Page 2 of 35
DR10.1 | Syndromic Case Management of Sexually Transmitted Diseases — SDL Guide (Part 2)
Interpreting the Syndrome and Selecting the Right Kit
Syndromic STI Interpretation and Kit Selection
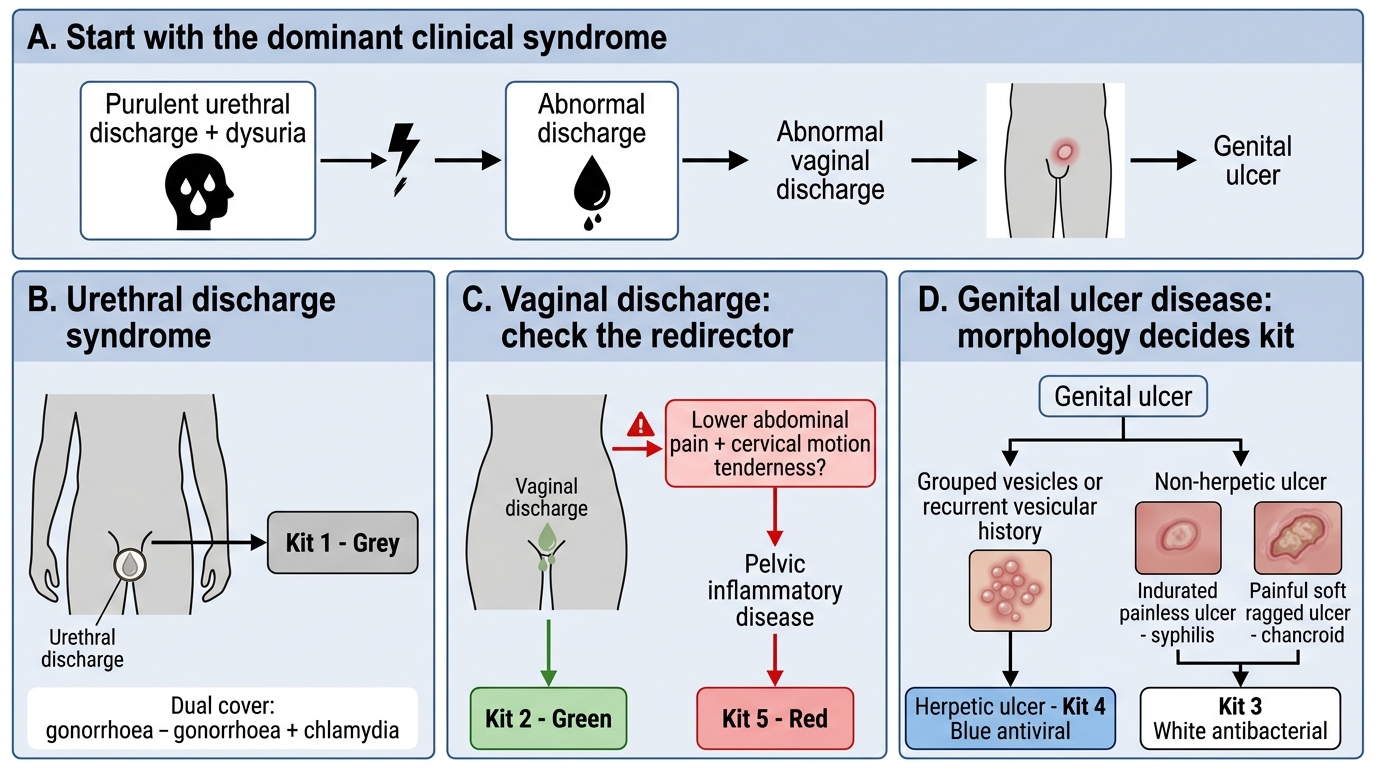
Interpreting a presentation correctly means matching the dominant clinical feature to a syndrome and then to its kit, while staying alert to the few features that redirect you. Consider three worked presentations. A man with purulent urethral discharge and dysuria has urethral discharge syndrome and receives Kit 1 (grey) — dual cover for gonorrhoea and chlamydia. A woman complaining of an abnormal vaginal discharge has vaginal discharge syndrome and receives Kit 2 (green), but you must additionally screen for lower abdominal tenderness, because if she has lower abdominal pain with cervical motion tenderness the picture becomes pelvic inflammatory disease, which needs Kit 5 (red) — a different and broader regimen. A patient with a genital ulcer is the most decision-rich: the single question "is the ulcer painful or painless, and are there grouped vesicles?" sorts the herpetic from the non-herpetic ulcer. Grouped vesicles or a recurrent vesicular history indicate herpes and Kit 4 (blue, antiviral); an indurated painless ulcer (syphilis) or a painful, soft, ragged ulcer (chancroid) indicate the non-herpetic group and Kit 3 (white, antibacterial).
The practical discipline is to interpret the dominant syndrome but actively look for the redirector — vaginal discharge that conceals PID, or a genital ulcer whose morphology decides antiviral versus antibacterial. The flowchart above formalises the GUD branch; the same painful-versus-painless logic threads through SDLs C, D, and E in this cluster.
- Match the dominant symptom to a syndrome, then to its kit.
- Always check vaginal discharge for coexisting lower abdominal pain → escalate to Kit 5 (PID).
- Vesicles or recurrence → herpetic GUD → Kit 4 (blue); otherwise non-herpetic GUD → Kit 3 (white).
Partner Management, the 4 Cs, and Programme Integration
Partner Management and Programme Integration in STI Care
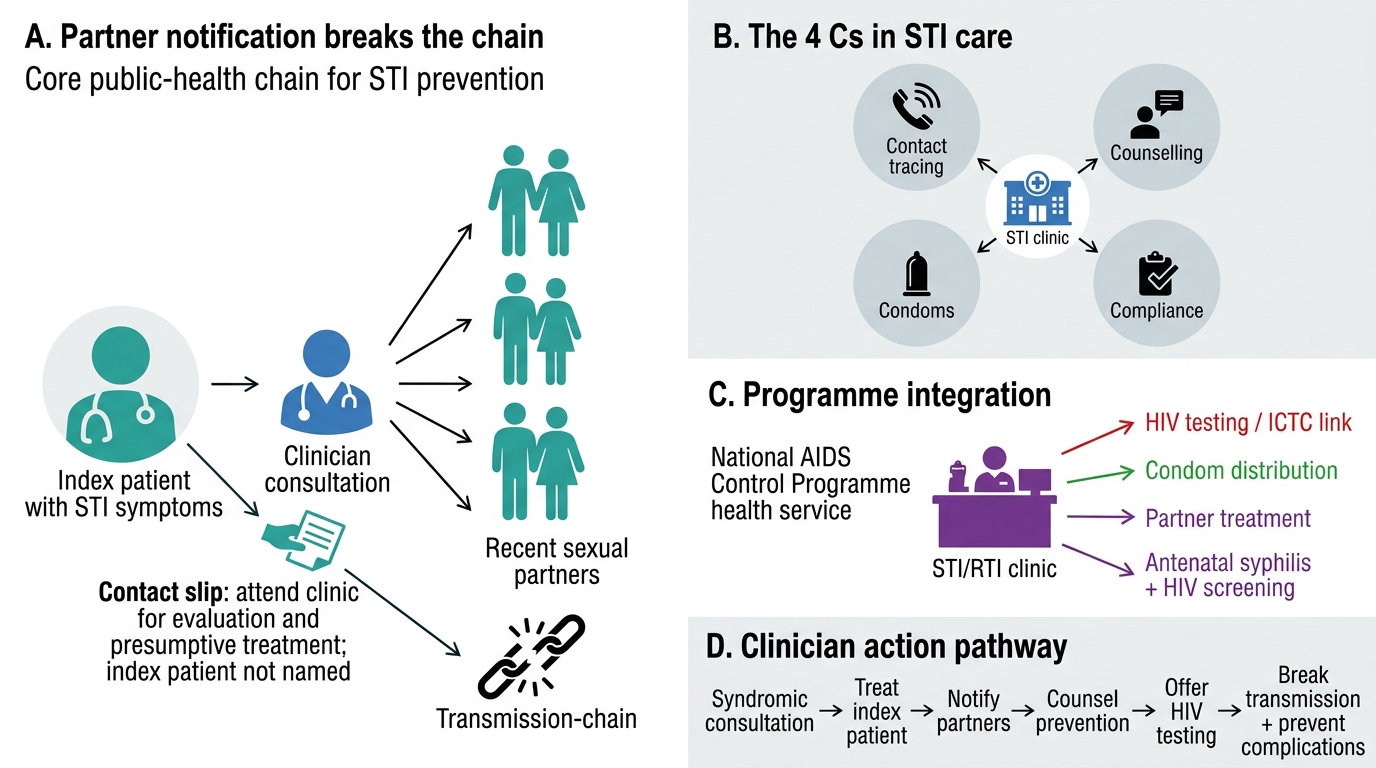
Treating the index patient cures one person; managing the partners breaks the chain. Partner notification is therefore not an afterthought but a defined step, usually delivered through the contact-slip method: the index patient is given a slip (or slips) to pass to recent sexual partners, inviting them to attend for evaluation and presumptive treatment without naming the index patient on the slip. Counselling supports this — you explain why partners must be treated even if asymptomatic, you promote consistent condom use, and you reinforce completing the full course of treatment. These are the 4 Cs in action: contact tracing, counselling, compliance, and condoms. Alongside them, every STI consultation is an opportunity to offer HIV testing and link the patient to integrated counselling and testing services, because STIs and HIV travel together and an STI both signals risk and biologically facilitates HIV acquisition.
Programme integration ties the visit to the wider system. Under the National AIDS Control Programme, STI/RTI services are delivered through designated clinics and linked to HIV testing, condom distribution, and — where relevant — antenatal screening for syphilis and HIV to prevent vertical transmission. As the treating clinician you are the entry point: a competent syndromic consultation that also offers HIV testing, notifies partners, and counsels on prevention does far more public-health work than the antibiotic alone.
- Notify partners using the contact-slip method; treat them presumptively.
- Deliver all 4 Cs — contact tracing, counselling, compliance, condoms — at every visit.
- Offer HIV testing and link the patient into NACP services.
SELF-CHECK
A woman is treated for vaginal discharge syndrome with Kit 2. She asks why her husband also needs to come for treatment when he has no symptoms. What is the best basis for your advice?
A. He does not need treatment unless he develops symptoms himself
B. Partner treatment is required to break the transmission chain and prevent re-infection, even when the partner is asymptomatic — part of the 4 Cs
C. He should be treated only if a laboratory confirms he carries the organism
D. He should be given a different kit chosen at random to be safe
Reveal Answer
Answer: B. Partner treatment is required to break the transmission chain and prevent re-infection, even when the partner is asymptomatic — part of the 4 Cs
Partner management is integral to syndromic care. An asymptomatic partner can harbour and re-transmit infection, so presumptive partner treatment (typically via the contact-slip method) is needed to interrupt transmission and prevent the index patient's re-infection. This is the contact-tracing component of the 4 Cs.
Self-Assessment — Syndromic Management Scenarios
Test your reasoning against the three commonest decisions you will face. First, recall the mapping itself: which kit and colour for urethral discharge, for vaginal discharge, for non-herpetic versus herpetic genital ulcer, for PID, for inguinal bubo, and for genital warts — and remember that the contents behind each colour are revised periodically, so the colour is a framework you confirm against the current NACO guideline. Second, practise the redirectors: a woman with vaginal discharge who also has lower abdominal pain and cervical motion tenderness is no longer a Kit 2 problem but a Kit 5 (PID) problem; a genital ulcer's morphology decides Kit 3 versus Kit 4. Third, rehearse the 4 Cs out loud, because in the examination and at the bedside the marks and the patient benefit come from remembering to notify partners, counsel, ensure compliance, promote condoms, and offer HIV testing — not from the antibiotic choice alone.
Work through the self-check questions below, and for each, force yourself to state the rationale, not just the answer. If you can explain why dual cover, why partner treatment, and why the painful-versus-painless split decides the GUD kit, you have understood syndromic management rather than memorised a colour chart.
- Map every syndrome to its kit and colour (confirm contents per current NACO guidance).
- Spot the redirectors: vaginal discharge + lower abdominal pain → PID/Kit 5; ulcer morphology → Kit 3 vs Kit 4.
- Always deliver the 4 Cs and offer HIV testing.
SELF-CHECK
A patient presents with grouped vesicles on the glans that have ruptured into shallow, painful ulcers, and reports a similar episode three months ago. Which kit is appropriate and why?
A. Kit 3 white — non-herpetic genital ulcer, because all genital ulcers need antibacterial cover
B. Kit 4 blue — herpetic genital ulcer, because grouped vesicles and recurrence indicate HSV, which requires antiviral rather than antibacterial therapy
C. Kit 1 grey — because the lesions are on the genitalia
D. Kit 6 yellow — because vesicular lesions always indicate an inguinal bubo
Reveal Answer
Answer: B. Kit 4 blue — herpetic genital ulcer, because grouped vesicles and recurrence indicate HSV, which requires antiviral rather than antibacterial therapy
Grouped vesicles evolving to painful shallow ulcers, especially with a recurrent history, are characteristic of herpes genitalis (HSV). This is herpetic genital ulcer disease and maps to Kit 4 (blue), which provides antiviral therapy. Kit 3 (white) covers the non-herpetic group (syphilis and chancroid) with antibacterials, which would not treat HSV.
CLINICAL PEARL
When a patient presents with a genital ulcer, the single most useful bedside question costs nothing and decides your kit: is it painful, and are there grouped vesicles? Painful grouped vesicles or a recurrent vesicular history point to herpes (Kit 4, antiviral); a painless indurated ulcer (syphilis) or a painful, soft, ragged, undermined ulcer (chancroid) point to the non-herpetic group (Kit 3, antibacterial). Train yourself to ask it every single time — it is the highest-yield discriminator in genital ulcer disease and it threads through every syphilis and GUD topic in this cluster.