Page 9 of 21
DR3.3 | Psoriasis Treatment Planning and Counselling — SDL Guide (Part 2)
Topical and Phototherapy Options
Topical and Phototherapy Options in Psoriasis
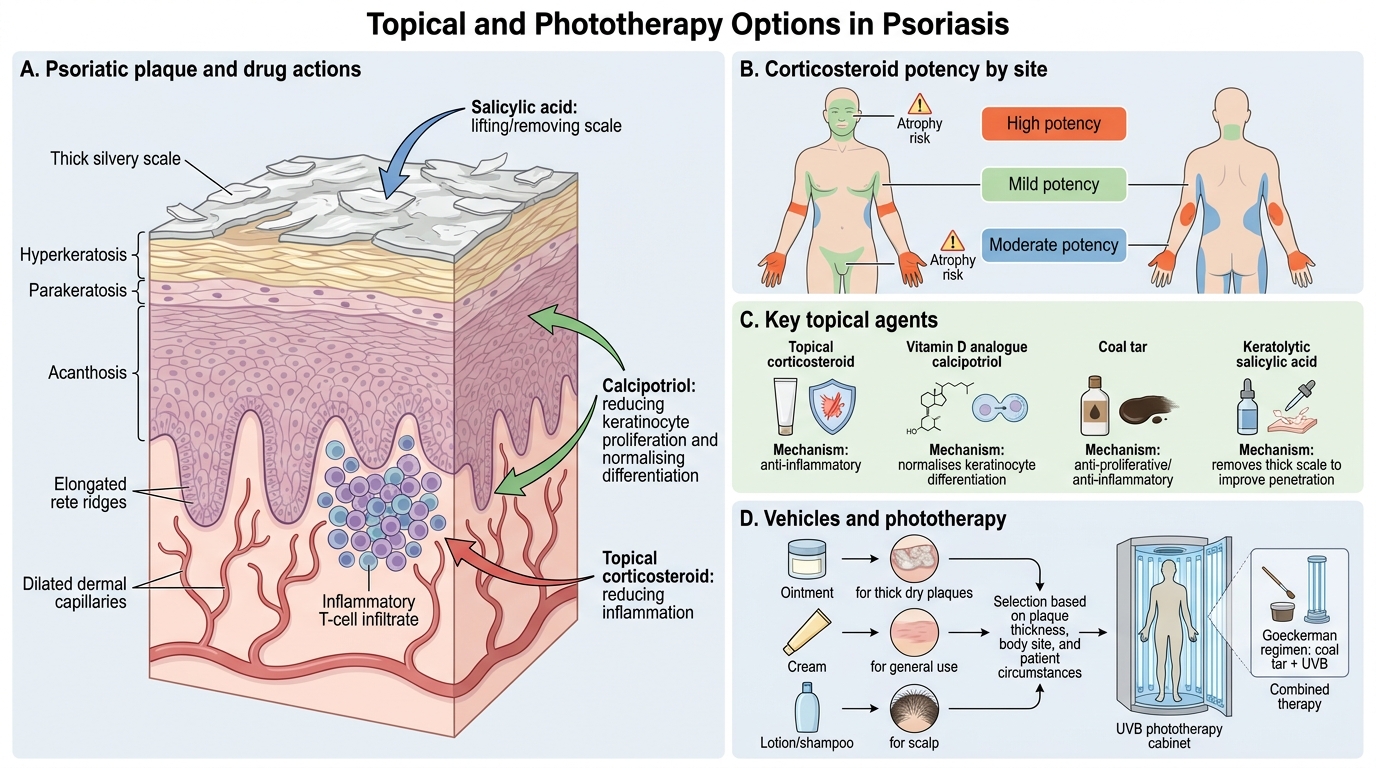
For limited and moderate disease, topical agents and phototherapy form the backbone of treatment, and selecting among them sensibly requires matching the agent to the site, the thickness of the plaque, and the patient's circumstances. Topical corticosteroids are the first-line agents for limited plaque psoriasis, with potency chosen by body region — high-potency preparations for thick plaques on elbows and knees, but only mild preparations on the face, flexures, and genitalia where the skin is thin and prone to atrophy. Calcipotriol, a vitamin D3 analogue, normalises keratinocyte differentiation and is widely used alone or in a fixed-dose combination with betamethasone. Coal tar is anti-proliferative and anti-inflammatory (the Goeckerman regimen combines it with UVB), and keratolytics such as salicylic acid are used first to remove thick scale so that active agents can penetrate. Vehicle matters too: ointments for thick dry plaques, creams for general use, lotions and shampoos for the scalp.
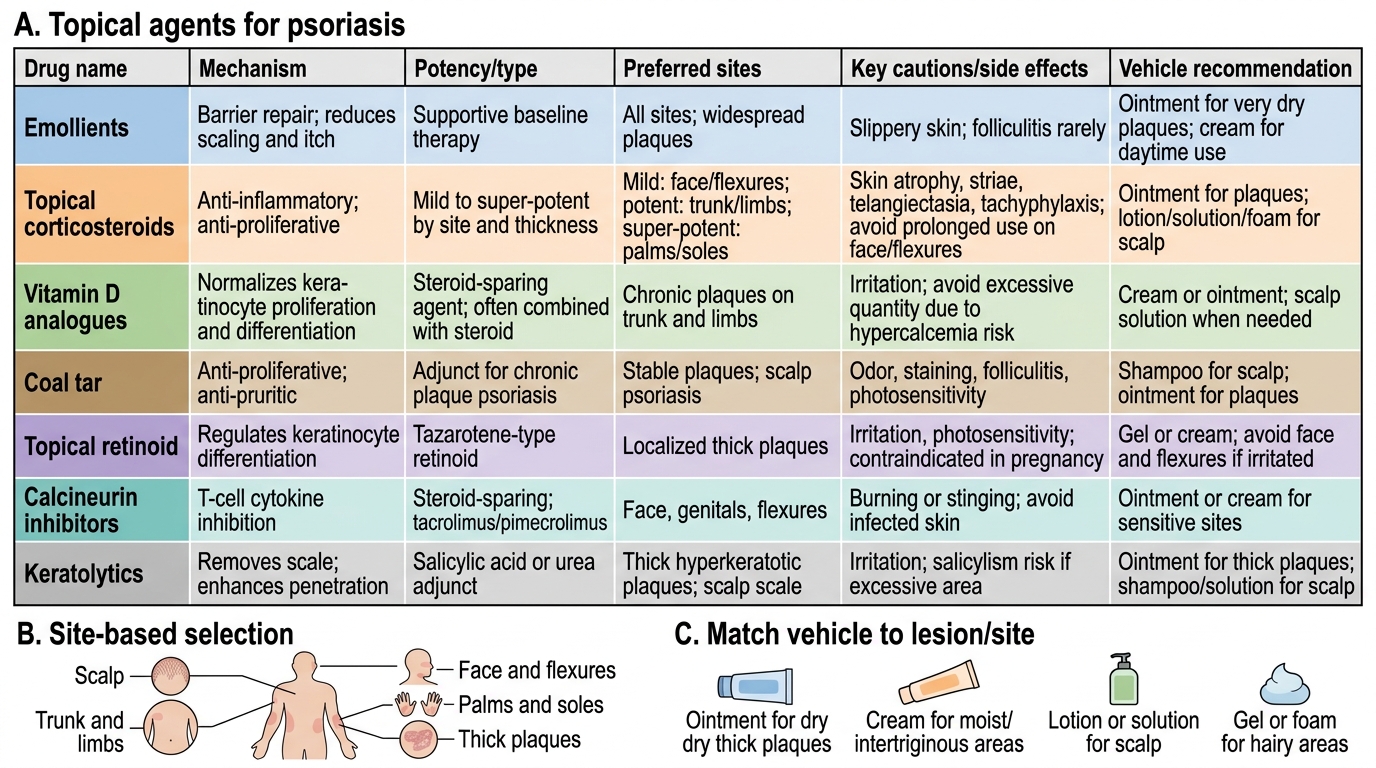
Topical Therapy for Psoriasis: Drug and Vehicle Selection
When topical therapy is insufficient or disease is more extensive, phototherapy is the next step. Narrowband UVB (NB-UVB, 311–313 nm) is the preferred first-line phototherapy: it is effective, relatively safe, and can be used in pregnancy because it involves no psoralen. PUVA (psoralen plus UVA) is reserved for selected resistant cases, as cumulative exposure carries a higher long-term risk of photocarcinogenesis. Phototherapy is typically given two to three times weekly with response assessed over several weeks.
Systemic Therapy and Contraindication of Systemic Steroids
Systemic Therapy for Psoriasis: Agents, Monitoring, and Safety Rules
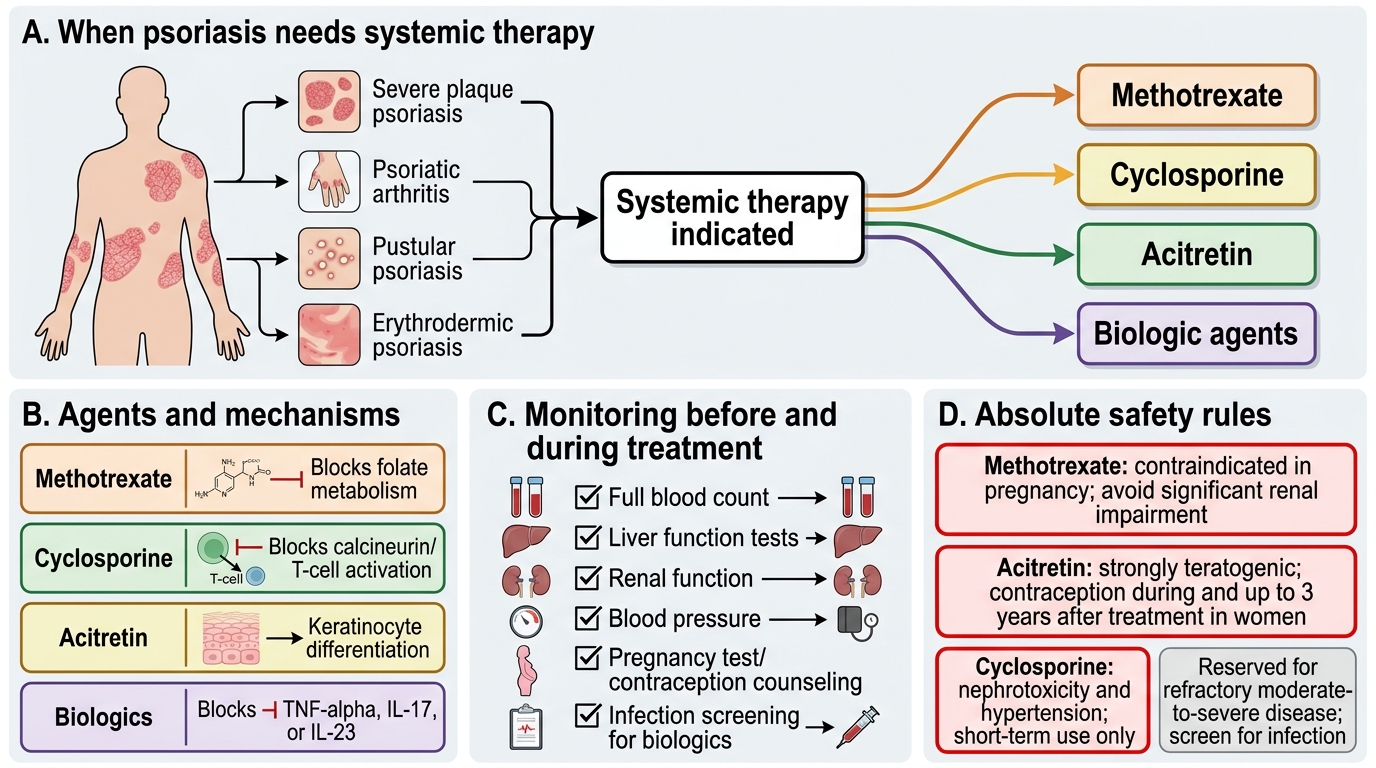
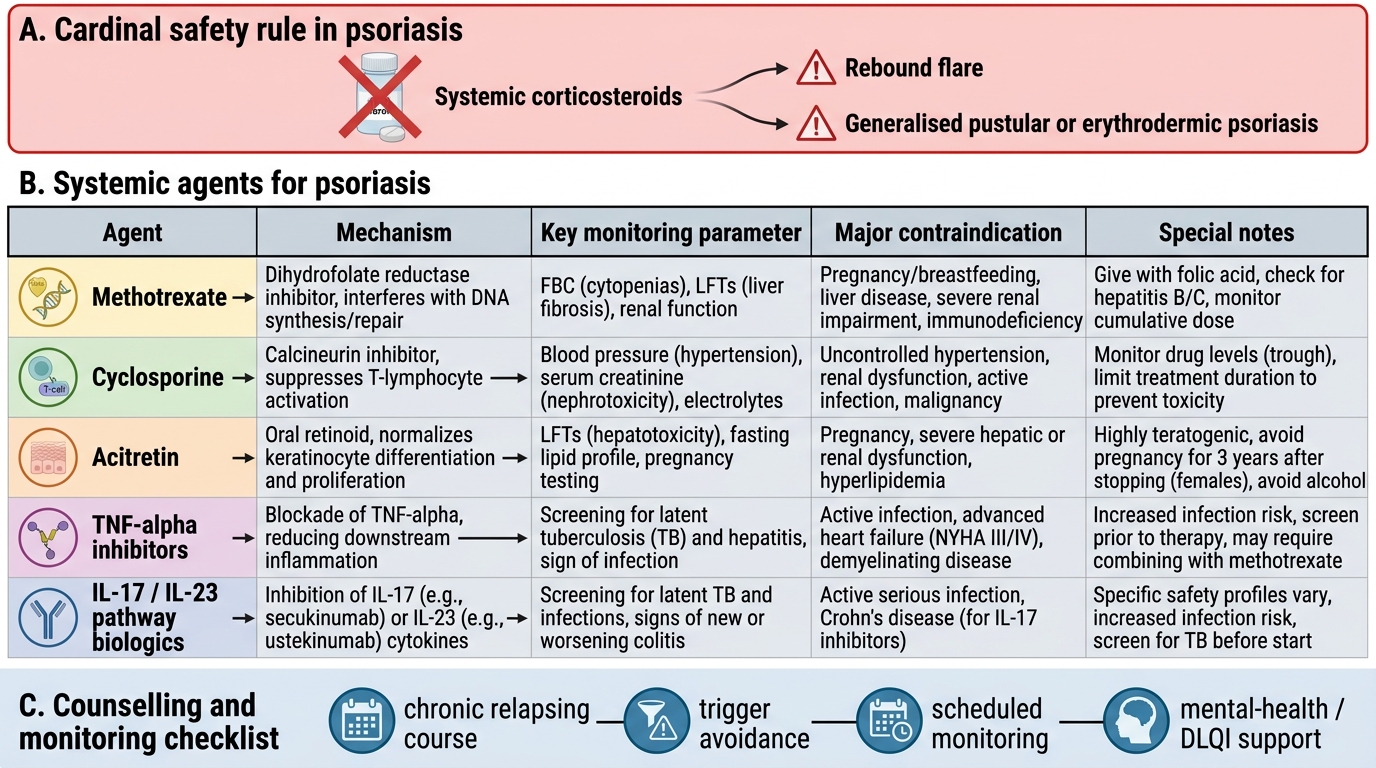
Severe, disabling, or special-variant psoriasis requires systemic therapy, and prescribing it safely depends on knowing each agent's monitoring needs and absolute rules — the most important of which is a hard contraindication that prevents a foreseeable emergency. Methotrexate, a folate antagonist, is a mainstay for severe plaque and arthritic disease; it requires folic acid supplementation and monitoring of full blood count, liver, and renal function, is teratogenic and so contraindicated in pregnancy, and should be avoided in significant renal impairment. Cyclosporine, a calcineurin inhibitor, acts quickly and is useful for short-term control or crises, but its nephrotoxicity and hypertension make it unsuitable for prolonged use. Acitretin, a systemic retinoid, is especially valuable in pustular and erythrodermic psoriasis; it is strongly teratogenic, requiring reliable contraception during and for an extended period after treatment (up to three years in women). Biologic agents that block TNF-α, IL-17, or IL-23 are reserved for refractory moderate-to-severe disease and represent targeted intervention on the cytokine axis.
Systemic Agents for Psoriasis: Safety and Monitoring
The cardinal safety rule overrides all of the above: systemic corticosteroids are contraindicated in psoriasis. Although they may transiently clear the skin, their withdrawal can precipitate a rebound flare into generalised pustular or erythrodermic psoriasis, which is potentially life-threatening — exactly what happened to the patient in our hook. This rule must be stated explicitly to the patient and to any other prescriber, because steroids may be offered innocently for unrelated complaints. Counselling, finally, ties the plan together: explain the chronicity and the remission-relapse pattern, agree on adherence and a realistic goal, identify and avoid triggers (streptococcal infection, certain drugs, trauma, stress, smoking), set up the monitoring schedule for whichever systemic agent is chosen, and offer mental-health support or referral when the DLQI signals distress.
SELF-CHECK
Which statement about systemic therapy for psoriasis is correct?
A. Systemic corticosteroids are the preferred long-term treatment for severe psoriasis
B. Methotrexate is safe in pregnancy and needs no monitoring
C. Acitretin is teratogenic and requires reliable contraception, and is particularly useful in pustular and erythrodermic psoriasis
D. Cyclosporine is the ideal agent for indefinite long-term maintenance
Reveal Answer
Answer: C. Acitretin is teratogenic and requires reliable contraception, and is particularly useful in pustular and erythrodermic psoriasis
Acitretin is a systemic retinoid that is strongly teratogenic — mandating reliable contraception during and for an extended period after treatment — and is particularly valuable in pustular and erythrodermic psoriasis. Systemic corticosteroids are contraindicated in psoriasis (rebound pustular/erythrodermic flare on withdrawal). Methotrexate is teratogenic, contraindicated in pregnancy, and needs FBC/LFT/renal monitoring. Cyclosporine's nephrotoxicity and hypertension make it unsuitable for prolonged maintenance.
Self-Assessment — Treatment Planning and Counselling
Consolidate this module by rehearsing the whole clinical task — assess, stratify, choose, and counsel — as a single integrated performance, because in practice and in examinations these steps are judged together. A competent clinician can take a described patient, estimate severity from BSA and DLQI, place them in the correct tier, name an appropriate agent with its key monitoring or contraindication, identify the contraindicated systemic steroid, and deliver a short, honest counselling message about chronicity and adherence. Work through the prompts below by imagining a real consultation: picture the patient in front of you, decide what you would prescribe and why, and rehearse the exact words you would use to explain that psoriasis is controllable but not curable. The ability to do all of this together, smoothly and safely, is the true measure of competence in managing psoriasis.
Self-check prompts:
- For a patient with 8% BSA and DLQI 4, which tier and which first-line agent?
- Name the contraindicated systemic agent in psoriasis and the consequence of using it.
- What three monitoring tests would you arrange before and during methotrexate therapy?
- How would you explain, in two sentences, why the plaques returned after a good response?
- Which phototherapy would you choose for a pregnant patient, and why?
SELF-CHECK
A patient with stable plaque psoriasis says a friend's doctor gave her oral steroids that 'cleared everything in a week' and asks you to prescribe the same. What is the best response?
A. Prescribe the oral steroids, as rapid clearance is the goal
B. Explain that systemic steroids are avoided in psoriasis because stopping them can trigger a severe pustular or erythrodermic flare, and offer a safe alternative plan
C. Refuse without explanation and end the consultation
D. Prescribe steroids but only for a single day to avoid any risk
Reveal Answer
Answer: B. Explain that systemic steroids are avoided in psoriasis because stopping them can trigger a severe pustular or erythrodermic flare, and offer a safe alternative plan
The correct, patient-centred response is to explain the specific danger — that systemic corticosteroids can clear psoriasis transiently but their withdrawal can precipitate a life-threatening generalised pustular or erythrodermic flare — and then to offer a safe, effective alternative appropriate to her severity (topical, phototherapy, or a non-steroid systemic agent). This both keeps the patient safe and respects her concern by addressing it directly rather than dismissing it.
CLINICAL PEARL
Match the treatment to the severity and the message to the disease. Limited disease needs topicals; moderate disease needs phototherapy (narrowband UVB, safe even in pregnancy); severe or special-variant disease needs a non-steroid systemic agent or a biologic. The one rule that never bends: never give a systemic corticosteroid, because its withdrawal can flip stable psoriasis into a pustular or erythrodermic emergency. And remember that the most therapeutic thing you can say is the truth — psoriasis is controllable, not curable; relapses are expected, not failures — because the patient who understands this stays on a safe plan instead of chasing a dangerous quick fix.