Page 1 of 35
DR10.1 | Syndromic Case Management of Sexually Transmitted Diseases — SDL Guide
Learning Objectives
- Explain the rationale for syndromic case management of sexually transmitted diseases in the Indian primary-care setting.
- Identify the seven NACO syndromes and the clinical presentation that triggers each.
- Select the correct NACO colour-coded pre-packed kit for a given syndrome (per current NACO guidance).
- Apply the 4 Cs — contact tracing, counselling, compliance, condoms — as integral components of every STD consultation.
- Counsel a patient on partner management and arrange appropriate follow-up.
INSTRUCTIONS
Most patients with a sexually transmitted infection in India are first seen at a peripheral health centre where same-day laboratory confirmation is impossible and follow-up is unreliable. The syndromic approach lets you treat the patient correctly at that first visit, interrupt transmission, and link them into the national programme — all without waiting for a culture report. This module teaches you how the approach works, which kit to reach for, and how to make the consultation count.
References
- NACO National Guidelines on Prevention, Management and Control of RTI/STI, Ministry of Health & Family Welfare, Government of India (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, Ch. on STD/Syndromic Management (textbook)
- IADVL Textbook of Dermatology, Ch. on Sexually Transmitted Infections (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old lorry driver walks into a rural primary health centre on a Sunday evening complaining of a burning discharge from the penis that began three days ago. There is no microbiology laboratory for forty kilometres, no Gram stain, no culture, and the man tells you plainly that he will be on the road again tomorrow and cannot return. If you wait for a confirmed organism, he leaves untreated, his regular and casual partners stay exposed, and the chain of transmission continues. If instead you recognise his urethral discharge syndrome and treat for the two organisms that almost always cause it, he walks out cured tonight. This is the everyday reality that the syndromic approach was designed for.
WHY THIS MATTERS
As a final-year student soon to be posted at a PHC or in a busy district STD clinic, you will rarely have the luxury of an etiological diagnosis at the moment a patient needs treatment. The syndromic approach is the official Government of India strategy under the National AIDS Control Programme precisely because it is fast, evidence-based, and deliverable by any trained health worker. Getting it right means you cure the patient on the first visit, you protect their partners, and you reduce the population reservoir of infections — including those that facilitate HIV transmission. Getting it wrong, or insisting on organism-specific work-up you cannot obtain, means missed treatment, ongoing spread, and a patient lost to follow-up.
RECALL
Before we go further, recall what you already know. You learned the common STI pathogens in microbiology: Neisseria gonorrhoeae and Chlamydia trachomatis causing urethral and cervical infection; Treponema pallidum, Haemophilus ducreyi, and herpes simplex virus causing genital ulcers; Trichomonas vaginalis and Candida causing vaginal discharge. You also know from your dermatology reading that a genital ulcer can be painful or painless, and that this single feature carries enormous diagnostic weight. The syndromic approach takes exactly this kind of clinical pattern recognition — the cluster of symptoms and signs the patient presents with — and converts it directly into a treatment decision.
Why Manage STDs by Syndrome, Not Organism
Why STDs Are Managed by Syndrome
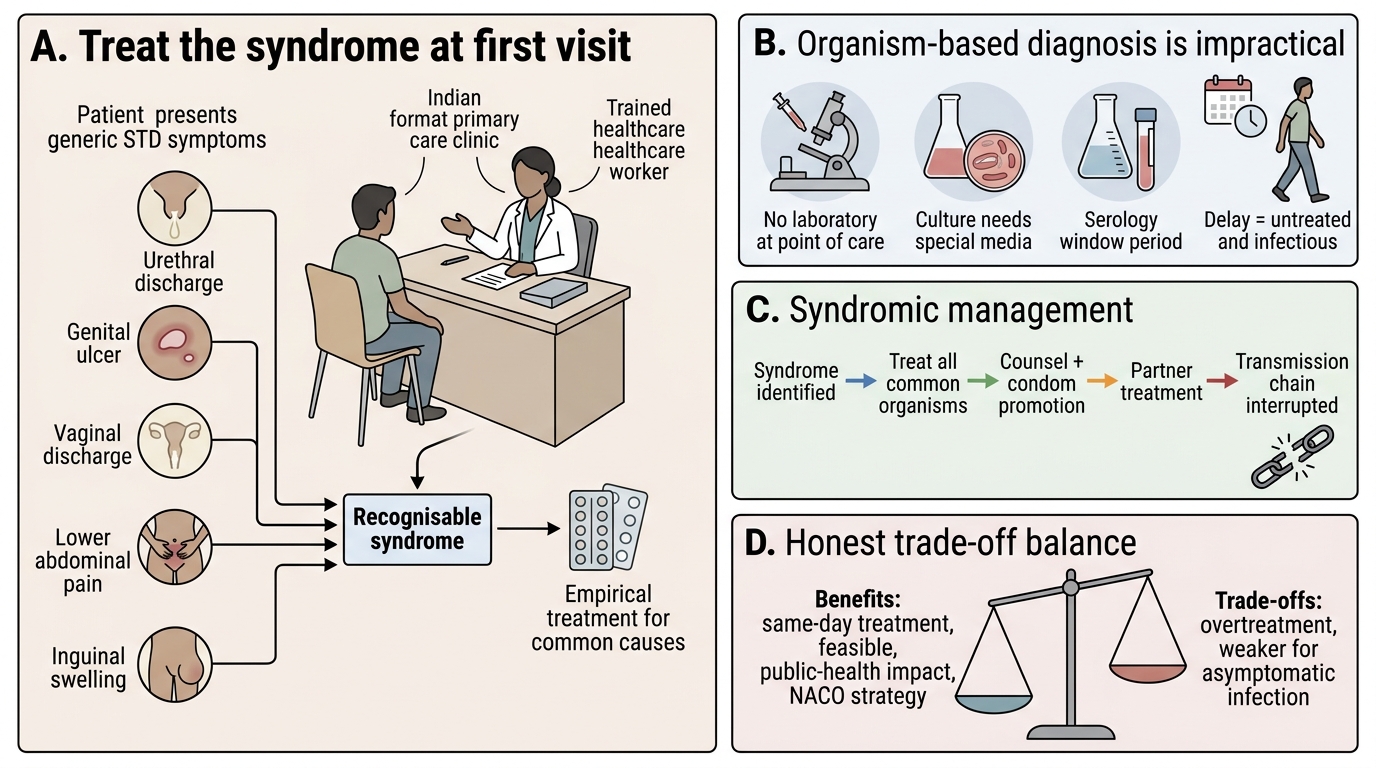
The central idea of syndromic management is deceptively simple: we treat the patient according to the syndrome they present with — the recognisable group of symptoms and signs — rather than waiting to identify the exact organism. This matters because in the settings where most Indian patients first seek care, organism identification is simply not available at the point of contact. There is no laboratory, or the laboratory cannot give a same-day result, or the patient cannot or will not return for a follow-up visit. A culture for Haemophilus ducreyi is technically demanding and rarely available; gonococcal culture needs special transport media; serology has a window period during which it reads falsely negative. If treatment depended on these, the patient would leave the clinic untreated and infectious. Syndromic management solves this by treating, at the first visit, for all the common organisms that produce a given syndrome at once. It is empirical, it is delivered with a simple flowchart any trained worker can follow, and it is the official NACO strategy under the National AIDS Control Programme. Critically, it is not a lazy shortcut — it is an evidence-based public-health intervention designed to break transmission chains where definitive diagnosis is impractical.
The trade-offs are worth naming honestly. Syndromic management over-treats some patients (a person with a non-infective cause receives antibiotics) and it is weakest for the asymptomatic or minimally symptomatic infections — particularly cervical infection in women, where the syndrome is an unreliable marker of underlying gonorrhoea or chlamydia. Where laboratory support exists, etiological or a hybrid approach is preferred. But for the symptomatic patient at the periphery, syndromic management remains the right first move.
Principles of Syndromic Management and NACO Framework
Principles of Syndromic STI Management and NACO Kit Framework
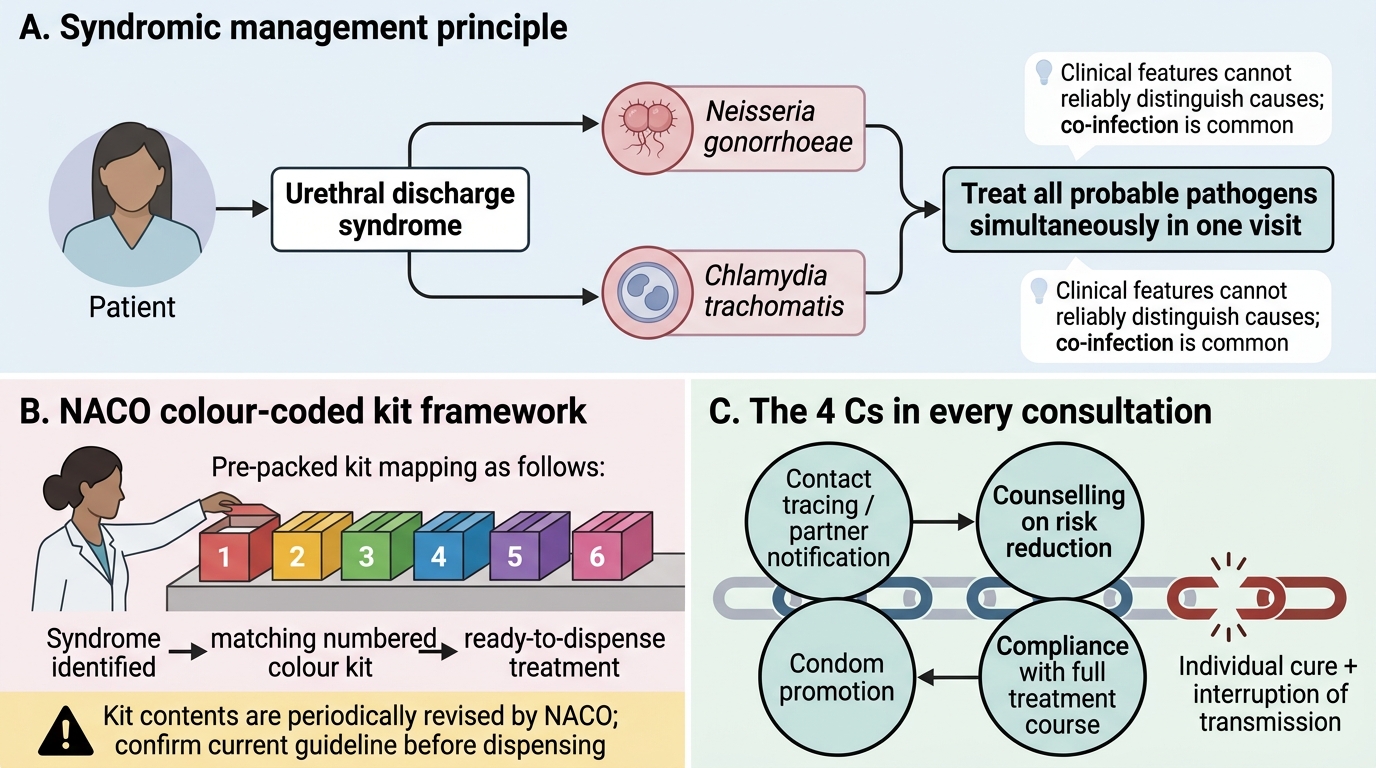
Three governing principles make the approach work. First, treat all the probable pathogens of a syndrome simultaneously — for urethral discharge that means covering both gonorrhoea and chlamydia in a single visit, because you cannot tell them apart clinically and co-infection is common. Second, the approach is operationalised through pre-packed, colour-coded kits: NACO supplies treatment as ready-to-dispense kits so that the health worker selects a kit by syndrome rather than writing individual prescriptions, which standardises dosing and improves compliance. Third, every consultation must include the 4 Cs — contact tracing (or partner notification), counselling on risk reduction, compliance with the full course of treatment, and condom promotion. The 4 Cs are not optional add-ons; they are what converts an individual cure into a break in the transmission chain.
The kit system deserves a careful caveat. The kits are numbered and colour-coded, and each maps to a syndrome, but the precise drug contents are revised periodically by NACO as resistance patterns and drug availability change. You should therefore learn the syndrome-to-kit mapping as a framework and always confirm the current contents against the prevailing NACO guideline edition before dispensing. The table below summarises the mapping as taught, with that caveat firmly in place.
NACO Colour-Coded STI/RTI Syndromic Kits
- The kit is chosen by syndrome, not by suspected organism.
- The 4 Cs accompany every kit dispensed.
- Kit contents are revised periodically — verify against the current NACO guideline.
The Seven NACO Syndromes and Their Colour-Coded Kits
NACO Colour-Coded STI/RTI Syndrome Kits
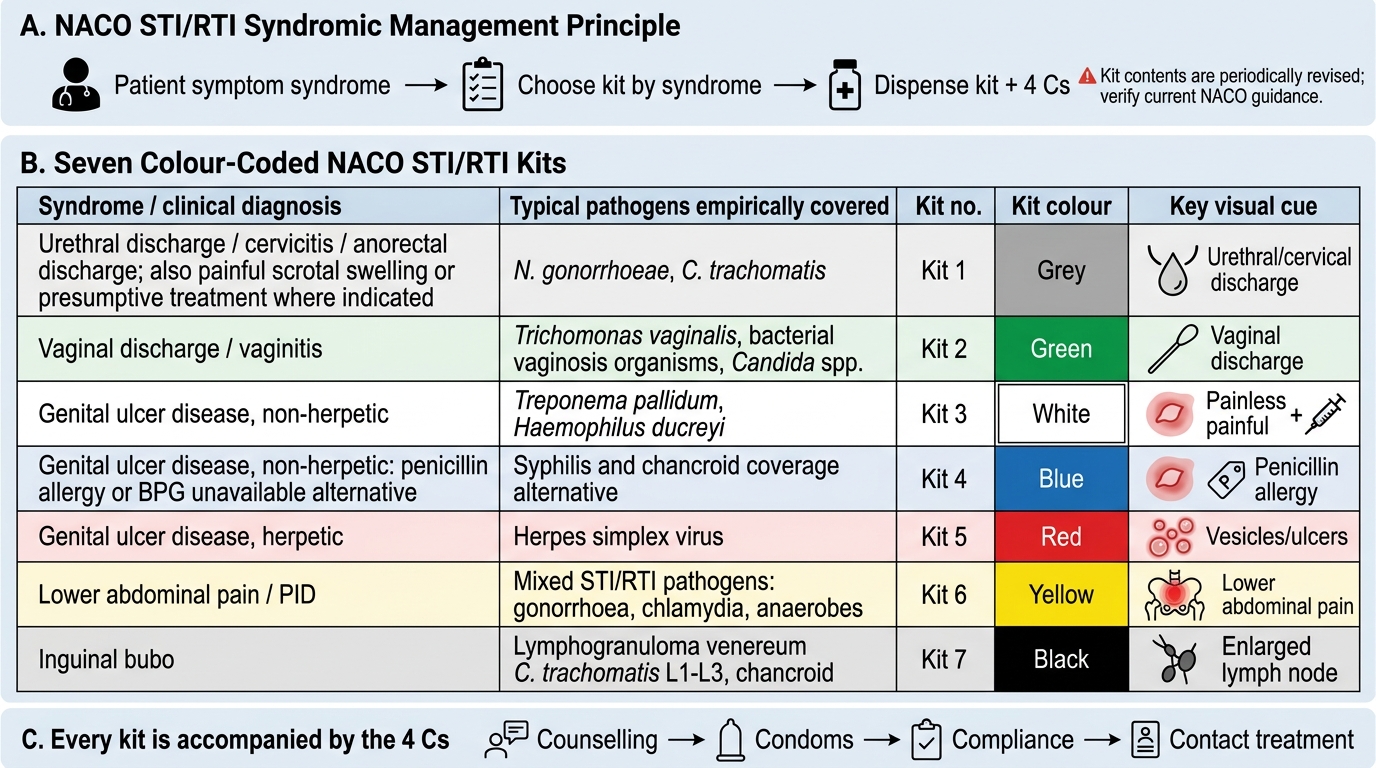
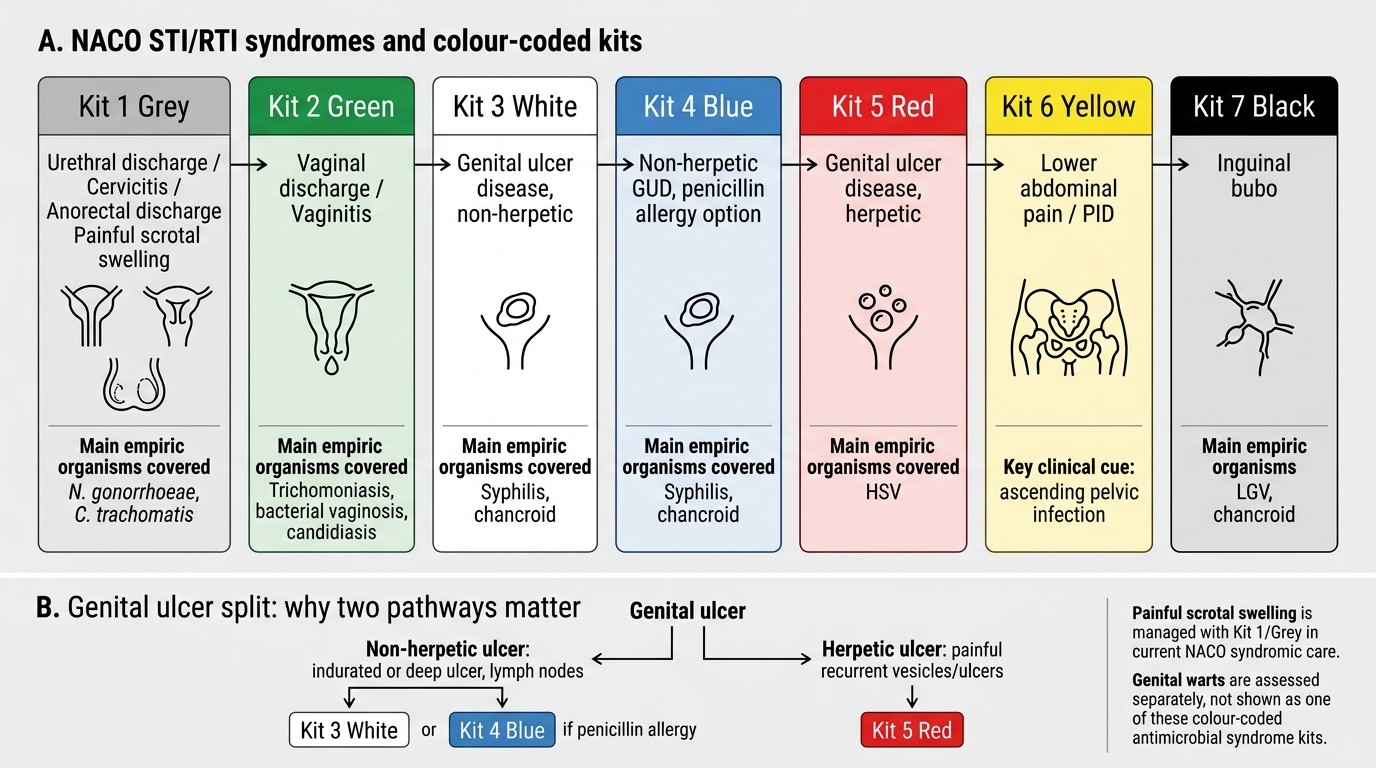
NACO recognises a defined set of STI/RTI syndromes, each with a characteristic presentation and a corresponding kit. Learning these as a set — syndrome, the organisms it empirically covers, and the kit — is the core skill of this module. The principal syndromes are: urethral discharge (and cervicitis and anorectal discharge, covered together), caused chiefly by gonorrhoea and chlamydia; vaginal discharge, caused by trichomoniasis, bacterial vaginosis, and candidiasis; genital ulcer disease, which is split into a non-herpetic group (syphilis and chancroid) and a herpetic group (HSV); lower abdominal pain suggesting pelvic inflammatory disease; inguinal bubo, the swollen, sometimes suppurative inguinal node of lymphogranuloma venereum or chancroid; scrotal swelling, an epididymo-orchitis picture; and the anorectal syndrome in receptive anal intercourse. Each maps to a colour-coded kit as taught by NACO (per current NACO guidance, contents subject to revision): Kit 1 grey for urethral discharge / cervicitis / anorectal; Kit 2 green for vaginal discharge; Kit 3 white for non-herpetic genital ulcer (covering syphilis and chancroid together); Kit 4 blue for herpetic genital ulcer; Kit 5 red for lower abdominal pain / PID; Kit 6 yellow for inguinal bubo; and Kit 7 black for genital warts.
The reason genital ulcer disease is split into two kits is clinically important and recurs throughout this cluster: a non-herpetic ulcer (Kit 3) needs antibacterial cover for Treponema and Haemophilus, whereas a herpetic ulcer (Kit 4) needs antiviral therapy — antibiotics do nothing for HSV. Recognising vesicles or a recurrent history pushes you toward Kit 4; an indurated painless ulcer or a painful ragged ulcer pushes you toward Kit 3.
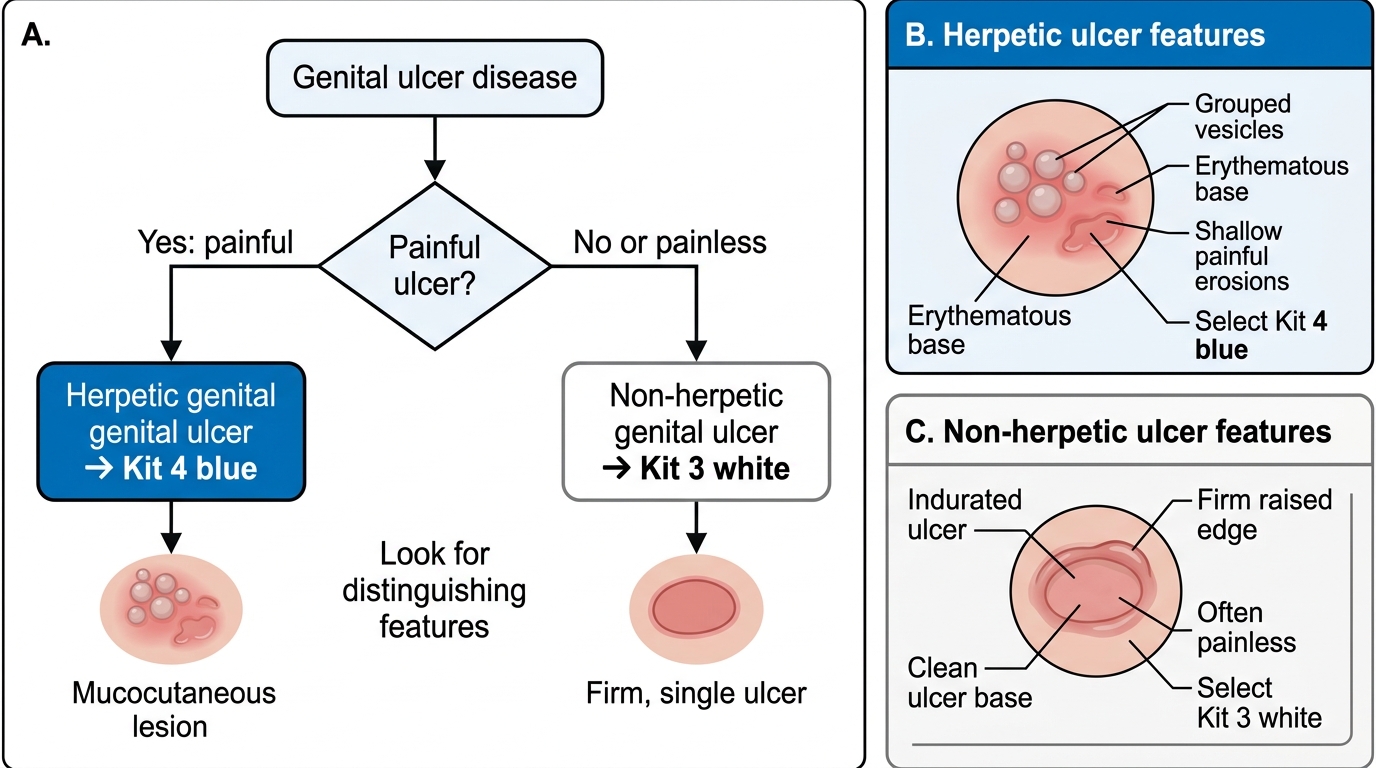
Genital Ulcer Disease: Painful vs Painless Kit Selection
- Urethral / cervical / anorectal discharge → Kit 1 grey.
- Vaginal discharge → Kit 2 green.
- Non-herpetic genital ulcer (syphilis + chancroid) → Kit 3 white; herpetic ulcer → Kit 4 blue.
- Lower abdominal pain / PID → Kit 5 red; inguinal bubo → Kit 6 yellow; genital warts → Kit 7 black.
SELF-CHECK
A male patient presents with painful micturition and a purulent urethral discharge. Which NACO kit is selected, and what is the rationale?
A. Kit 2 green — to cover the candidal and trichomonal causes of his discharge
B. Kit 1 grey — to empirically cover both gonorrhoea and chlamydia, the two organisms that cause urethral discharge syndrome
C. Kit 4 blue — because urethral discharge is most often viral in origin
D. No kit — withhold treatment until a Gram stain and culture confirm the organism
Reveal Answer
Answer: B. Kit 1 grey — to empirically cover both gonorrhoea and chlamydia, the two organisms that cause urethral discharge syndrome
Urethral discharge syndrome maps to Kit 1 (grey), which provides empirical cover for both gonorrhoea and chlamydia simultaneously, because the two cannot be distinguished clinically and co-infection is common. Waiting for laboratory confirmation defeats the entire purpose of the syndromic approach at the point of care.