Page 1 of 21
DR3.1 | Psoriasis Recognition and Differential Diagnosis — SDL Guide
Learning Objectives
- Describe the cardinal morphology of a psoriatic plaque and recognise the silvery-white (candle-grease) scale, Auspitz sign, and Koebner phenomenon used in recognition.
- Classify psoriasis into its four major clinical variants — chronic plaque, guttate, pustular, and erythrodermic — with their distinguishing features and triggers.
- Outline the etiopathogenesis of psoriasis at a level sufficient to explain its clinical signs.
- Construct a structured differential diagnosis distinguishing psoriasis from seborrhoeic dermatitis, pityriasis rosea, lichen planus, tinea corporis, and secondary syphilis.
- Explain how accurate morphological recognition determines the safe management pathway, including why systemic corticosteroids are avoided.
INSTRUCTIONS
Psoriasis is one of the commonest chronic papulosquamous disorders you will encounter, and it is also one of the most frequently misdiagnosed — mistaken for fungal infection, eczema, or seborrhoeic dermatitis, leading to wrong and sometimes harmful treatment. This module trains you to recognise the psoriatic plaque on sight, to name its variant correctly, and to separate it confidently from its mimics. Getting the diagnosis right is not academic: it directly determines whether the patient receives a topical, a phototherapy, or a systemic plan, and it is the safeguard against giving a systemic steroid that can precipitate a life-threatening flare.
References
- IADVL Textbook of Dermatology, Section on Papulosquamous Disorders — Psoriasis (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & STD, Ch. on Psoriasis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 32-year-old man comes to the skin OPD with thick, scaly, itchy patches over both elbows and knees that have waxed and waned for three years. A previous prescriber treated him for 'ringworm' with an antifungal cream and then with a potent topical-steroid–antifungal combination; the patches briefly flattened and then returned worse. On examination you see well-defined red plaques topped with loose silvery scale. You gently lift a flake of scale and it comes away like a shaving of candle wax; a little further scraping reveals tiny pinpoint bleeding spots. In that moment the diagnosis declares itself — this is psoriasis, not a fungal infection. The cost of the earlier error was months of inappropriate treatment. Recognition is the whole game here, and it begins with reading the plaque correctly.
WHY THIS MATTERS
As a final-year student and intern, you will see papulosquamous lesions constantly — in the skin OPD, in general medicine wards, and in the community. Psoriasis affects roughly 1–2% of the population, runs a lifelong relapsing course, and carries a heavy psychological and quality-of-life burden that is often invisible to an untrained eye. The single most valuable thing you can do for these patients is to make the correct diagnosis early, because the entire management pathway — topical versus phototherapy versus systemic — branches from it, and because a confident diagnosis lets you warn the patient away from dangerous shortcuts such as systemic steroids and unregulated 'skin specialists'. Recognising psoriasis and separating it from its mimics is therefore a core clinical skill, not a specialist nicety.
RECALL
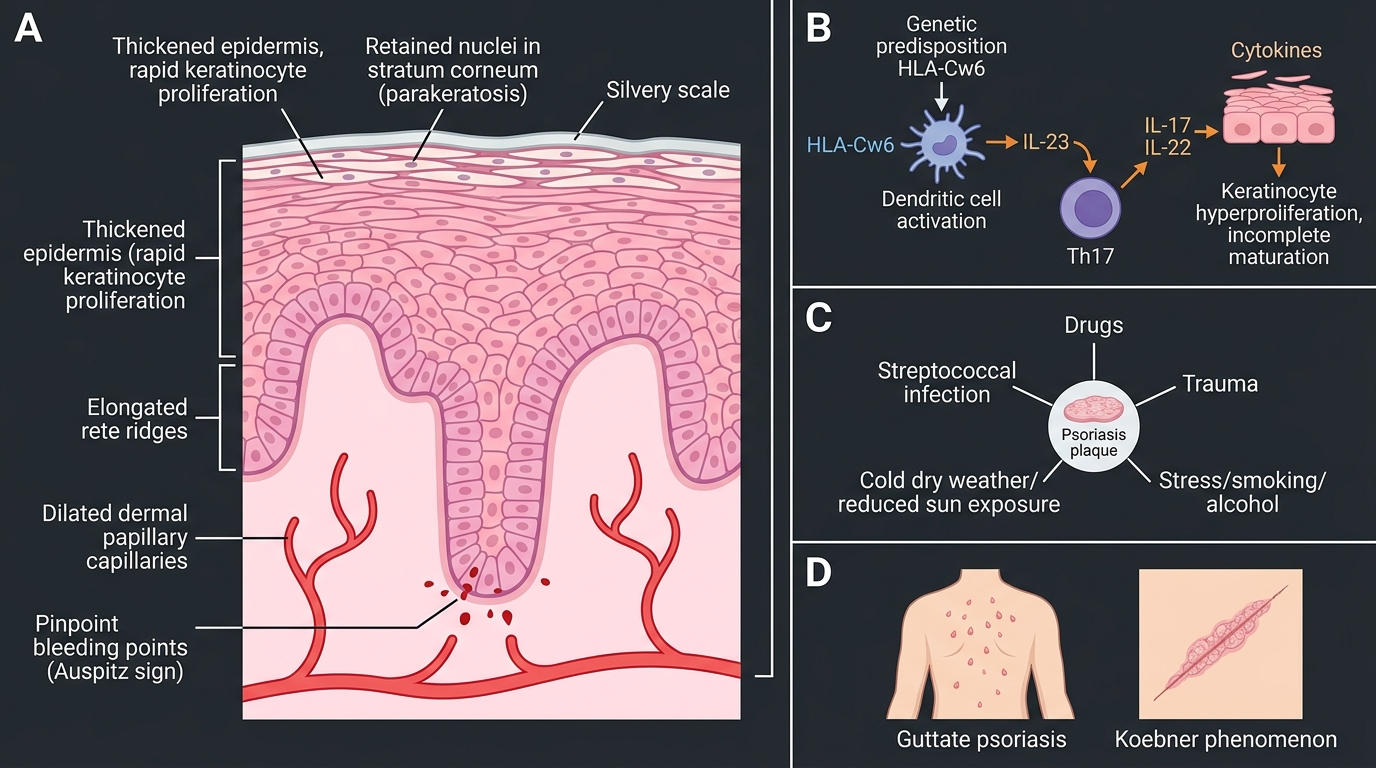
Before we begin, recall the normal architecture of the epidermis from your first-year anatomy and histology: the basal layer where keratinocytes are born, the spinous and granular layers where they mature, and the stratum corneum — the flat, anucleate horny layer that forms the skin's surface scale. In normal skin, a keratinocyte takes about 28 days to travel from the basal layer to be shed at the surface. Hold on to one more idea from physiology: the dermal papillae just beneath the epidermis carry small blood capillaries. Psoriasis is, at its core, a disease of grossly accelerated keratinocyte turnover combined with these dermal capillaries being brought abnormally close to the surface — and almost every clinical sign you are about to learn flows directly from those two facts.
Morphology of the Psoriatic Plaque
Morphology of the Psoriatic Plaque
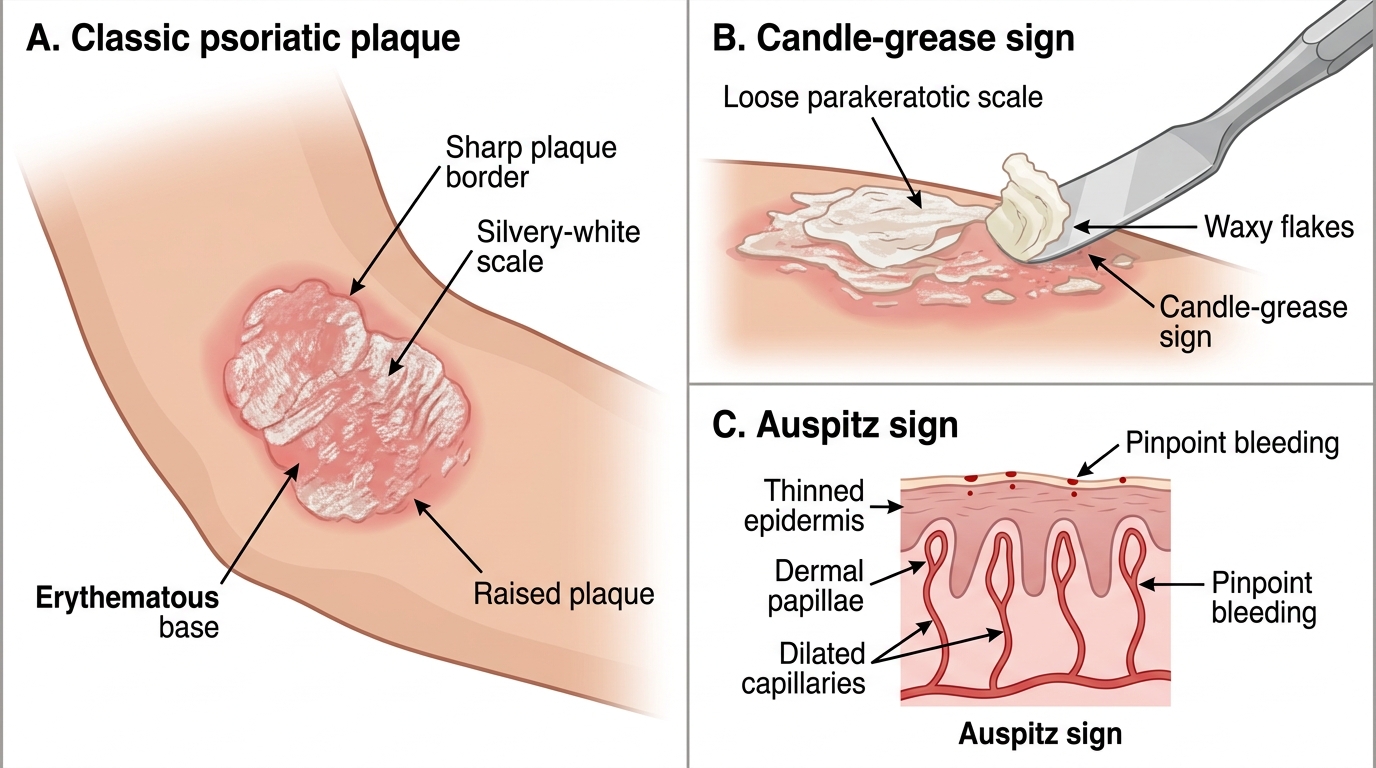
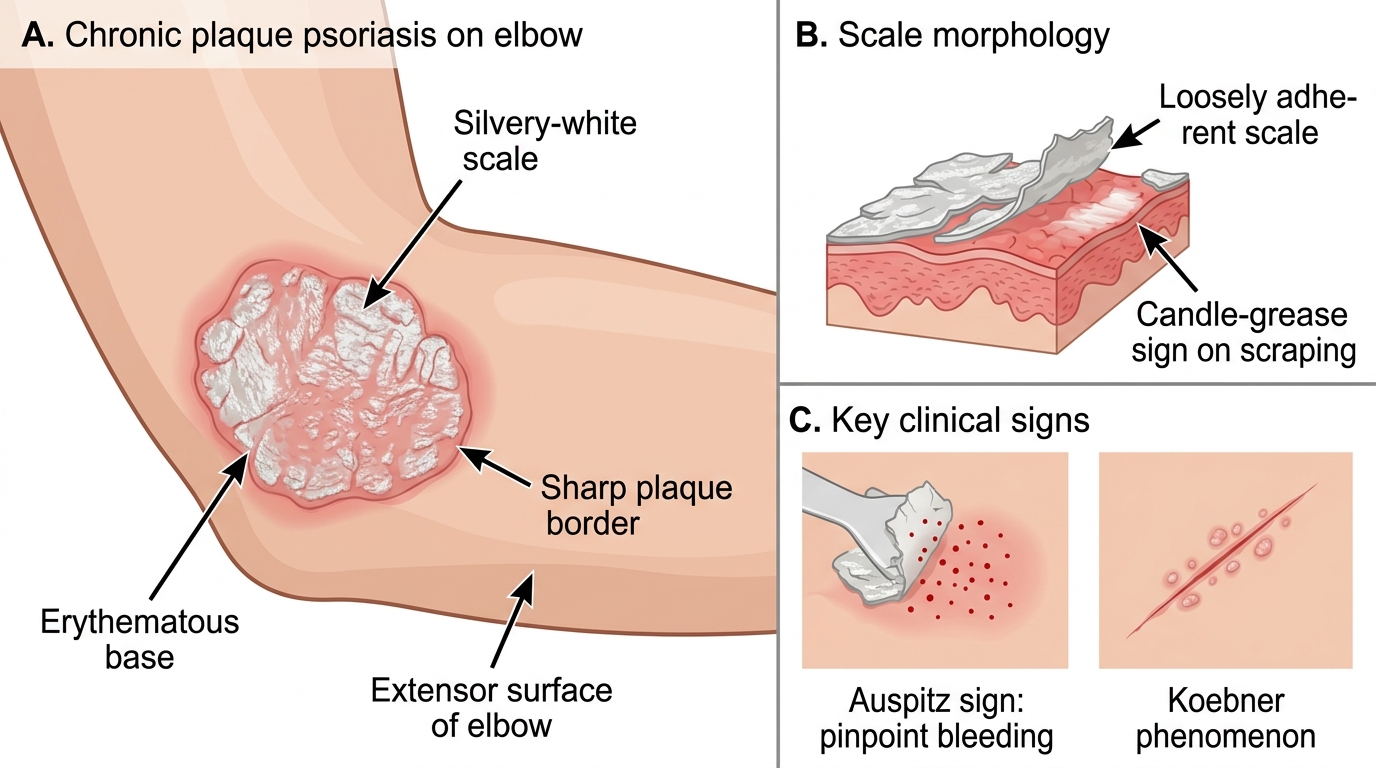
The diagnosis of psoriasis is, in the great majority of cases, a clinical one made by reading the morphology of the lesion carefully. The classic lesion is a plaque — a well-demarcated, raised, erythematous (red) area larger than a papule — surfaced by loose, dry, silvery-white scale. The scale is the visible consequence of the accelerated keratinocyte turnover you recalled a moment ago: cells reach the surface in three to four days instead of four weeks, arriving immature and piling up as parakeratotic scale. Two elicited signs are central to bedside recognition. When the scale is gently scraped, it flakes off in waxy layers — the candle-grease sign — because the loose parakeratotic scale separates easily. Continue removing the scale and you expose a thin surface that, on further gentle trauma, produces discrete pinpoint bleeding points: this is the Auspitz sign, and it occurs because the dermal papillae carrying dilated capillaries sit immediately beneath a thinned epidermis. (The full graded-scraping procedure that elicits these signs in sequence — including the glistening last membrane — is a defined bedside skill, the Grattage test, covered separately in DR3.2; here we use candle-grease scale and Auspitz only as recognition cues.)
Chronic Plaque Psoriasis: Morphology and Clinical Signs
Key morphological cues to fix in memory:
- Well-defined margin — psoriatic plaques have sharp borders, unlike the ill-defined patches of eczema.
- Silvery-white, loosely adherent scale (candle-grease sign on scraping).
- Auspitz sign — pinpoint bleeding after scale removal — reflecting dilated dermal papillary capillaries.
- A third sign, the Koebner phenomenon, describes new psoriatic lesions appearing along sites of trauma such as a scratch or surgical scar; it is supportive but not unique to psoriasis.
Clinical Variants of Psoriasis
Clinical Variants of Psoriasis
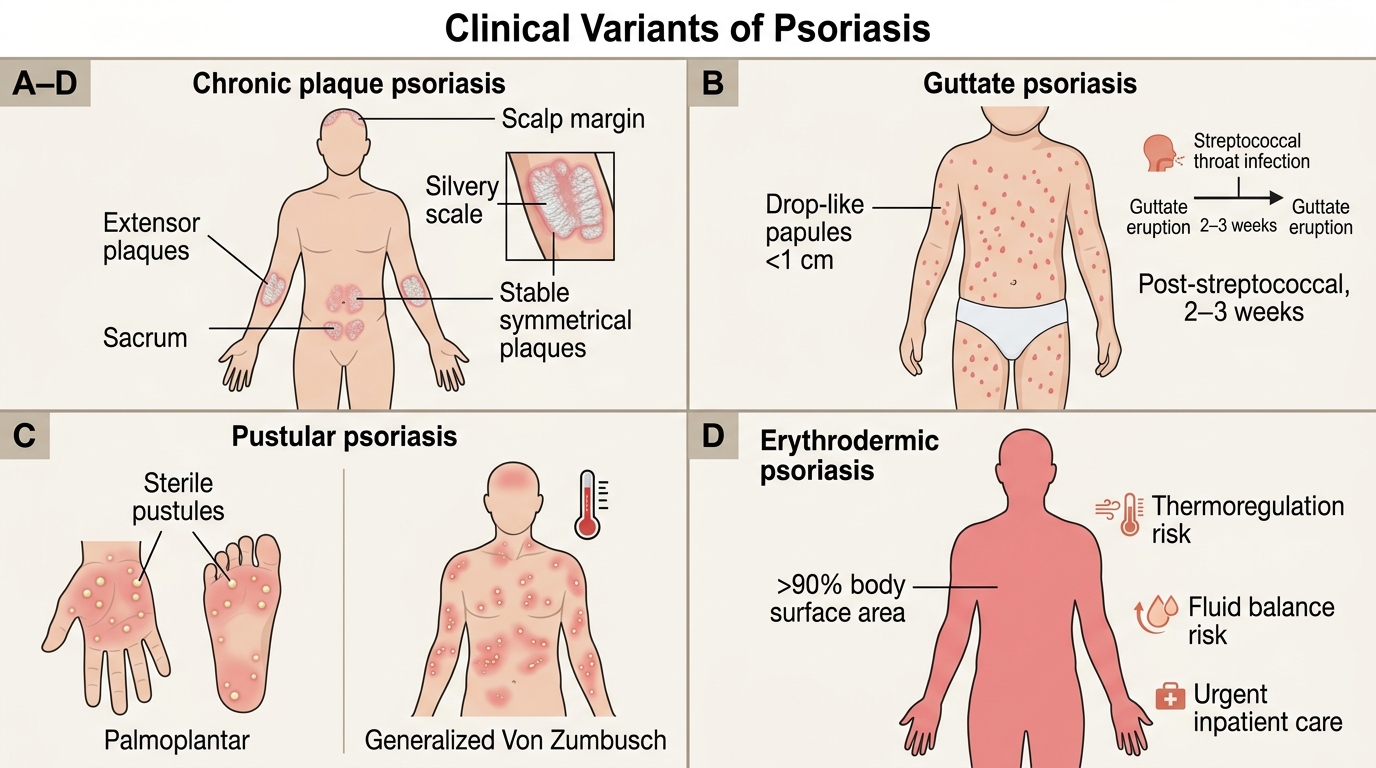
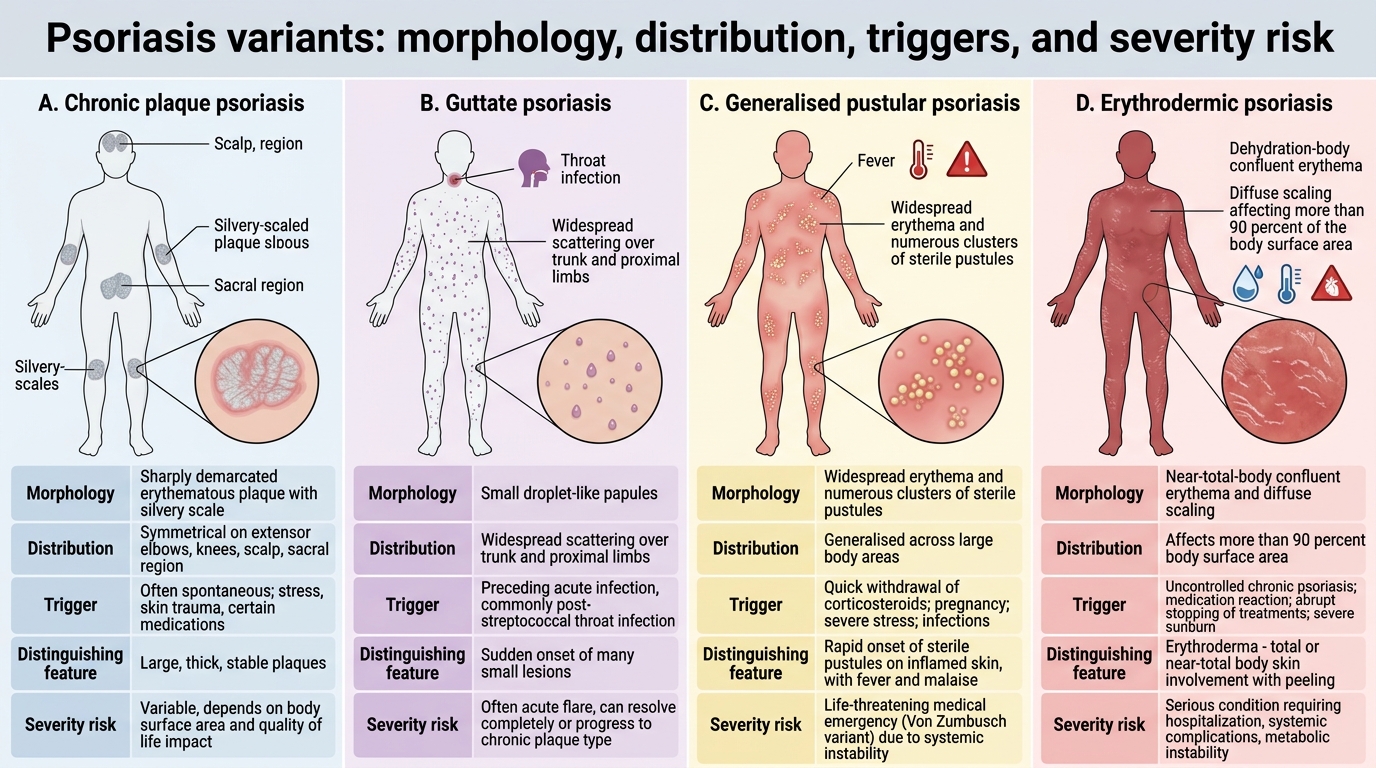
Psoriasis is not a single appearance but a family of related presentations, and naming the variant correctly matters because it changes both the differential and the management. The commonest form by far is chronic plaque psoriasis (psoriasis vulgaris), which favours the extensor surfaces — elbows, knees, the scalp, the sacrum and the umbilicus — with stable, symmetrical, well-defined plaques. Guttate psoriasis appears abruptly as crops of small (under 1 cm), droplet-shaped ("guttate" = drop-like) papules scattered over the trunk and proximal limbs, characteristically two to three weeks after a streptococcal throat infection — making it a classically post-streptococcal presentation that is commonest in children and young adults. Pustular psoriasis is defined by sterile pustules rather than scale; it may be localised to the palms and soles (palmoplantar) or generalised (the acute, febrile, dangerous Von Zumbusch pattern). Erythrodermic psoriasis is the most severe variant, in which inflammation involves more than 90% of the body surface area, threatening thermoregulation and fluid balance and requiring urgent inpatient care.
Comparison of Major Psoriasis Variants
A quick variant map:
| Variant | Morphology | Distribution | Key feature |
|---|---|---|---|
| Chronic plaque (commonest) | Silvery-scaled plaques | Extensors, scalp, sacrum | Stable, symmetrical |
| Guttate | Small droplet papules | Trunk, proximal limbs | Post-streptococcal |
| Pustular | Sterile pustules | Palms/soles or generalised | Von Zumbusch is a medical emergency |
| Erythrodermic | Confluent erythema + scale | >90% BSA | Systemic instability |
SELF-CHECK
A 9-year-old develops a sudden shower of small, drop-shaped scaly papules over the trunk three weeks after a sore throat. Which variant of psoriasis is this, and what is the classic trigger?
A. Chronic plaque psoriasis, triggered by trauma to extensor surfaces
B. Guttate psoriasis, triggered by a preceding streptococcal throat infection
C. Pustular psoriasis, triggered by abrupt withdrawal of systemic steroids
D. Erythrodermic psoriasis, triggered by extensive sunburn
Reveal Answer
Answer: B. Guttate psoriasis, triggered by a preceding streptococcal throat infection
The sudden eruption of small (<1 cm), droplet-shaped ("guttate") scaly papules over the trunk and proximal limbs, typically two to three weeks after a streptococcal pharyngitis, is the textbook picture of guttate psoriasis. It is the classically post-streptococcal variant and is commonest in children and young adults. Chronic plaque psoriasis is stable and extensor; pustular psoriasis shows sterile pustules; erythrodermic psoriasis involves >90% BSA.
Etiopathogenesis of Psoriasis
Etiopathogenesis of Psoriasis
Understanding why psoriasis looks the way it does makes recognition far more secure, so it is worth grasping its mechanism even in a recognition-focused module. Psoriasis is a chronic, immune-mediated inflammatory disease arising in a genetically predisposed person — the strongest single genetic association is with HLA-Cw6, and the inheritance is polygenic, which is why a family history is common but not invariable. The central immunological event is activation of the IL-23/IL-17 axis: dendritic cells and T-helper-17 lymphocytes drive a cytokine cascade that makes keratinocytes proliferate far too rapidly and incompletely, producing the immature parakeratotic scale, while simultaneously dilating the dermal papillary capillaries that give the plaque its red colour and underlie the Auspitz sign. A number of well-recognised factors can trigger or worsen disease, and asking about them is part of clinical assessment.
Common triggers and aggravators:
- Streptococcal infection — the classic precipitant of guttate psoriasis.
- Drugs — lithium, beta-blockers, antimalarials, and NSAIDs can precipitate or worsen psoriasis; abrupt withdrawal of systemic corticosteroids can trigger pustular/erythrodermic flares.
- Physical trauma — provoking the Koebner phenomenon.
- Psychological stress, smoking, and alcohol.
- Cold, dry weather and reduced sun exposure in many patients.