Page 2 of 21
DR3.1 | Psoriasis Recognition and Differential Diagnosis — SDL Guide (Part 2)
Clinical Features and Diagnosis of Psoriasis
Clinical Features and Diagnosis of Psoriasis
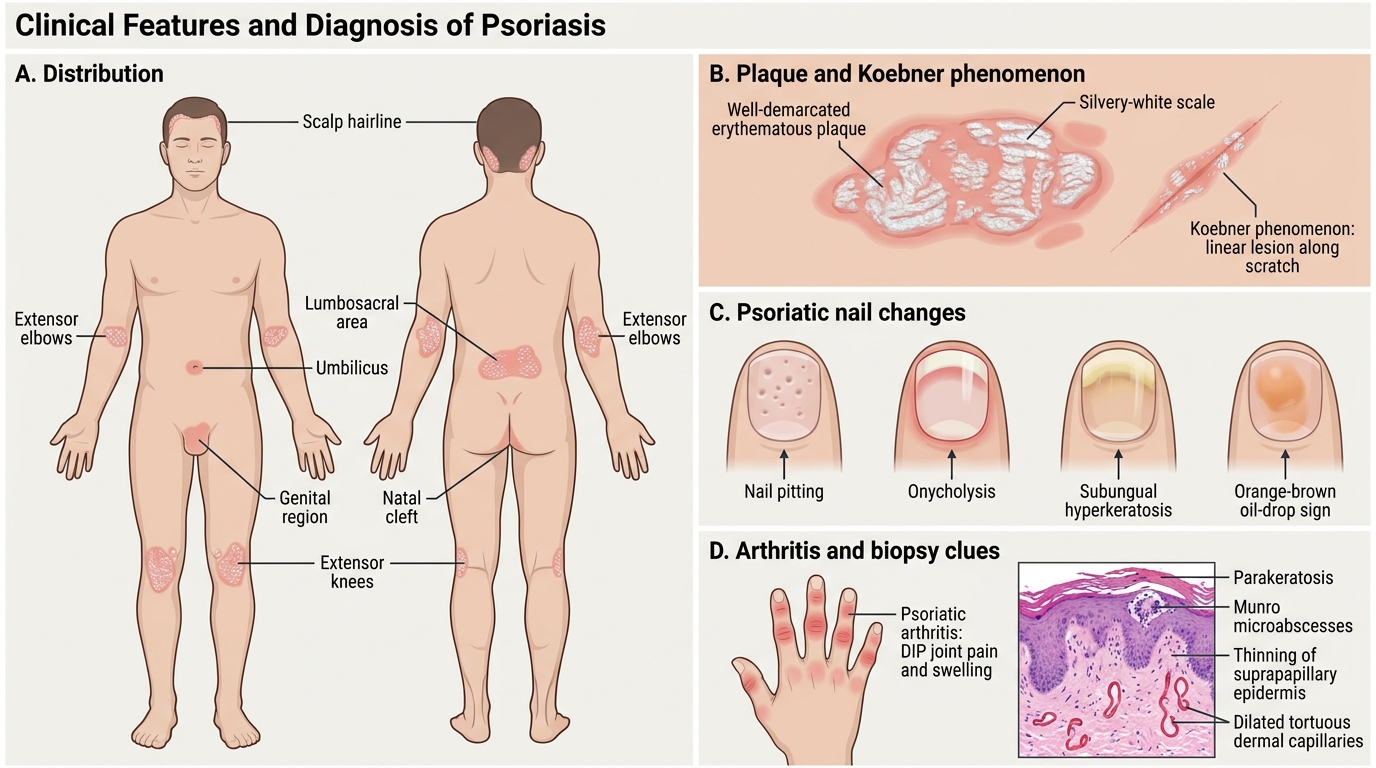
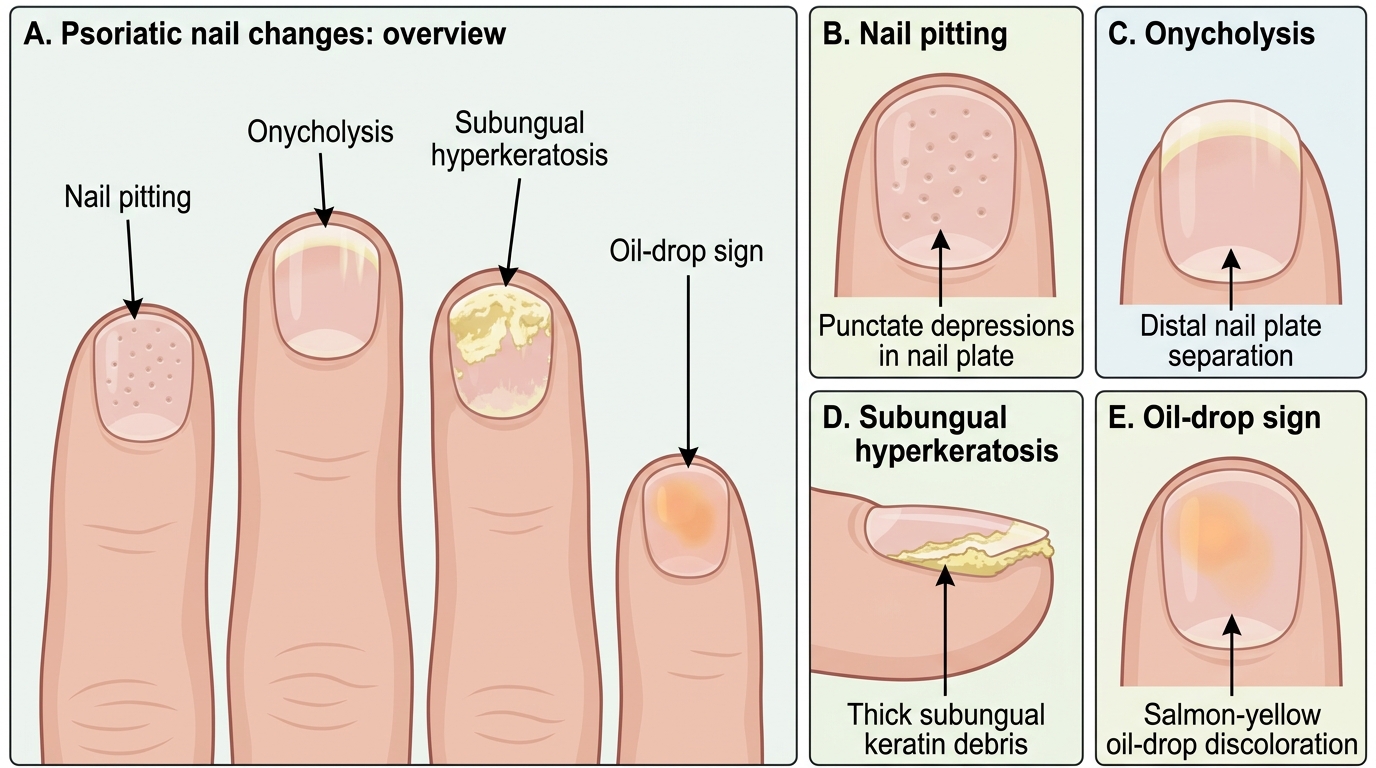
Moving from a single plaque to the whole patient, a systematic examination both confirms psoriasis and gauges its extent. Begin with the distribution: psoriasis has a strong predilection for the extensor surfaces (elbows, knees), the scalp (often with thick adherent scale at the hairline), the lumbosacral area, the umbilicus, the natal cleft and the genitalia. Examine the nails specifically, because nail change is a powerful diagnostic clue and a marker of disease severity and arthritis risk: look for pitting (small thumbprint-like depressions), onycholysis (distal separation of the nail plate), subungual hyperkeratosis, and the orange-brown "oil-drop" sign. Ask about and examine for psoriatic arthritis — joint pain and swelling, classically of the distal interphalangeal joints — which co-exists in a significant minority. Demonstrate the Koebner phenomenon if there is a linear lesion along a scratch. The diagnosis remains overwhelmingly clinical; a skin biopsy is reserved for atypical cases and characteristically shows parakeratosis, Munro microabscesses (neutrophils in the horny layer), thinning of the suprapapillary epidermis, and dilated tortuous capillaries — the histological correlates of the bedside signs.
Psoriatic Nail Changes
Checklist for the focused psoriasis examination:
- Sites — extensors, scalp, umbilicus, natal cleft, genitalia.
- Nails — pitting, onycholysis, oil-drop sign, subungual hyperkeratosis.
- Joints — screen for psoriatic arthritis (especially DIP joints).
- Signs — silvery scale, candle-grease and Auspitz on scraping, Koebner along trauma.
Differential Diagnosis of Psoriasis
Differential Diagnosis of Psoriasis
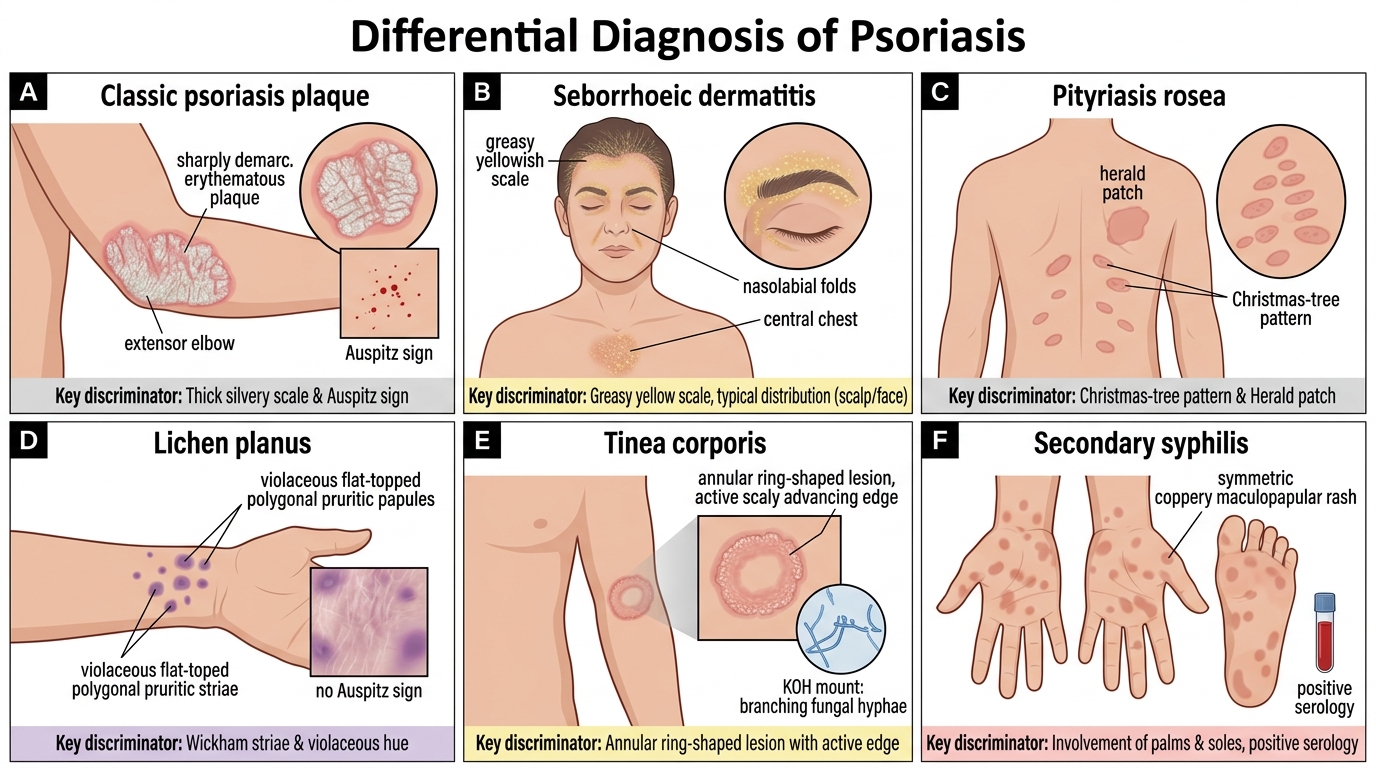
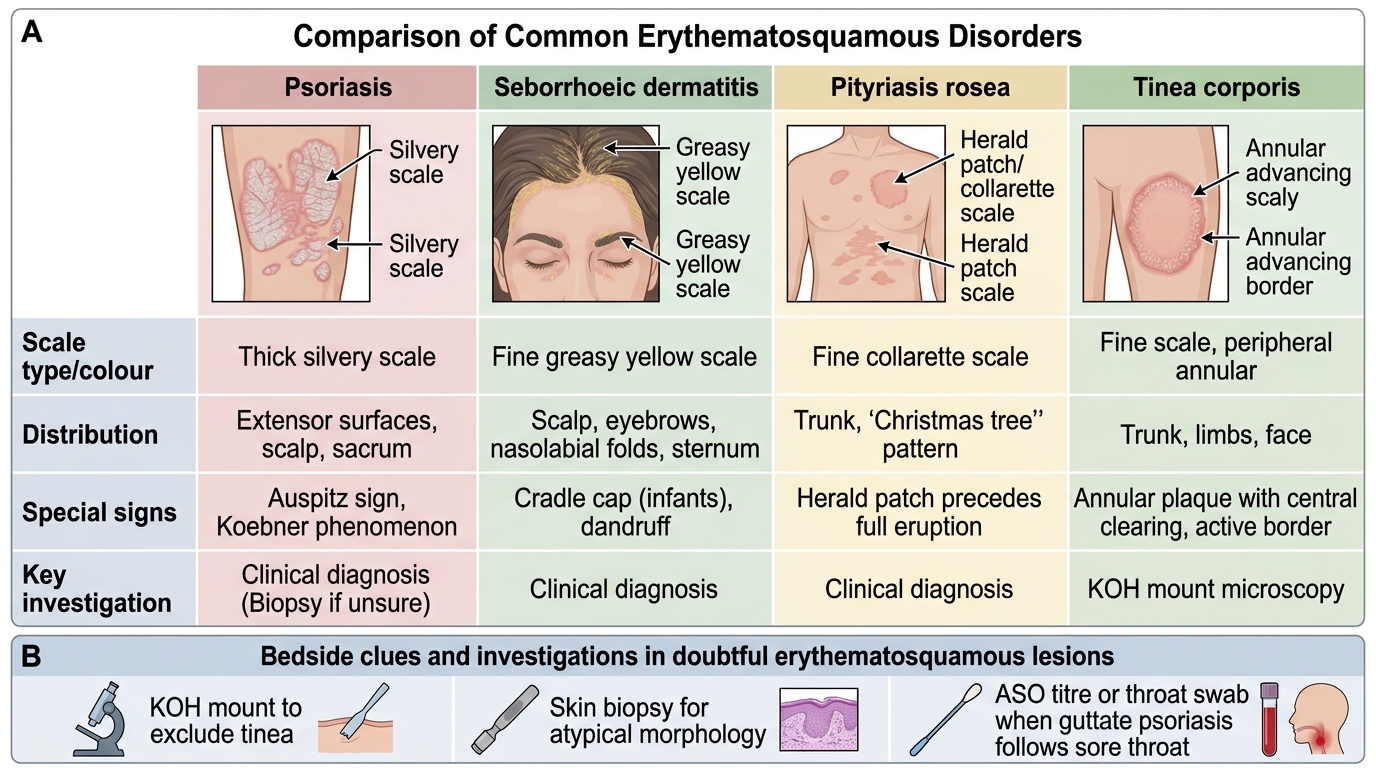
Because several conditions produce red, scaly lesions, a disciplined differential is what separates a safe clinician from a careless one. The most important mimics each have a discriminating feature, and learning these pairs is the core skill of this module. Seborrhoeic dermatitis produces greasy, yellowish scale on seborrhoeic sites (scalp, eyebrows, nasolabial folds, central chest) and lacks the silvery scale and Auspitz sign. Pityriasis rosea begins with a single "herald patch" followed by smaller oval lesions in a "Christmas-tree" distribution along skin cleavage lines on the trunk, is self-limiting over weeks, and does not show Auspitz. Lichen planus — covered in detail in DR4.1 — presents with violaceous, flat-topped, polygonal pruritic papules bearing fine white Wickham striae, and crucially has no Auspitz sign. Tinea corporis (ringworm) shows an annular lesion with central clearing and an active scaly advancing edge, and is confirmed by a positive KOH mount showing fungal hyphae — the test that would have spared our hook patient months of mistreatment. Secondary syphilis must be remembered because, unlike most papulosquamous diseases, it characteristically involves the palms and soles and is confirmed serologically.
Comparison of Erythematosquamous Disorders
For investigations in doubtful cases, reach for a KOH mount (to exclude tinea), a skin biopsy (for atypical morphology), and an ASO titre or throat swab when guttate psoriasis is suspected after a sore throat. Note that the formal graded grattage procedure is a separate bedside skill (DR3.2); for recognition, candle-grease scale plus Auspitz sign on careful scraping is sufficient.
SELF-CHECK
You see a patient with red scaly plaques and want to distinguish psoriasis from lichen planus at the bedside. Which single finding most reliably points AWAY from psoriasis and towards lichen planus?
A. Pinpoint bleeding (Auspitz sign) after scraping the scale
B. Silvery-white scale that flakes off like candle wax
C. Violaceous flat-topped papules with white lacy Wickham striae and no Auspitz sign
D. New lesions appearing along a scratch (Koebner phenomenon)
Reveal Answer
Answer: C. Violaceous flat-topped papules with white lacy Wickham striae and no Auspitz sign
Lichen planus is recognised by violaceous (purple), flat-topped, polygonal papules carrying fine white Wickham striae, and it does NOT produce the Auspitz sign. The Auspitz sign and silvery candle-grease scale are features of psoriasis, not lichen planus. The Koebner phenomenon is shared by both conditions (and by vitiligo), so it cannot be used to separate them — making the violaceous papule with Wickham striae and absent Auspitz the decisive discriminator.
Why Accurate Diagnosis Drives Management
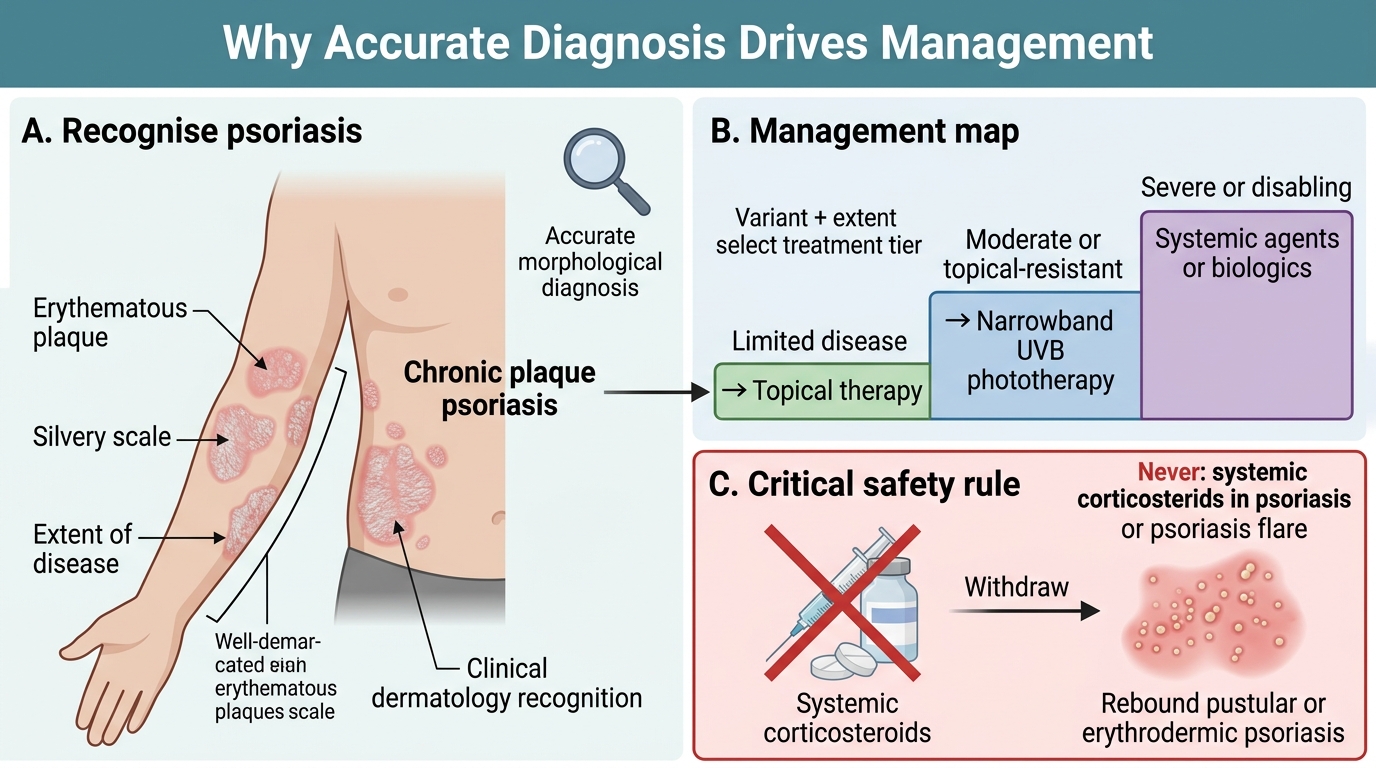
Psoriasis Diagnosis Guides Management and Safety
It is worth closing the recognition loop by seeing why all this morphological care matters at the point of treatment, even though detailed treatment planning belongs to DR3.3. The variant and extent you diagnose select the management tier directly: limited chronic plaque disease is managed with topical agents, more extensive disease with phototherapy, and severe or disabling disease with systemic therapy. Most importantly, accurate recognition protects the patient from a specific and serious error. Systemic corticosteroids are contraindicated in psoriasis: although they may transiently improve the skin, their withdrawal can precipitate a rebound flare into generalised pustular or erythrodermic psoriasis, which is potentially life-threatening. The same caution applies to potent oral or injected steroids prescribed for unrelated reasons in a known psoriatic. Recognising psoriasis correctly is therefore not only a diagnostic exercise but a safety intervention — it tells you what to do and, just as vitally, what never to do.
The one-line management map (detailed in DR3.3):
- Limited disease → topical therapy.
- Moderate / topical-resistant → phototherapy (narrowband UVB).
- Severe / disabling → systemic agents or biologics.
- Never → systemic corticosteroids (rebound pustular/erythrodermic flare).