Page 14 of 21
DR2.1 | Vitiligo Diagnosis and Treatment Planning — SDL Guide
Learning Objectives
- Describe the morphology of vitiligo as depigmented (not merely hypopigmented) macules and its typical distribution and types.
- Outline the autoimmune etiopathogenesis of vitiligo and its associated systemic autoimmune diseases.
- Use clinical examination and Wood's lamp to diagnose vitiligo.
- Differentiate vitiligo from other hypopigmented and depigmented lesions, especially leprosy, pityriasis versicolor, and pityriasis alba.
- Devise a stage- and extent-appropriate treatment plan and counsel the patient about the chronic, autoimmune nature of the disease.
INSTRUCTIONS
Vitiligo is a common, cosmetically and psychologically distressing pigmentary disorder, and in the Indian context its correct diagnosis carries a special responsibility: it must never be confused with leprosy, a treatable infection whose hypopigmented patches can superficially resemble it but are anaesthetic. This module teaches you to recognise the depigmented macules of vitiligo, to confirm them with simple bedside tools, to separate vitiligo rigorously from the other causes of pale patches, and to plan treatment by extent and stability. The single most important habit it instils is to test sensation on every pale patch — because missing an anaesthetic patch means missing leprosy.
References
- IADVL Textbook of Dermatology, Section on Disorders of Pigmentation — Vitiligo (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & STD, Ch. on Vitiligo and Pigmentary Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old college student is brought by her anxious mother to the OPD with a few well-defined white patches on her hands and around her mouth. The family is distraught — a neighbour has told them it is leprosy, and the social consequences of that word in their community are devastating. You examine the patches carefully. They are not merely pale; they are milky-white, completely depigmented, with sharp borders. You test light touch across each patch with a wisp of cotton: sensation is entirely normal. Under a Wood's lamp the patches light up a bright chalky blue-white. This is vitiligo, an autoimmune loss of pigment cells — not leprosy, and not contagious. The relief on the family's faces is immediate. That single careful examination — looking at the colour, testing the sensation, using the lamp — has corrected a diagnosis that would otherwise have shadowed this young woman's life.
WHY THIS MATTERS
Pale patches on the skin are an extremely common presentation, and in India the stakes of getting the diagnosis right are unusually high. The chief differential — leprosy — is an infectious, treatable, and historically stigmatised disease whose early lesions are hypopigmented and anaesthetic; to mistake leprosy for vitiligo is to miss a curable infection, while to mistake vitiligo for leprosy is to inflict needless stigma. Beyond leprosy, you must distinguish vitiligo from fungal infection (pityriasis versicolor), from the common childhood patches of pityriasis alba, and from birthmarks and post-inflammatory change. Vitiligo itself, though benign, carries a heavy psychosocial burden and is linked to other autoimmune diseases that you should screen for. Competence here protects patients from both medical and social harm.
RECALL
Recall from your histology that melanocytes reside in the basal layer of the epidermis, where they manufacture melanin in melanosomes and transfer it to surrounding keratinocytes; the amount of melanin determines skin and hair colour. Distinguish carefully between two words you will use throughout this module: hypopigmentation means reduced melanin with melanocytes still present, whereas depigmentation means complete loss of melanin because the melanocytes themselves are gone. Recall, too, the basic idea of autoimmunity — the immune system attacking the body's own cells — and the clinical fact that leprosy, caused by Mycobacterium leprae, characteristically produces a patch that is both hypopigmented and, importantly, anaesthetic. These three anchors — melanocyte biology, the hypo-versus-depigmentation distinction, and the anaesthetic leprosy patch — underpin everything that follows.
Clinical Morphology of Vitiligo — Depigmentation vs Hypopigmentation
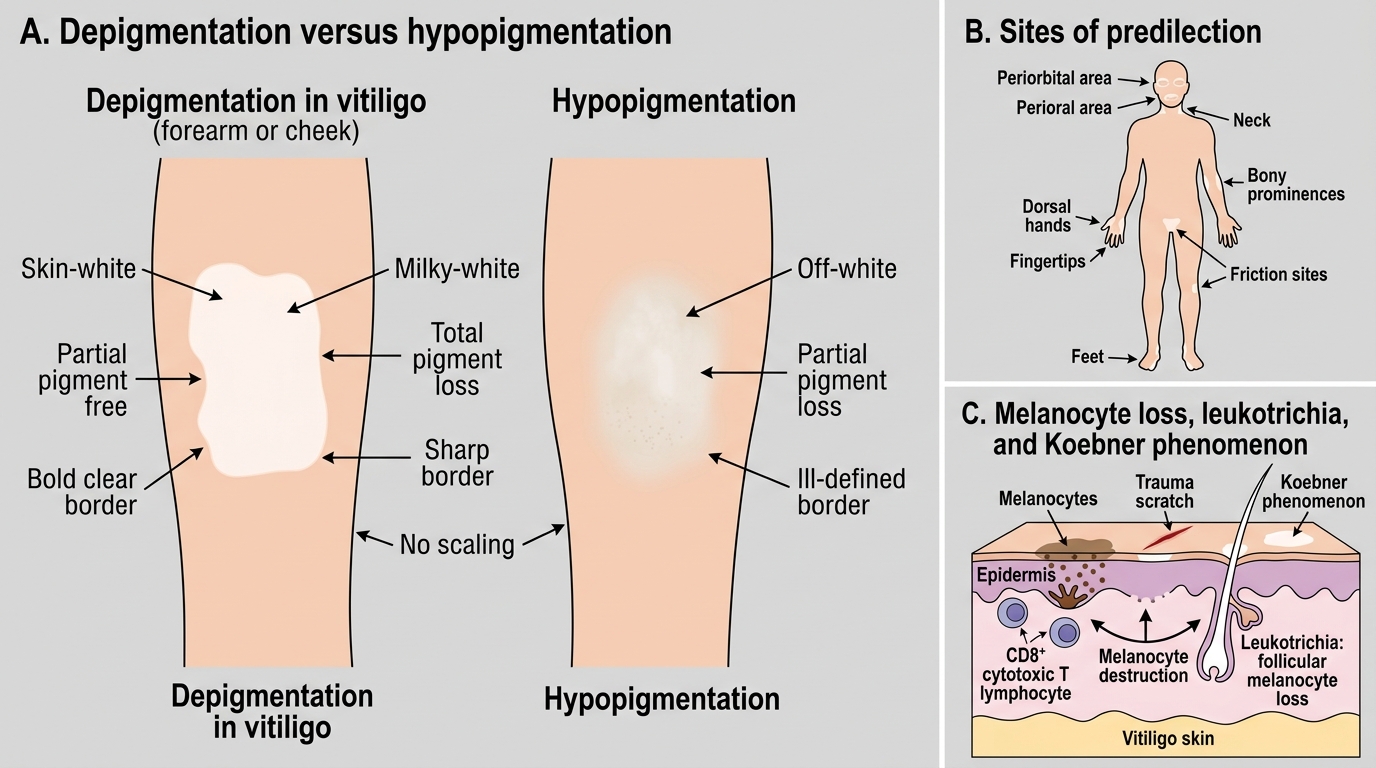
Clinical Morphology of Vitiligo
The recognition of vitiligo begins with a precise observation that the competency itself hinges upon: vitiligo lesions are depigmented, not merely hypopigmented. Because the melanocytes are destroyed, the affected skin loses melanin completely and appears milky- or chalk-white with sharply defined borders, in contrast to the off-white, ill-defined paleness of conditions where melanocytes survive but make less pigment. This distinction — milky-white and total versus dull and partial — is the first and most useful discriminator at the bedside. Vitiligo has characteristic sites of predilection: the face (especially around the eyes and mouth), the neck, the dorsa of the hands and the fingertips, the feet, the genitalia, and bony prominences and sites of friction. White hairs within a patch (leukotrichia) indicate involvement of follicular melanocytes and predict a poorer response to medical treatment. The Koebner phenomenon — new depigmented patches at sites of trauma — also occurs.
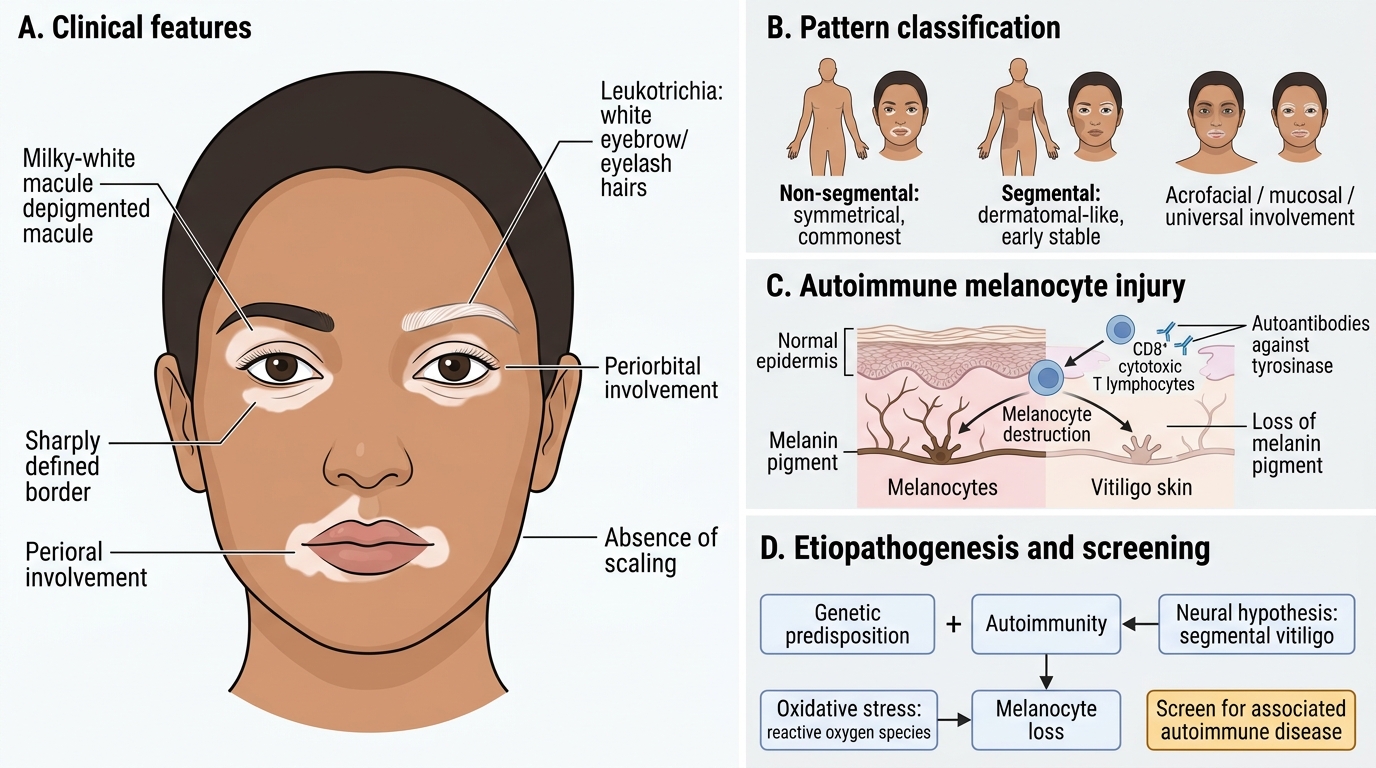
Vitiligo: Clinical Features, Patterns, and Pathogenesis
Vitiligo is classified by pattern, which carries prognostic meaning:
- Non-segmental (generalised) — the commonest form, often symmetrical, tending to progress, and associated with autoimmunity.
- Segmental — confined to one dermatomal-like region, usually of early onset, which characteristically becomes stable quickly.
- Acrofacial, mucosal, and universal — describing acral/facial, mucosal, and near-complete involvement respectively.
Etiopathogenesis of Vitiligo
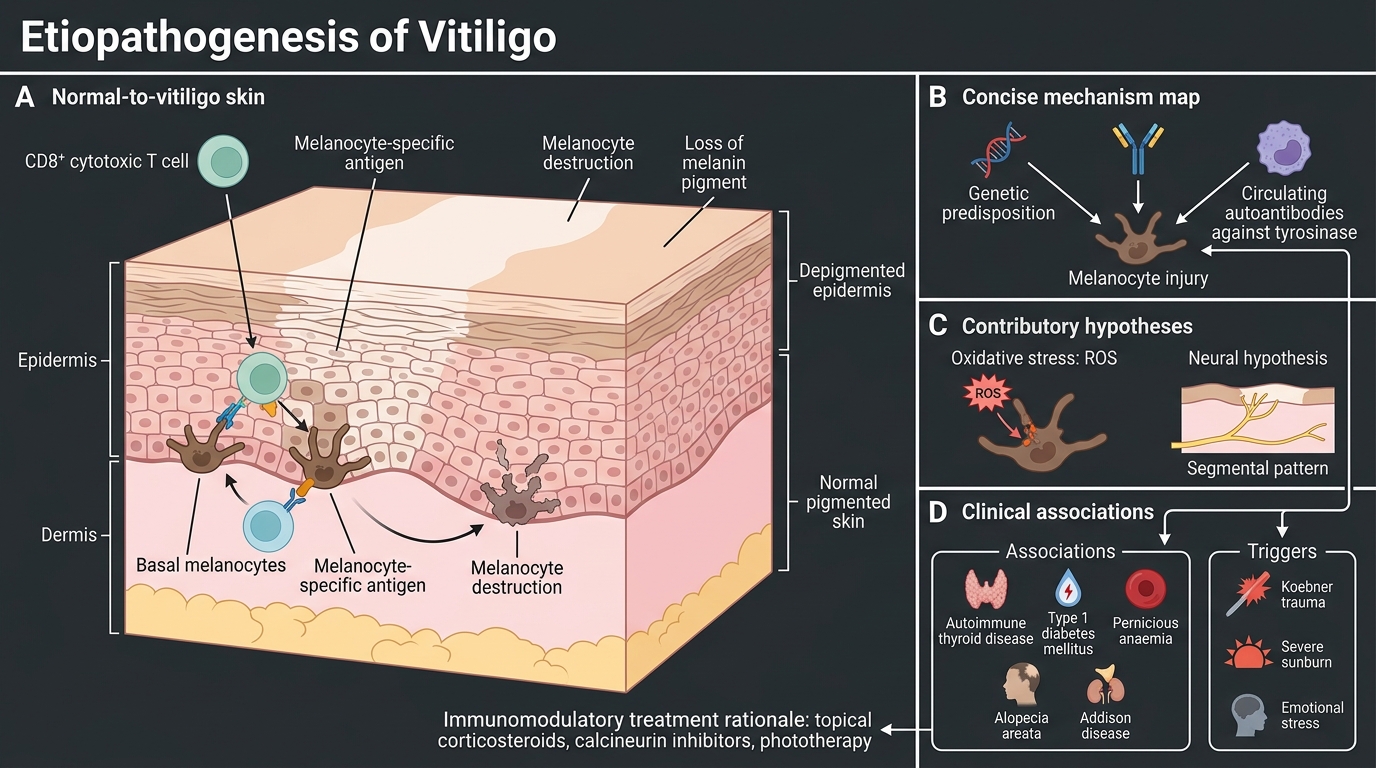
Etiopathogenesis of Vitiligo
Vitiligo is best understood as an autoimmune disease, and grasping its mechanism explains both its associations and the rationale for treatment. The dominant model is that CD8+ cytotoxic T-lymphocytes target melanocyte-specific antigens and destroy the pigment cells, supported by the presence of circulating autoantibodies against melanocyte proteins such as tyrosinase. A genetic predisposition is well recognised, and the disease clusters with other autoimmune conditions, which is why a new diagnosis of vitiligo should prompt a targeted screen. Additional contributory hypotheses — an oxidative-stress model in which accumulated reactive oxygen species damage melanocytes, and a neural hypothesis particularly invoked for the segmental type — complement rather than replace the autoimmune account. Recognised triggers can precipitate or extend disease in a predisposed person.
Associations and triggers worth knowing:
- Associated autoimmune diseases — autoimmune thyroid disease (the commonest), type 1 diabetes mellitus, pernicious anaemia, alopecia areata, and Addison's disease.
- Triggers — physical trauma (Koebner), severe sunburn, and emotional stress.
- A family history of vitiligo or of autoimmune disease is common.
This autoimmune basis is the reason that immunomodulatory treatments — topical corticosteroids, calcineurin inhibitors, and phototherapy — form the backbone of medical therapy.
Diagnosis of Vitiligo — Clinical Examination and Wood's Lamp
The diagnosis of vitiligo is overwhelmingly clinical, resting on careful inspection supplemented by one simple and powerful bedside tool, and a competent examination follows a reliable routine. On inspection, vitiligo presents as sharply demarcated, milky-white depigmented macules and patches with no scaling and no surface change, and — critically — with normal sensation, a feature you must actively test to exclude leprosy. The single most useful instrument is the Wood's lamp (long-wave ultraviolet light viewed in a darkened room): vitiligo patches show a striking bright chalky or blue-white accentuation, appearing more obvious and often larger than in daylight, which is especially valuable in fair-skinned patients in whom the lesions may be hard to see. The lamp also helps separate vitiligo from mimics that fluoresce differently. Because vitiligo is autoimmune, the assessment should include a screen for associated disease.
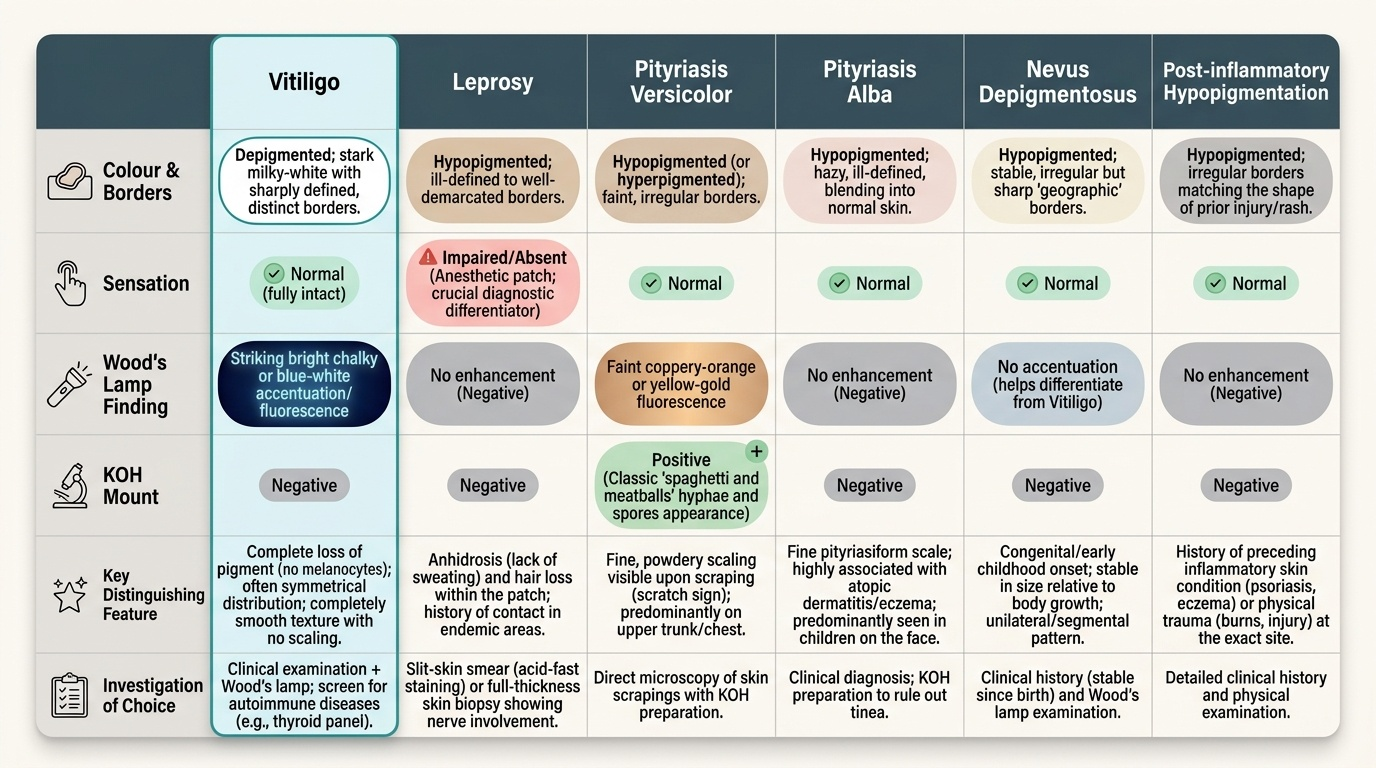
Provided image
A practical diagnostic routine:
- Inspect the colour and borders — milky-white and sharply defined favours vitiligo.
- Test sensation on every patch — normal in vitiligo, impaired in leprosy.
- Use the Wood's lamp — bright blue-white accentuation in vitiligo.
- Screen for associations — thyroid function tests and antibodies, fasting glucose.
- Biopsy is rarely needed but shows absent melanocytes; KOH mount excludes pityriasis versicolor.