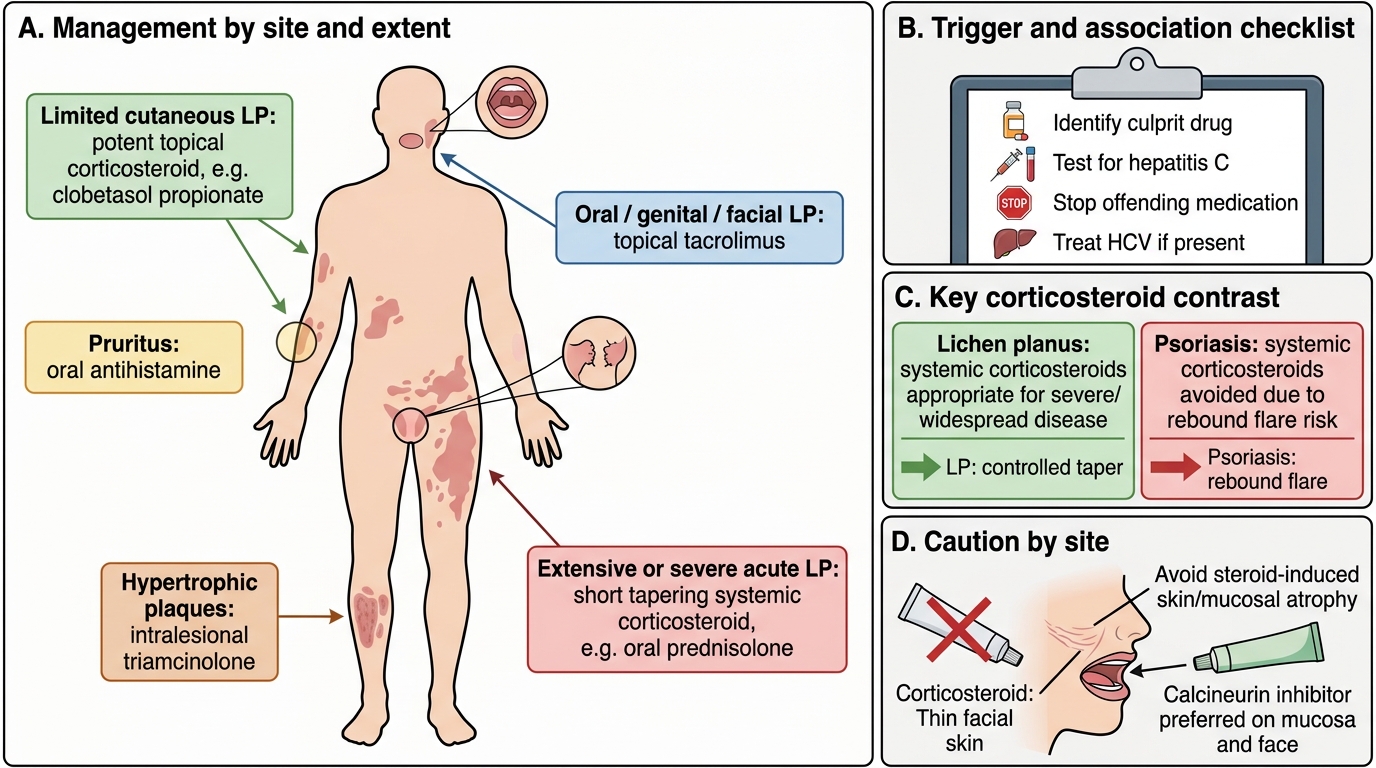
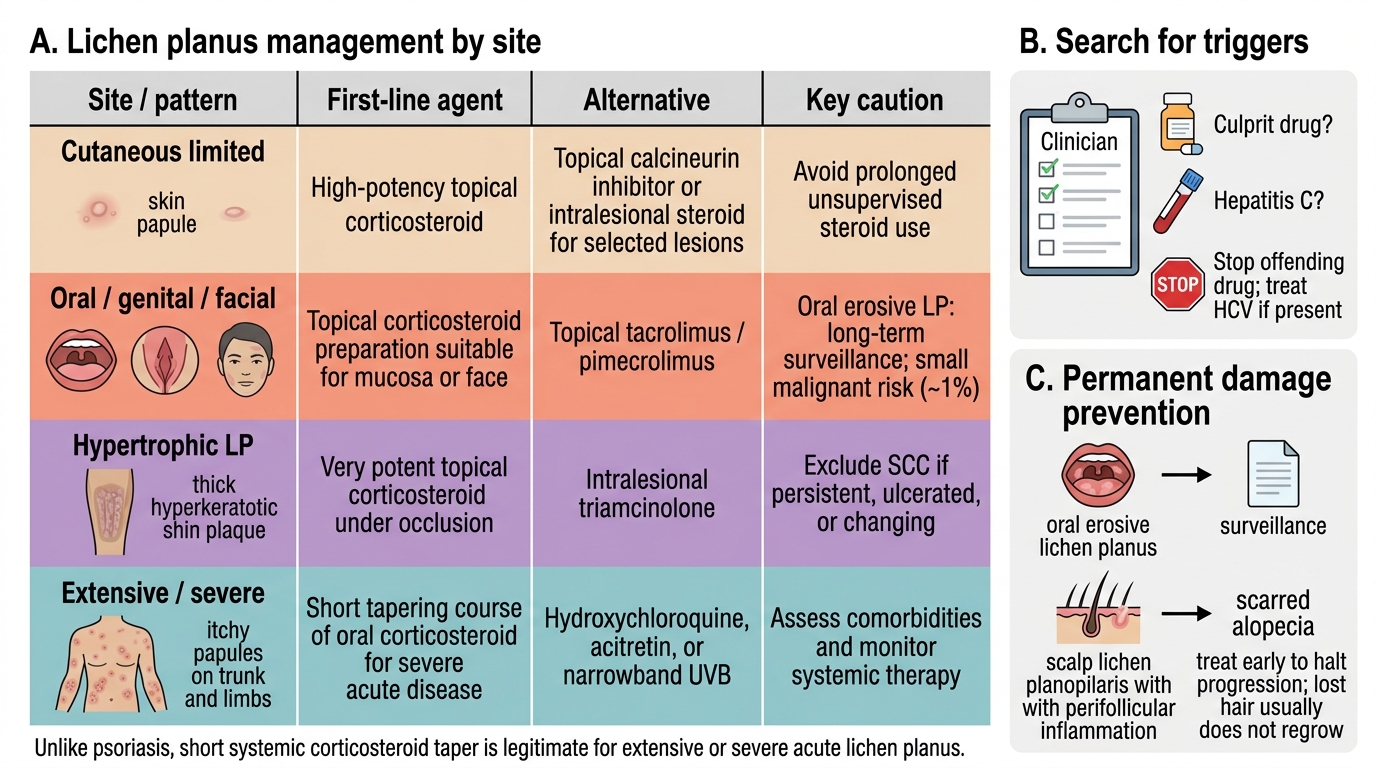
Managing lichen planus is guided by the site and extent of disease, and it differs from psoriasis in an important way that students must grasp: systemic corticosteroids are a legitimate and effective treatment here, not a contraindicated one. For limited cutaneous disease, the first-line treatment is a potent topical corticosteroid such as clobetasol propionate, which controls itch and flattens lesions; antihistamines help the pruritus. For oral, genital, or facial lichen planus, topical tacrolimus (a calcineurin inhibitor) is preferred because it avoids the mucosal and skin atrophy that prolonged topical steroids cause; intralesional triamcinolone is useful for thick hypertrophic plaques. For extensive or severe acute disease, a short, tapering course of systemic corticosteroids (for example oral prednisolone) is appropriate and effective — a key contrast with psoriasis, where systemic steroids are avoided because of rebound flares. Lichen planus does not carry that rebound risk, so systemic steroids are a reasonable option for widespread or distressing disease.
Lichen Planus Management by Site
Further points of management:
- Second-line options include hydroxychloroquine, acitretin, and phototherapy (narrowband UVB) for resistant or widespread disease.
- Oral erosive lichen planus requires long-term surveillance because of its small (~1%) risk of malignant transformation.
- Scarring alopecia from lichen planopilaris is usually permanent; treatment aims to halt progression early rather than to regrow lost hair.
- Identify and stop any culprit drug, and treat associated hepatitis C where present.
SELF-CHECK
A patient has widespread, intensely itchy cutaneous lichen planus that is severely affecting sleep and quality of life. Regarding a short tapering course of oral corticosteroids, which statement is correct?
A. It is contraindicated, exactly as in psoriasis, because of rebound pustular flares
B. It is a legitimate and effective option for extensive or severe acute lichen planus, which — unlike psoriasis — does not carry the steroid rebound-flare risk
C. It is useless because lichen planus does not respond to corticosteroids
D. It should be given indefinitely as lifelong maintenance
Reveal Answer
Answer: B. It is a legitimate and effective option for extensive or severe acute lichen planus, which — unlike psoriasis — does not carry the steroid rebound-flare risk
Unlike psoriasis, lichen planus does NOT carry the danger of a steroid-withdrawal rebound into pustular or erythrodermic disease, so a short, tapering course of systemic corticosteroids is a legitimate and effective treatment for extensive or severe acute lichen planus. This is a key examination distinction: systemic steroids are contraindicated in psoriasis but usable in lichen planus. They are used as a short course, not indefinite maintenance.
Self-Assessment — Lichen Planus Recognition and Management
Consolidate your understanding by rehearsing the whole diagnostic and therapeutic reasoning for lichen planus, deliberately contrasting it with psoriasis at every step, because that contrast is both clinically important and a favourite of examiners. A competent student can recite the classic 'P' features and the significance of Wickham striae, explain the lichenoid mechanism and its drug and viral associations, recognise oral, nail, and scalp involvement and their implications, distinguish lichen planus from psoriasis and the other mimics, and devise a site-appropriate management plan including the permitted use of systemic steroids. Work through the prompts below by imagining real patients and explaining your reasoning aloud; the ability to teach the psoriasis–lichen-planus contrast clearly is a good test of having truly learned it.
Self-check prompts:
- Recite the classic clinical 'P' features of lichen planus and name the diagnostic surface sign.
- Which nail change is pathognomonic of lichen planus?
- How does the safe use of systemic corticosteroids differ between lichen planus and psoriasis, and why?
- What is the first-line treatment for symptomatic oral erosive lichen planus, and what long-term action does that diagnosis require?
- List three features that separate lichen planus from psoriasis at the bedside.
CLINICAL PEARL
Read the colour and the surface, and let lichen planus declare itself against psoriasis. Violaceous, flat-topped, polygonal papules with fine white Wickham striae and no Auspitz sign on the flexor wrists are lichen planus; red plaques with silvery scale and a positive Auspitz sign on the extensors are psoriasis. Always look in the mouth, at the nails (pterygium unguis is pathognomonic), and on the scalp. And remember the management contrast that examiners love: systemic corticosteroids are contraindicated in psoriasis but are a legitimate short-course treatment in extensive lichen planus, which does not rebound. Oral erosive lichen planus earns long-term surveillance for its small malignant potential.