Page 15 of 21
DR2.1 | Vitiligo Diagnosis and Treatment Planning — SDL Guide (Part 2)
Differential Diagnosis — Hypopigmented and Depigmented Lesions
Vitiligo Versus Leprosy: Pale Patch Bedside Comparison
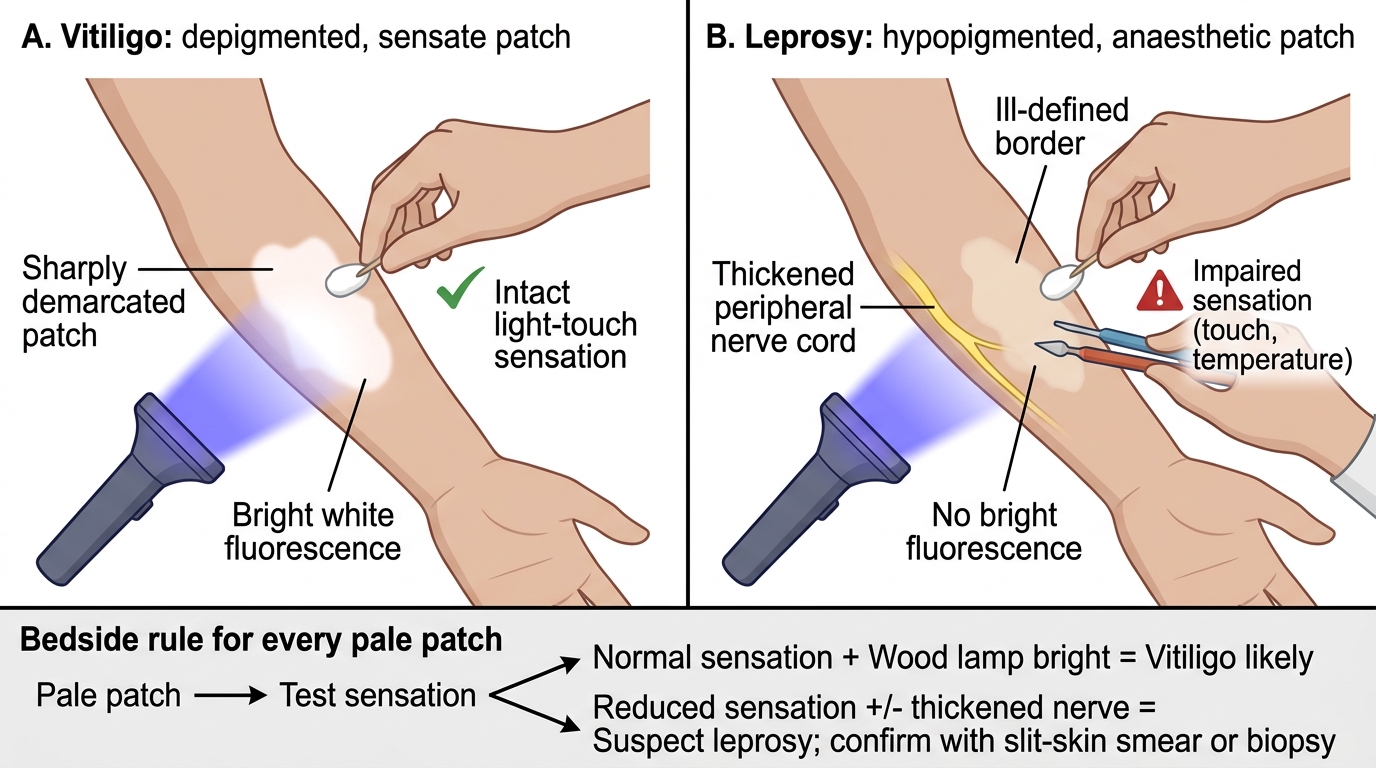
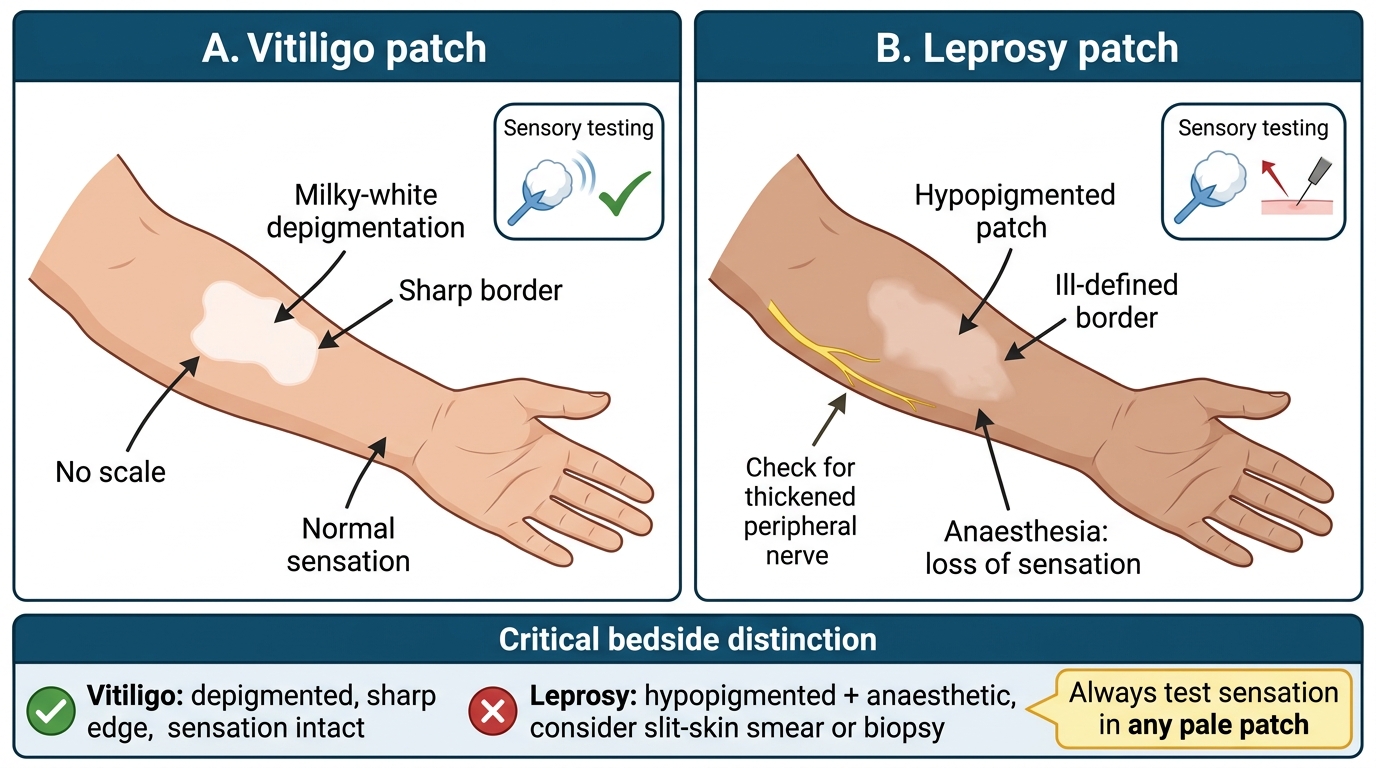
Constructing the differential for a pale patch is the heart of this competency, and it must be done with discipline because the conditions differ in colour, sensation, fungal status, and — most consequentially — in whether they represent a treatable infection. The single most important rule is to test sensation on every hypopigmented patch, because leprosy is hypopigmented and ANAESTHETIC: a Mycobacterium leprae lesion typically shows reduced (not complete) pigment loss, impaired light-touch and temperature sensation, and sometimes a thickened peripheral nerve, and unlike vitiligo it does not light up brightly under Wood's lamp. Missing the anaesthesia is the classic, harmful error. The other common mimics each have a discriminating test or history that separates them cleanly from the milky-white, normally-sensate, Wood's-lamp-bright lesion of vitiligo.
Vitiligo Versus Leprosy: Pale Patch Bedside Comparison
The key differentials:
- Leprosy — hypopigmented AND anaesthetic, possibly with a thickened nerve; confirmed by slit-skin smear or biopsy. The critical differential in India.
- Pityriasis versicolor — hypopigmented (or hyperpigmented) scaly macules; KOH mount positive (hyphae and spores), Wood's lamp shows golden-yellow fluorescence.
- Pityriasis alba — poorly defined hypopigmented patches with fine scale on the face of atopic children; not depigmented.
- Nevus depigmentosus — congenital, stable, non-progressive hypopigmented patch present from birth.
- Post-inflammatory hypopigmentation — follows eczema, psoriasis, or burns; matches the shape of the prior lesion.
- Chemical leukoderma — depigmentation from occupational/contact chemicals (most often catechols in rubber and adhesives, such as para-tertiary butyl catechol; also topical monobenzyl ether of hydroquinone); suggested by a relevant exposure history and a distribution matching the contact.
SELF-CHECK
A 30-year-old man has a single pale patch on his forearm. Which single bedside finding most urgently distinguishes leprosy from vitiligo and must always be checked?
A. Whether the patch shows bright blue-white accentuation under Wood's lamp
B. Whether the patch is anaesthetic (loss of light-touch/temperature sensation), which points to leprosy rather than vitiligo
C. Whether the patch is itchy
D. Whether the patch has a herald-patch appearance
Reveal Answer
Answer: B. Whether the patch is anaesthetic (loss of light-touch/temperature sensation), which points to leprosy rather than vitiligo
The decisive and always-mandatory test is for SENSATION: a leprosy patch is hypopigmented AND anaesthetic (impaired light touch and temperature, sometimes with a thickened nerve), whereas a vitiligo patch is depigmented but has entirely normal sensation. Missing the anaesthesia means missing a treatable infection. Wood's lamp accentuation supports vitiligo but does not replace sensory testing; itch and herald patches are not relevant to this distinction.
Treatment Planning for Vitiligo
Stepped Treatment Planning for Vitiligo
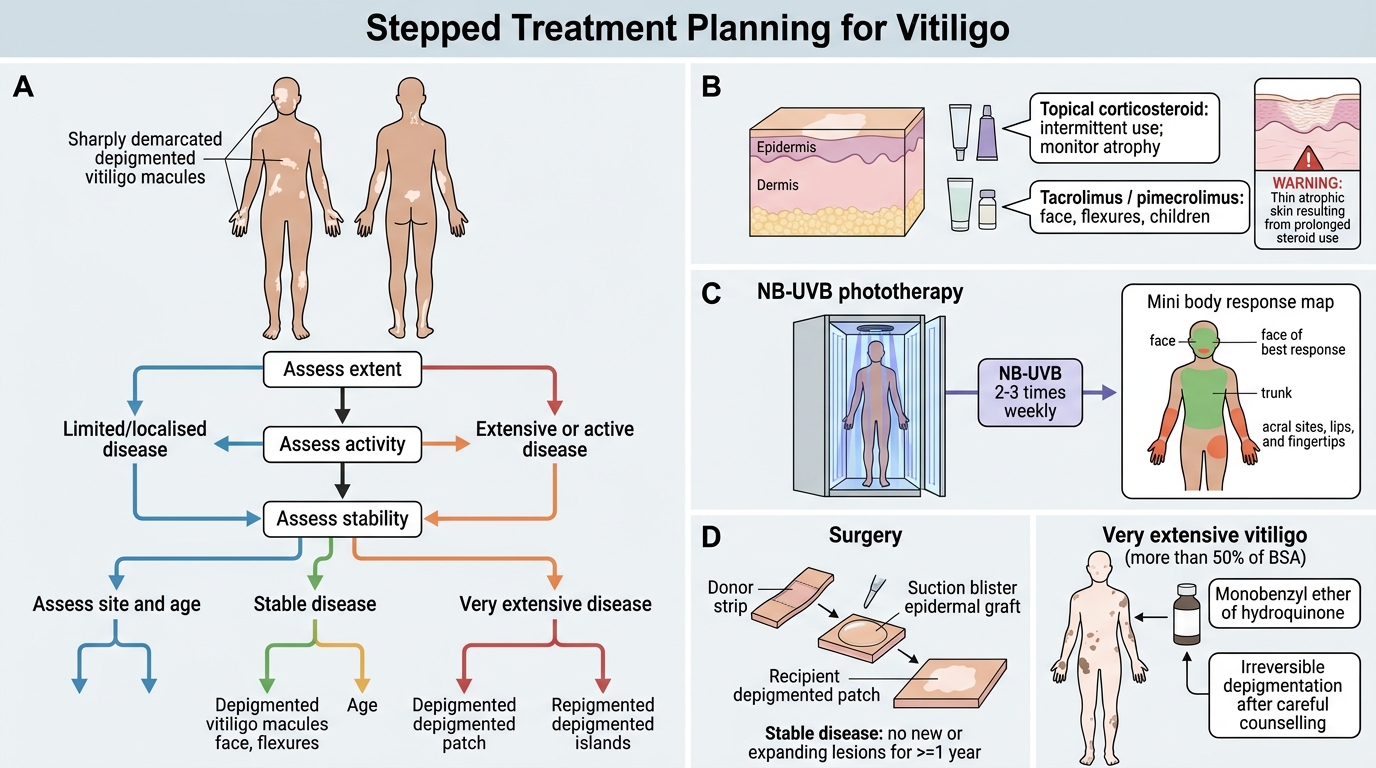
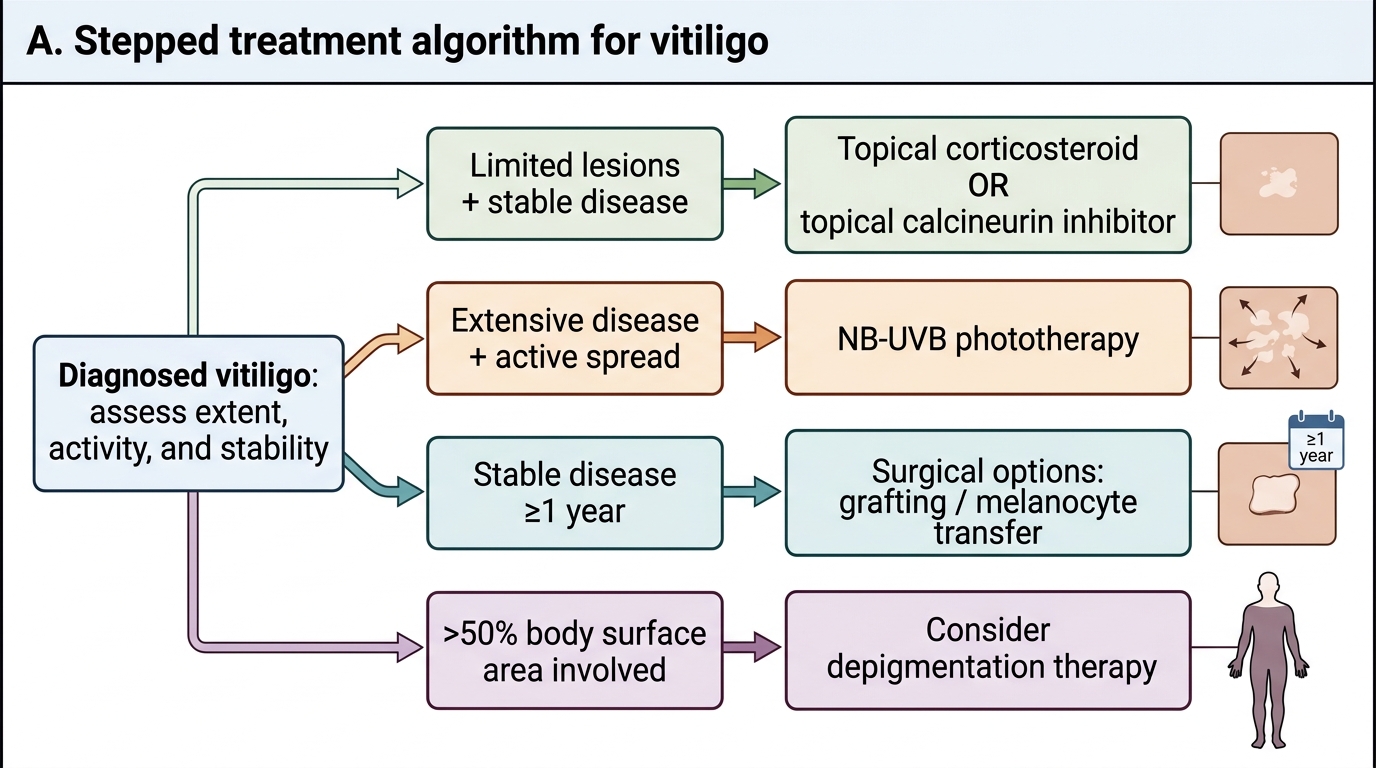
Treatment planning in vitiligo is individualised by the extent, activity, and stability of disease, and a clear framework lets you offer realistic options while counselling honestly about a chronic autoimmune condition with no universal cure. For limited or localised disease, first-line medical therapy is a topical corticosteroid (used intermittently to limit atrophy) or a topical calcineurin inhibitor such as tacrolimus or pimecrolimus, which is preferred on the face and flexures and in children because it avoids steroid-induced atrophy. For extensive or active disease, narrowband UVB (NB-UVB) phototherapy is the first-line option, given two to three times weekly with response judged over several months; the face and trunk respond best, while acral sites, lips, and fingertips respond poorly. Surgical options — such as split-thickness or suction-blister epidermal grafting and melanocyte-keratinocyte transplantation — are reserved for stable disease, defined per IADVL guidance as no new lesions and no expansion of existing lesions for at least one year. For very extensive vitiligo (more than about 50% of the body surface) where repigmentation is impractical, depigmentation of the remaining normal skin (using monobenzyl ether of hydroquinone) may be offered as an irreversible cosmetic option after careful counselling.
Stepped Treatment Algorithm for Vitiligo
Counselling is integral to the plan:
- Explain the autoimmune, chronic nature and that treatment aims at repigmentation and control, not guaranteed cure.
- Stress sun protection of depigmented skin, which has no melanin photoprotection.
- Screen for and manage associated autoimmune disease (thyroid in particular).
- Address the psychosocial impact and correct the common, harmful belief that vitiligo is leprosy or is contagious.
SELF-CHECK
A patient with vitiligo asks about surgical grafting to restore colour. What is the essential prerequisite before offering a surgical option?
A. The disease must be actively spreading so that grafts can keep pace
B. The disease must be stable — no new lesions and no expansion of existing lesions for at least one year (per IADVL guidance)
C. The patient must first have failed depigmentation therapy
D. Surgery can be offered at any time regardless of disease activity
Reveal Answer
Answer: B. The disease must be stable — no new lesions and no expansion of existing lesions for at least one year (per IADVL guidance)
Surgical repigmentation procedures (such as epidermal grafting or melanocyte-keratinocyte transplantation) require STABLE vitiligo — defined per IADVL guidance as no new lesions and no expansion of existing lesions for at least one year. Operating on active, spreading disease risks Koebnerisation and graft failure. Depigmentation therapy is a separate option reserved for very extensive disease, not a prerequisite for surgery.
Self-Assessment — Vitiligo Recognition and Differential
Consolidate this competency by rehearsing the complete reasoning from pale patch to plan, keeping the leprosy differential at the front of your mind throughout, because that vigilance is the safest habit this module can give you. A competent student can describe vitiligo as depigmented (milky-white) rather than hypopigmented, demonstrate the diagnostic routine of inspecting colour, testing sensation, and using the Wood's lamp, build a disciplined differential that always excludes leprosy by sensory testing, and devise a treatment plan stratified by extent and stability while counselling the patient compassionately. Work through the prompts below by picturing real patients and reasoning aloud; if you can explain why you test sensation on every patch and why stability governs surgery, you have grasped the essentials.
Self-check prompts:
- Why is vitiligo described as depigmented rather than hypopigmented, and what does the Wood's lamp show?
- Which single test must be performed on every hypopigmented patch, and what diagnosis are you excluding?
- How does the Wood's lamp finding of vitiligo differ from that of pityriasis versicolor?
- What is the first-line treatment for limited facial vitiligo, and why is a calcineurin inhibitor preferred there?
- What stability criterion must be met before offering surgical treatment?
CLINICAL PEARL
On every pale patch, do three things before you say a word about the diagnosis: look at the colour (milky-white and sharply bordered favours vitiligo; dull and ill-defined favours a hypopigmenting cause), test the sensation (normal in vitiligo, impaired in leprosy — never skip this), and shine the Wood's lamp (bright blue-white accentuation in vitiligo, golden-yellow in pityriasis versicolor). The anaesthetic patch is the one that changes everything: it converts a cosmetic pigment problem into a treatable, notifiable infection. And when you reassure a frightened family that this is vitiligo and not leprosy, you are treating the social disease as much as the skin.