Page 8 of 21
DR3.3 | Psoriasis Treatment Planning and Counselling — SDL Guide
Learning Objectives
- Frame psoriasis as a chronic, relapsing, incurable disease and set realistic expectations with the patient.
- Relate treatment targets to the underlying pathophysiology (IL-23/IL-17 axis, keratinocyte hyperproliferation).
- Assess severity using BSA, PASI, and DLQI and stratify patients into topical, phototherapy, and systemic tiers.
- Select appropriate topical, phototherapy, and systemic agents, stating key monitoring needs and contraindications.
- Explain why systemic corticosteroids are contraindicated and counsel the patient on chronicity, adherence, triggers, and psychosocial impact.
INSTRUCTIONS
Once psoriasis is correctly recognised (DR3.1), the next clinical task is to devise a rational, individualised treatment plan and to counsel the patient honestly about a disease that will accompany them for life. This module teaches you to match treatment intensity to disease severity, to choose agents safely, and — crucially — to communicate. Patients with psoriasis are frequently let down not by a lack of drugs but by poor explanation: they expect a cure, abandon treatment when remission fades, or fall prey to harmful steroid shortcuts. Your job is to plan the therapy and to be the person who explains chronicity, sets expectations, and keeps the patient safe.
References
- IADVL Textbook of Dermatology, Section on Management of Psoriasis (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & STD, Ch. on Psoriasis — Treatment (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old teacher with chronic plaque psoriasis returns to clinic, frustrated. "The cream worked, doctor — my skin was clear for two months. Then it all came back. The medicine has stopped working." She has, in fact, done nothing wrong; she has simply met the natural history of her disease, which no one ever explained to her. On her last visit elsewhere she was given a course of oral steroids that cleared her dramatically — and then, two weeks after stopping them, she erupted in painful sterile pustules and a fever and was admitted. Both episodes — the disappointment and the dangerous flare — were preventable, not with a better drug but with better counselling and a safer plan. Devising a treatment plan for psoriasis is inseparable from counselling the patient about its chronicity. That is the dual task of this module.
WHY THIS MATTERS
As a clinician you will manage psoriasis across a spectrum from a few stubborn plaques to disabling, life-altering disease, and your decisions will determine not only the state of the skin but the patient's mental health, adherence, and safety. Choosing the right tier of therapy avoids both under-treatment (leaving a patient to suffer) and over-treatment (exposing them to needless toxicity). Understanding the contraindication to systemic steroids prevents a foreseeable emergency. And learning to counsel — to explain that psoriasis is controllable but not curable, that remissions and relapses are expected, and that adherence and trigger-avoidance matter — is what converts a prescription into effective care. These are core skills you will use in any branch of medicine, because psoriatic patients present everywhere.
RECALL
Recall from DR3.1 the recognition of psoriasis and its variants — chronic plaque, guttate, pustular, and erythrodermic — and the immunological mechanism that drives it: activation of the IL-23/IL-17 axis causing keratinocyte hyperproliferation and dermal capillary dilatation. Recall, too, that systemic corticosteroids are contraindicated in psoriasis because their withdrawal can precipitate a pustular or erythrodermic flare. Bring forward one more idea from your communication-skills foundation: chronic-disease counselling is itself a clinical intervention, requiring you to set expectations, build a shared plan, and support adherence over years. Every treatment choice you make in this module sits on top of these facts — the mechanism tells you what the drugs target, the variant and severity tell you which tier to use, and the counselling makes the plan actually work.
Psoriasis as a Chronic Relapsing Disease — Setting Expectations
Psoriasis: Chronic Relapsing Course and Patient Expectations
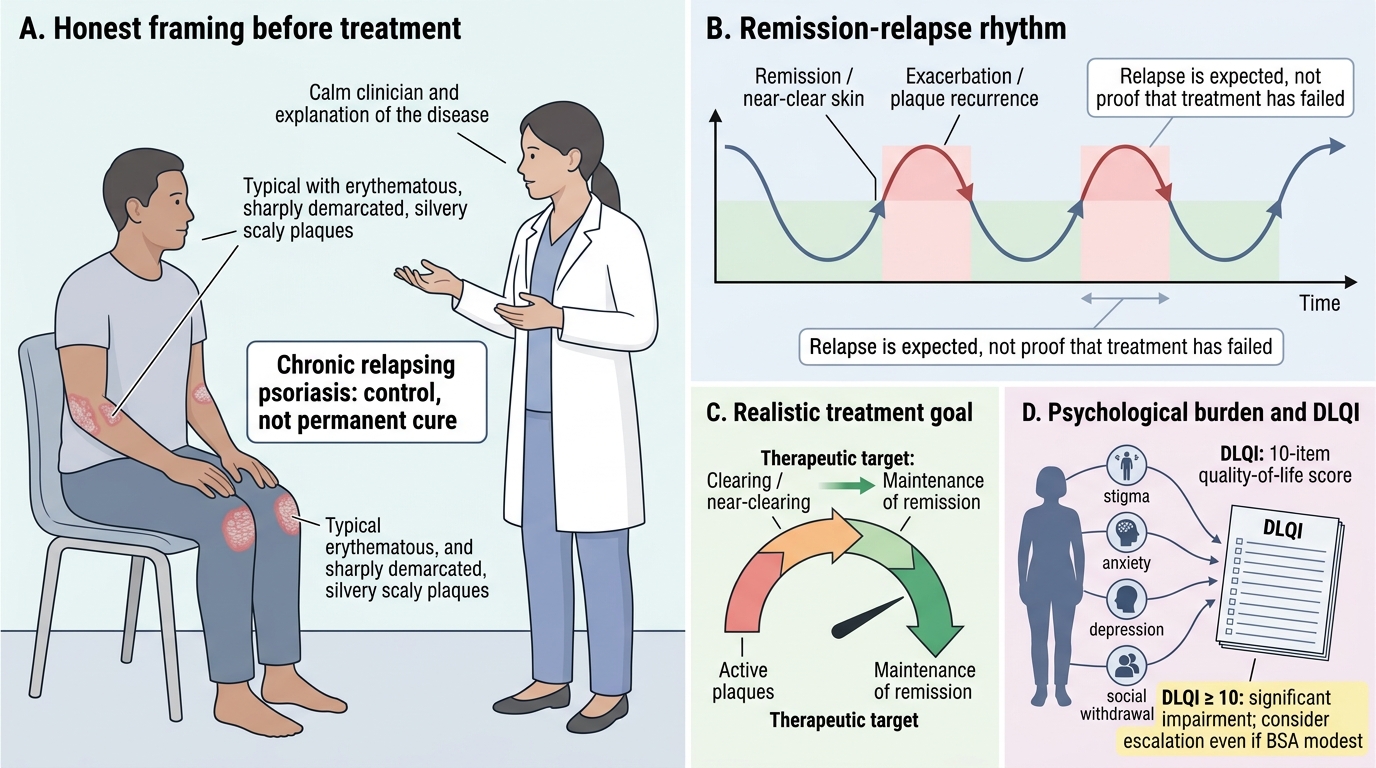
Before any drug is chosen, the single most important therapeutic act is to frame the disease honestly for the patient, because an unrealistic expectation is the commonest cause of treatment failure and of dangerous self-directed shortcuts. Psoriasis is a chronic, relapsing, and at present incurable condition; the realistic goal of treatment is sustained control — clearing or near-clearing of the skin and maintenance of remission — not a permanent cure. Patients must understand that remissions and exacerbations are the natural rhythm of the disease, so that the return of plaques after a good response is not a sign that 'the medicine stopped working' but an expected event to be managed. Just as important is acknowledging the disproportionate psychological burden: the visible, scaly nature of psoriasis carries stigma, and rates of depression, anxiety, and social withdrawal are high and often unrelated to the physical extent of disease. This is why patient-centred outcome measures matter from the outset.
The Dermatology Life Quality Index (DLQI) is a simple ten-item questionnaire that captures how much the disease affects daily life; a DLQI of 10 or more signals significant impairment and may justify escalating therapy even when the body-surface area looks modest. Setting these expectations early — chronicity, the remission-relapse pattern, and the legitimacy of psychological impact — is the foundation on which every subsequent treatment decision rests.
Pathophysiological Basis of Treatment Targets
Psoriasis Pathway and Treatment Targets
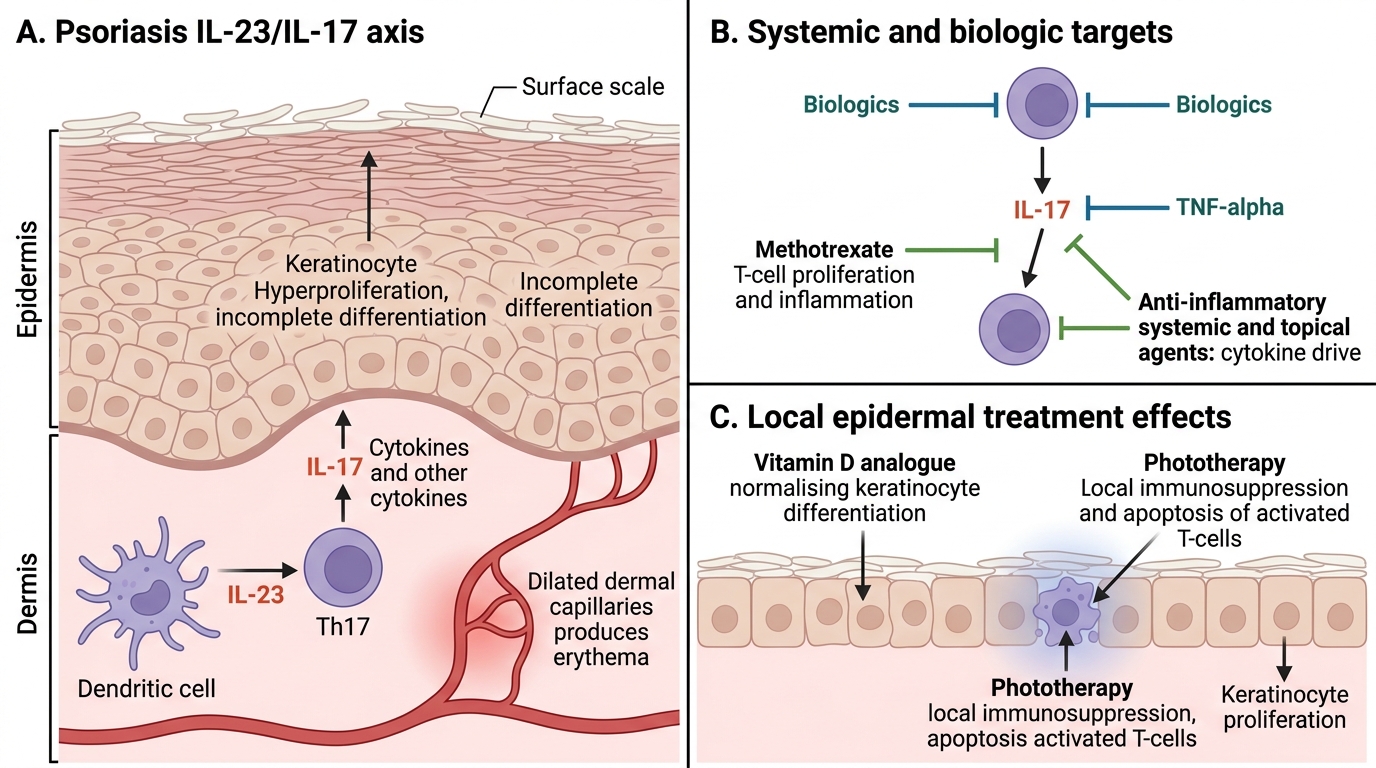
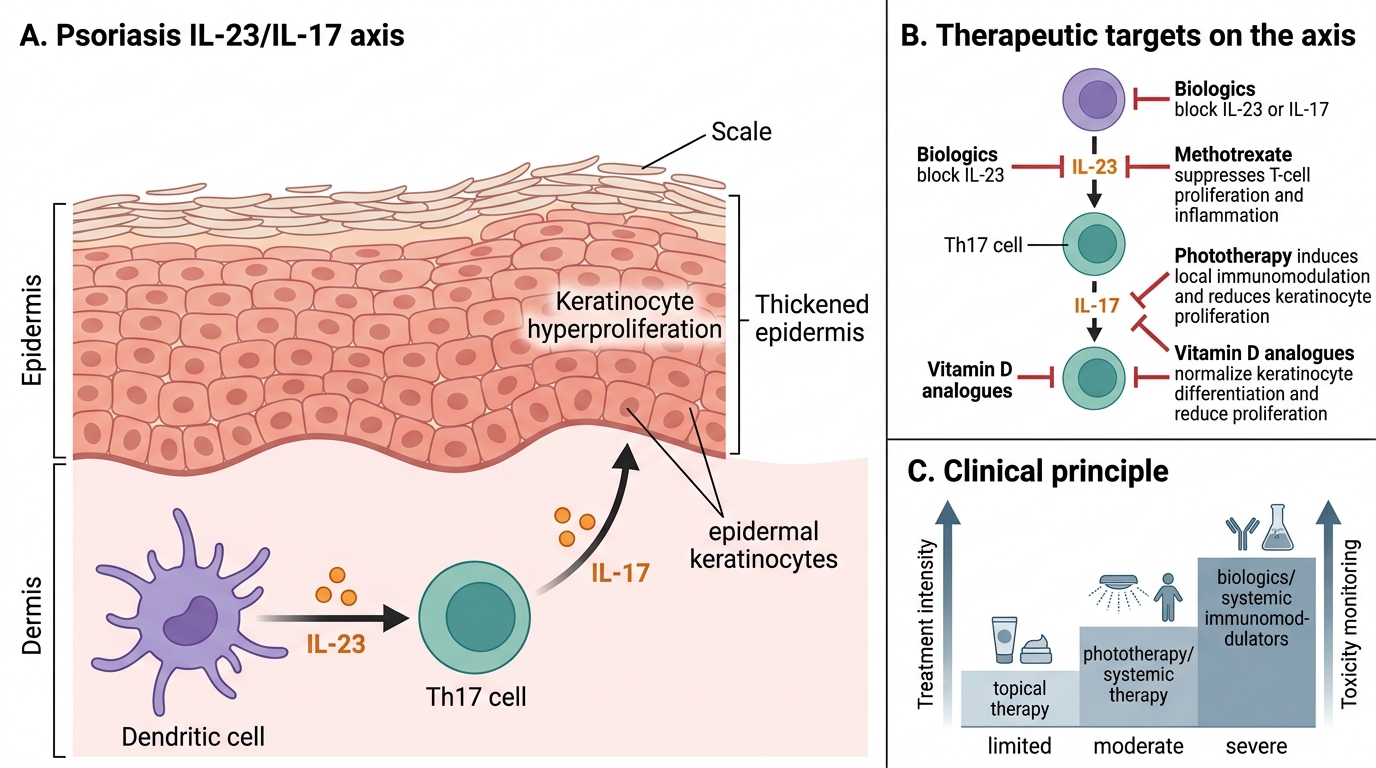
Rational prescribing flows directly from mechanism, so it is worth briefly revisiting why each class of treatment works before deciding which to use. The core abnormality in psoriasis is immune-driven: activation of the IL-23/IL-17 axis drives T-helper-17 lymphocytes and a cytokine cascade that makes keratinocytes proliferate too rapidly and incompletely, producing scale, while inflammatory mediators dilate dermal capillaries to produce erythema. Each therapeutic class intervenes at a recognisable point on this pathway, and seeing the link makes the choices logical rather than arbitrary. Topical vitamin D analogues normalise the deranged keratinocyte differentiation; topical and systemic agents that suppress inflammation dampen the cytokine drive; phototherapy induces local immunosuppression and apoptosis of activated T-cells in the skin; methotrexate and other systemic agents reduce the hyperproliferation and inflammation more broadly; and biologic agents block specific cytokines (TNF-α, IL-17, or IL-23) at the very heart of the cascade.
Psoriasis IL-23/IL-17 Axis and Treatment Targets
The practical point is that treatment intensity should match disease burden, because the more powerful the intervention on this axis, the greater its potential toxicity — which is exactly why severity assessment, considered next, governs the choice of tier.
Severity Assessment and Treatment Stratification
Psoriasis Severity Assessment and Treatment Stratification
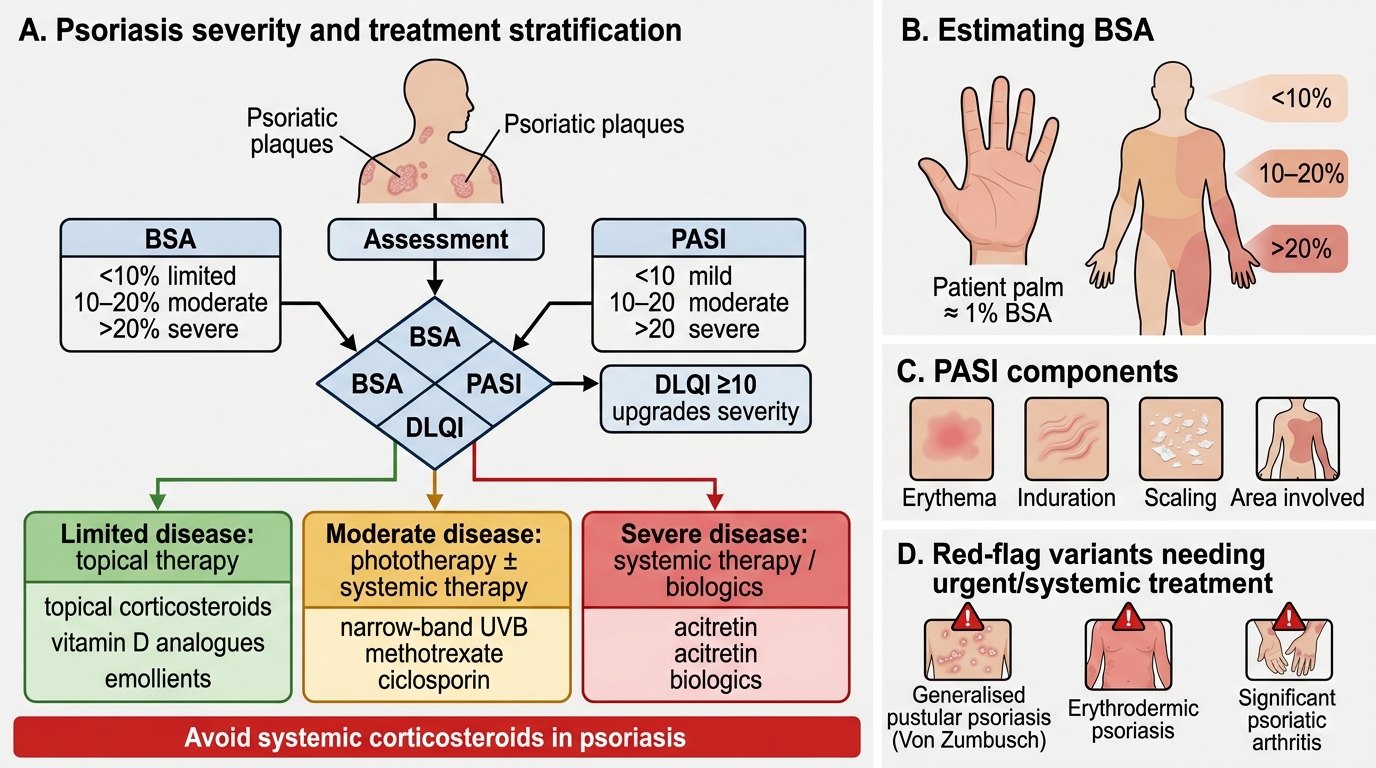
Choosing a treatment tier rationally depends on assessing severity systematically rather than by impression, using three complementary measures and a short list of red-flag variants. The first is body surface area (BSA), estimated roughly with the patient's palm as about 1% of their skin; conventionally, limited disease is under 10% BSA, moderate disease is 10–20%, and severe disease exceeds 20%. The second is the PASI (Psoriasis Area and Severity Index), a composite score of erythema, induration, scaling, and area, where mild is below 10, moderate is 10–20, and severe is above 20. The third is the DLQI, the quality-of-life measure introduced earlier, which can upgrade a patient's effective severity when the psychological burden is high even if the skin area is modest. Alongside these, certain variants demand urgent or systemic treatment regardless of area: generalised pustular psoriasis (Von Zumbusch), erythrodermic psoriasis, and significant psoriatic arthritis.
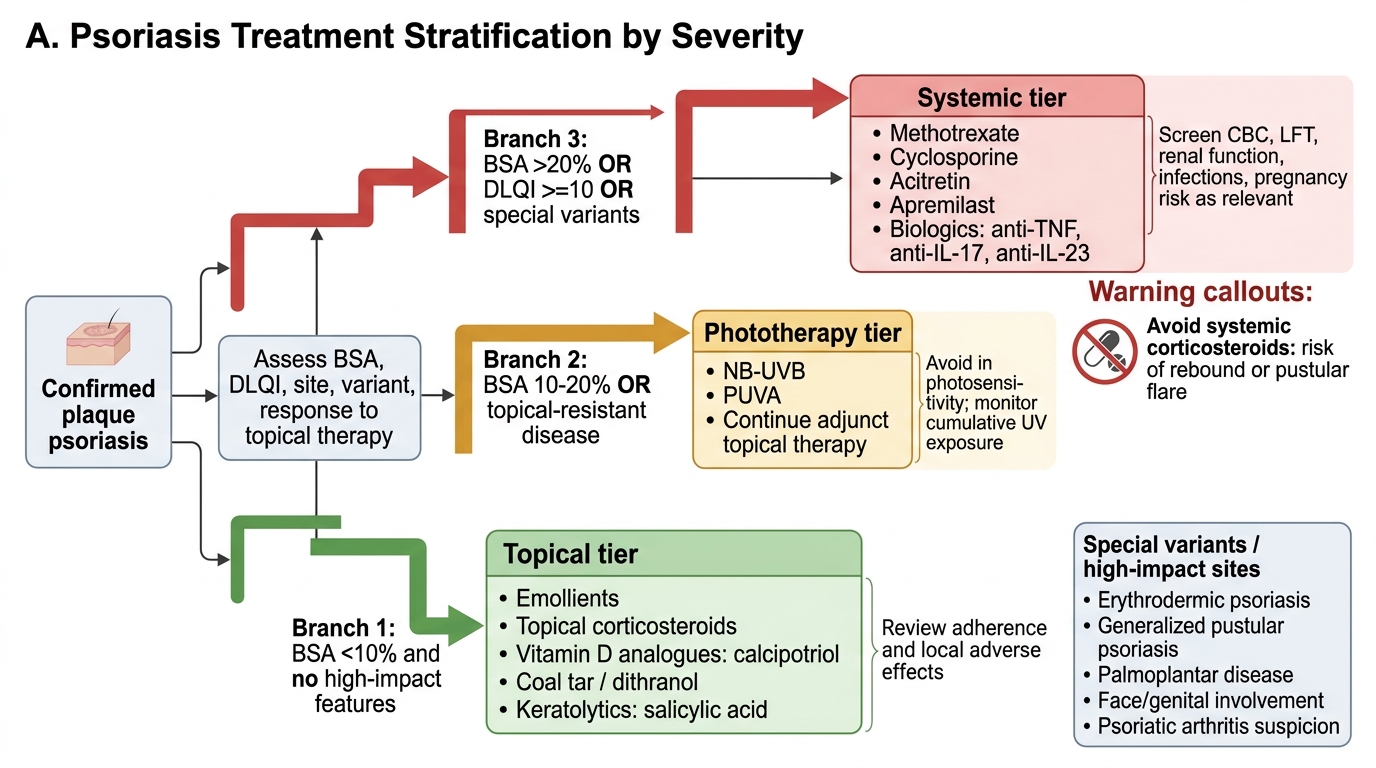
Psoriasis Treatment Stratification Decision Tree
The stratification follows directly:
- Limited disease (<10% BSA, low DLQI) → topical therapy.
- Moderate disease (10–20% BSA, or topical-resistant) → phototherapy, sometimes with systemic agents.
- Severe disease (>20% BSA, DLQI ≥10, or special variants) → systemic therapy or biologics, with urgent inpatient care for pustular/erythrodermic emergencies.
SELF-CHECK
A patient has plaques covering about 15% of his body surface area and a DLQI of 12, with no pustular or erythrodermic features. Which treatment tier is most appropriate as a starting point?
A. Topical therapy alone, since the disease is mild
B. Phototherapy (narrowband UVB), with consideration of systemic agents, since this is moderate disease with significant quality-of-life impairment
C. Immediate systemic corticosteroids to clear the skin rapidly
D. No treatment is needed below 20% body surface area
Reveal Answer
Answer: B. Phototherapy (narrowband UVB), with consideration of systemic agents, since this is moderate disease with significant quality-of-life impairment
A BSA of 10–20% defines moderate psoriasis, and a DLQI of 12 indicates significant quality-of-life impairment (≥10) — together these place the patient in the moderate tier, for which narrowband UVB phototherapy (with consideration of systemic agents if needed) is appropriate. Topical therapy alone is usually insufficient at this extent and impact. Systemic corticosteroids are contraindicated in psoriasis because of the rebound flare risk, and a DLQI of 12 shows treatment is clearly warranted.