Page 1 of 12
DR13.1 | Autoimmune Vesiculobullous Disorder Diagnosis — SDL Guide
Learning Objectives
- Describe the morphology of vesiculobullous lesions and distinguish flaccid from tense bullae at the bedside.
- Explain the etiopathogenesis of pemphigus vulgaris and bullous pemphigoid, including the level of epidermal cleavage and the target autoantigens.
- Diagnose pemphigus vulgaris and bullous pemphigoid clinically using lesion morphology, Nikolsky's sign and the Bulla-spread sign.
- Select and interpret appropriate confirmatory investigations — Tzanck smear, skin biopsy with H&E, and direct immunofluorescence.
- Construct a differential diagnosis for a patient presenting with blisters and outline first-line management principles.
INSTRUCTIONS
A patient who walks into your clinic with blisters poses an immediate diagnostic challenge: some blistering diseases are self-limiting nuisances, while others — the autoimmune vesiculobullous disorders — are potentially fatal if missed. Pemphigus vulgaris, before the corticosteroid era, killed most patients within a year. The single most important early skill is to separate an intra-epidermal disease (pemphigus) from a sub-epidermal one (bullous pemphigoid), because the two differ in prognosis, the urgency of referral, and the intensity of immunosuppression required. This module builds that diagnostic reasoning from lesion morphology, through two simple bedside signs you can elicit with gloved hands, to the immunofluorescence findings that confirm the diagnosis.
References
- Neena Khanna — Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed., Ch. on Vesiculobullous Disorders (textbook)
- IADVL Textbook of Dermatology, 4th ed., Section on Immunobullous Diseases (textbook)
- Roxburgh's Common Skin Diseases, 18th ed., Ch. on Bullous Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 48-year-old schoolteacher comes to your outpatient clinic having lived for two months with painful mouth ulcers that never healed. She has stopped eating solid food. In the last fortnight, soft fragile blisters have begun appearing on her scalp, chest and back; they break almost as soon as they form, leaving raw, weeping erosions. A junior colleague has been treating her for "recurrent aphthous ulcers" and a separate "skin infection." When you run a gloved finger sideways across her normal-looking chest skin, the top layer slides away like wet tissue paper. That single finding — a positive Nikolsky's sign — reframes the entire case. This is not two unrelated problems; it is one disease, pemphigus vulgaris, in which the patient's own antibodies are dissolving the glue between her skin cells. Recognising it today, rather than weeks from now, is the difference between a controllable disease and a life-threatening one.
WHY THIS MATTERS
As a newly qualified doctor in India, you will be the first clinician many blistering patients ever meet — in a PHC, a district hospital casualty, or a general medicine ward. Autoimmune vesiculobullous disorders are uncommon but not rare, and they are dangerous precisely because they are easily misdiagnosed as impetigo, drug rash, burns, or recurrent stomatitis. Extensive erosions behave like burns: they lose fluid and protein, and they are a wide-open portal for sepsis, still the leading cause of death in pemphigus. You do not need a dermatologist to suspect the diagnosis — you need to recognise the morphology, elicit two bedside signs correctly, order the right confirmatory tests, and refer early. The diagnostic discipline you build here is exactly what the competency DR13.1 asks of you: to diagnose common autoimmune vesiculobullous disorders on clinical grounds with the appropriate use of Nikolsky's and Bulla-spread signs.
RECALL
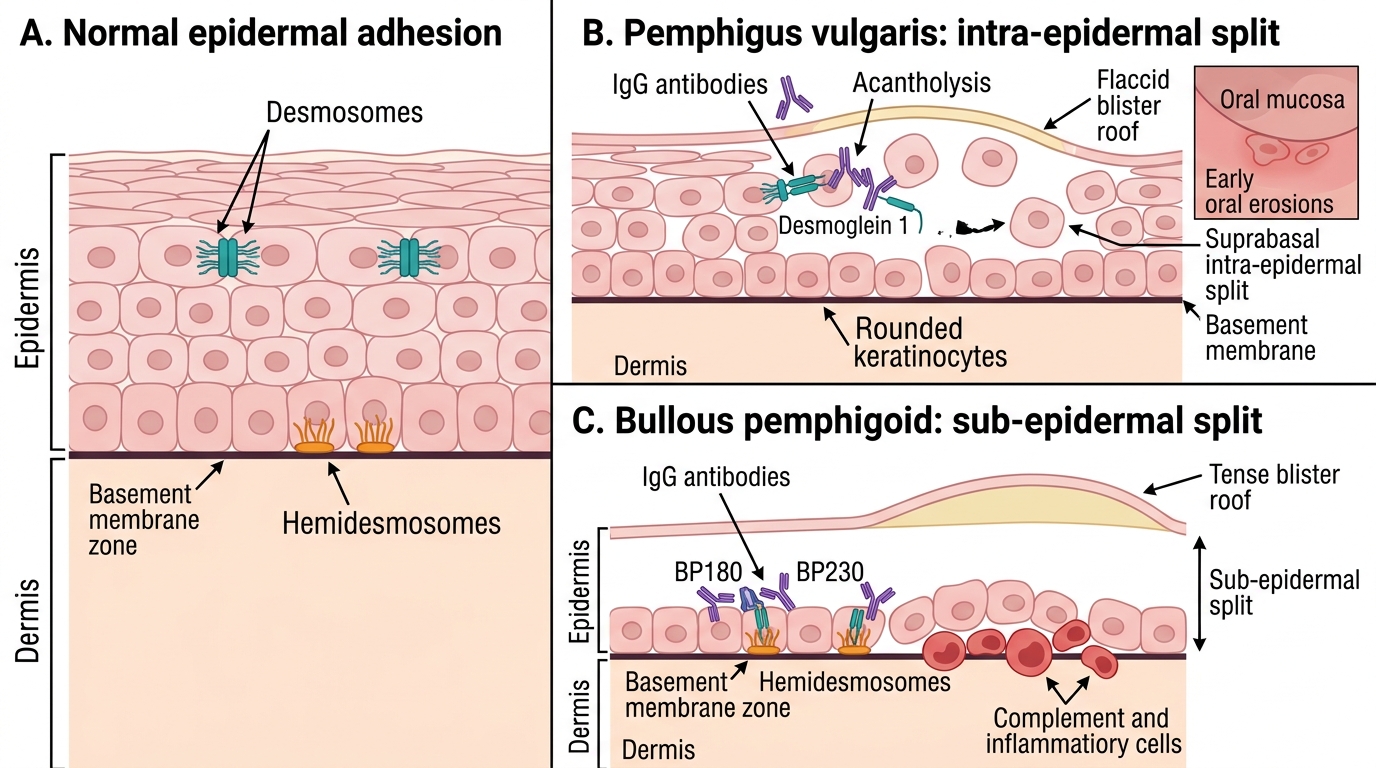
Before we begin, recall the architecture of normal skin from your first-year histology. The epidermis is a stratified squamous epithelium with four working layers — from the base upward: stratum basale, stratum spinosum, stratum granulosum and stratum corneum. Keratinocytes are held to one another by desmosomes (whose key adhesion proteins are the desmogleins) and anchored to the underlying basement membrane by hemidesmosomes (whose components include BP180 and BP230). Hold onto one simple idea: if the adhesion that fails is between keratinocytes, the split is inside the epidermis and the blister roof is thin and fragile; if the adhesion that fails is between the epidermis and the dermis, the split is beneath the epidermis and the blister roof is thick and tense. Everything in this module flows from where the skin comes apart.
Clinical Presentation: Morphology of Blisters in Skin Disease
Morphology of Blisters in Skin Disease
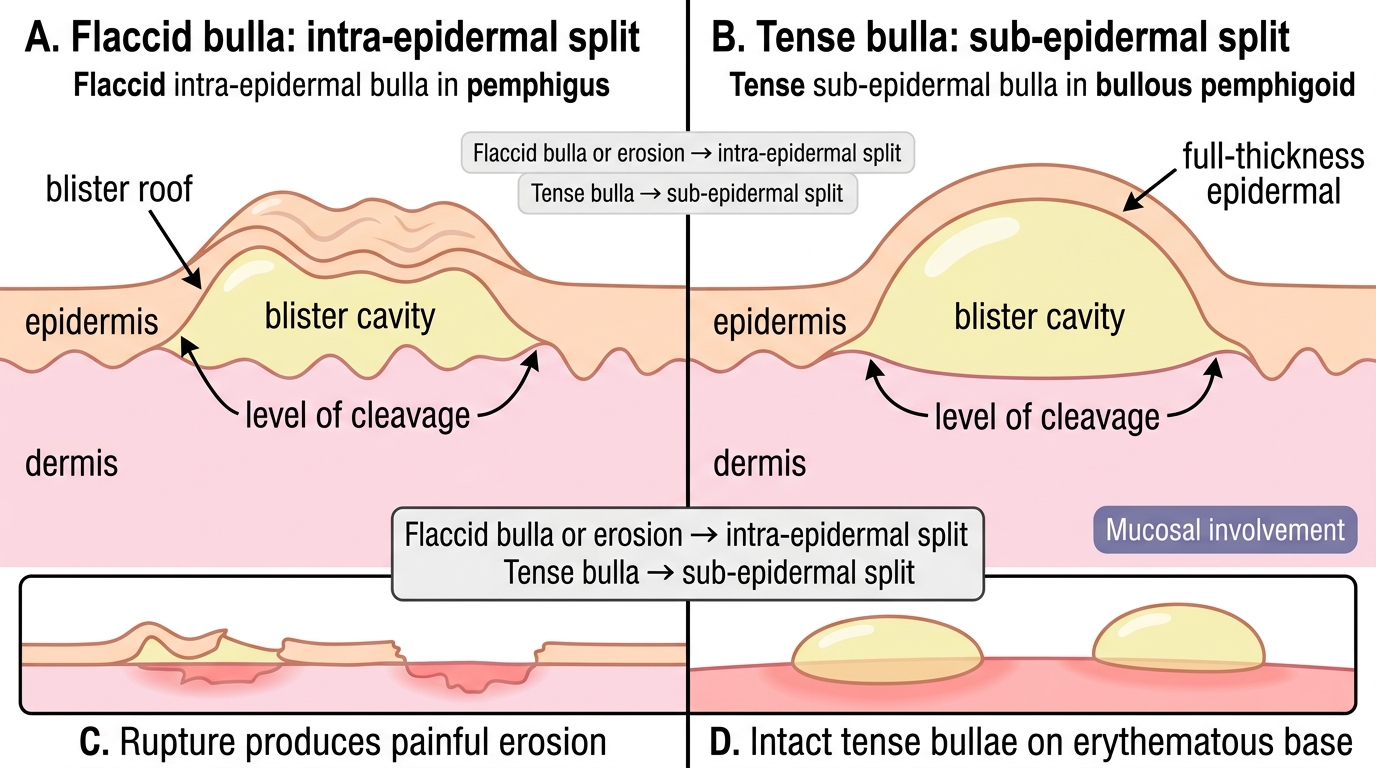
Diagnosis of blistering disease begins not with a laboratory test but with disciplined description of what you see. A vesicle is a small fluid-filled lesion (conventionally up to 0.5 cm) and a bulla is a larger one (above 0.5 cm); both are "primary" lesions, but their character tells you a great deal about the level of skin involved. The most useful single observation is whether a bulla is flaccid or tense. A flaccid bulla has a thin, easily ruptured roof and wrinkles or collapses under its own weight — it sits high, within the epidermis, so very little tissue lies above the fluid. A tense bulla is dome-shaped and resists rupture because a thicker roof of full-thickness epidermis lies over a deeper, sub-epidermal split. Because flaccid bullae break so readily, pemphigus patients are often seen not with intact blisters but with widespread painful erosions — raw denuded areas where the roof has already sheared off. Learning to read these features at the bedside lets you predict the level of cleavage before any biopsy is taken.
Key morphological clues to capture in every blistering patient:
- Flaccid bullae and erosions → suspect an intra-epidermal (high) split, e.g. pemphigus.
- Tense bullae on an erythematous or urticarial base → suspect a sub-epidermal (deep) split, e.g. bullous pemphigoid.
- Mucosal involvement (mouth, conjunctiva, genitalia) → common and often the first feature in pemphigus vulgaris; relatively spared in bullous pemphigoid.
- Distribution and age — pemphigus typically affects middle-aged adults; bullous pemphigoid characteristically affects the elderly.
Flaccid Versus Tense Bullae: Split Level Comparison
Etiopathogenesis: Intra-epidermal vs Sub-epidermal Autoimmunity
Split Level in Pemphigus Vulgaris vs Bullous Pemphigoid
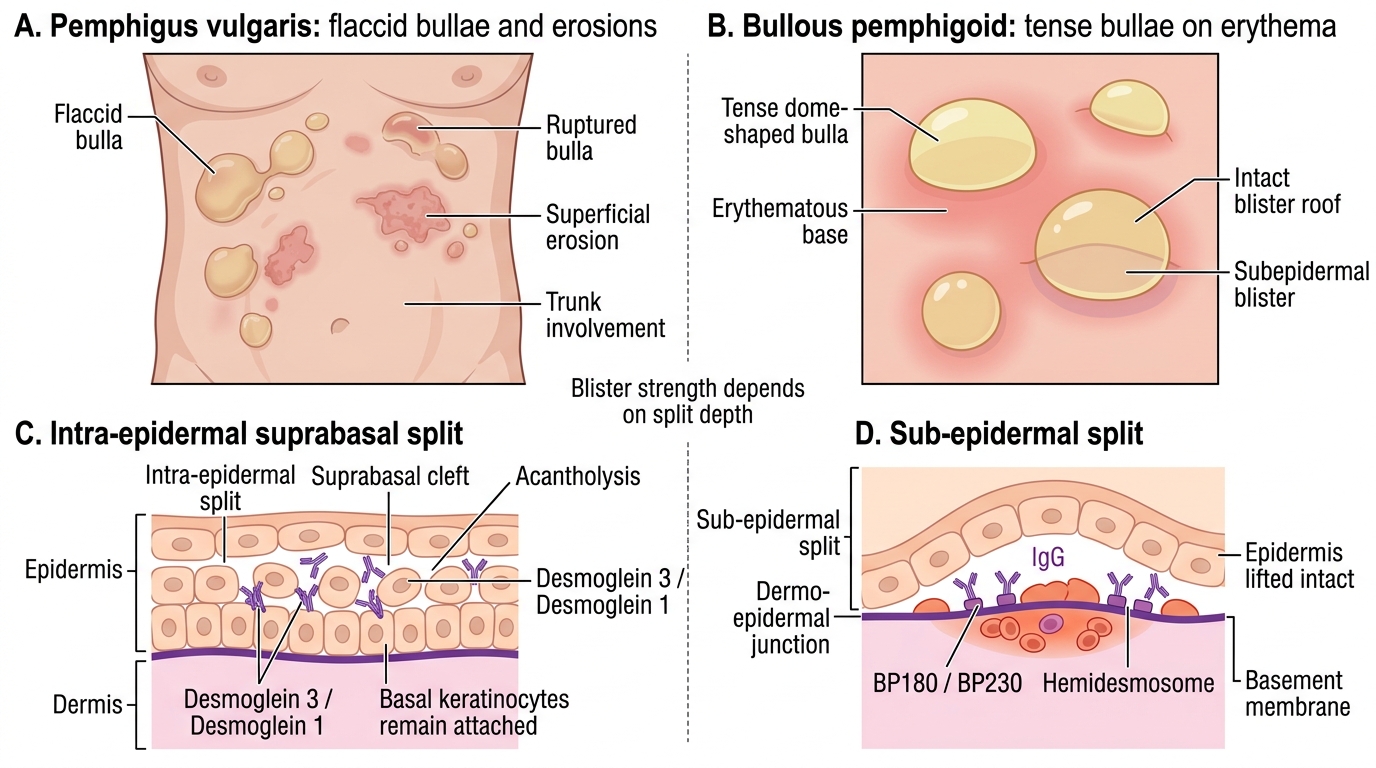
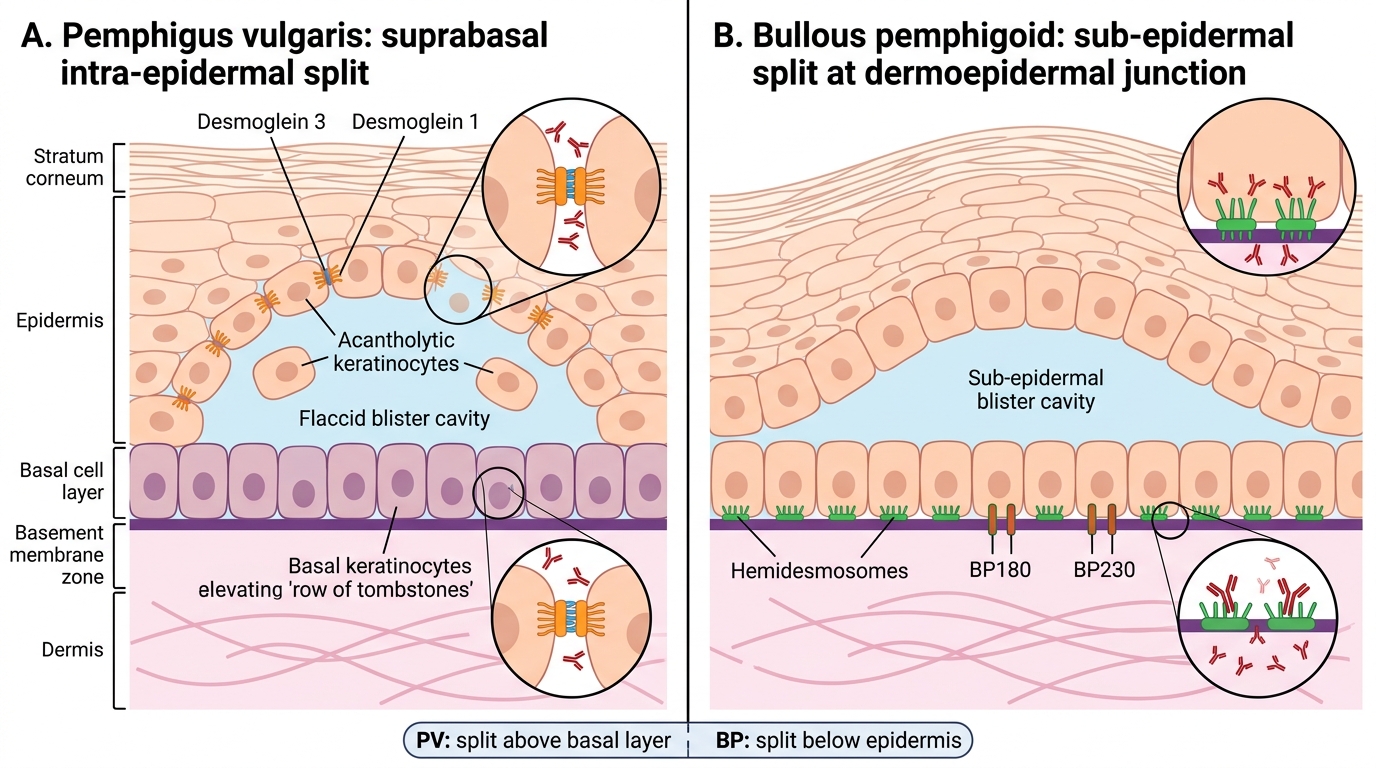
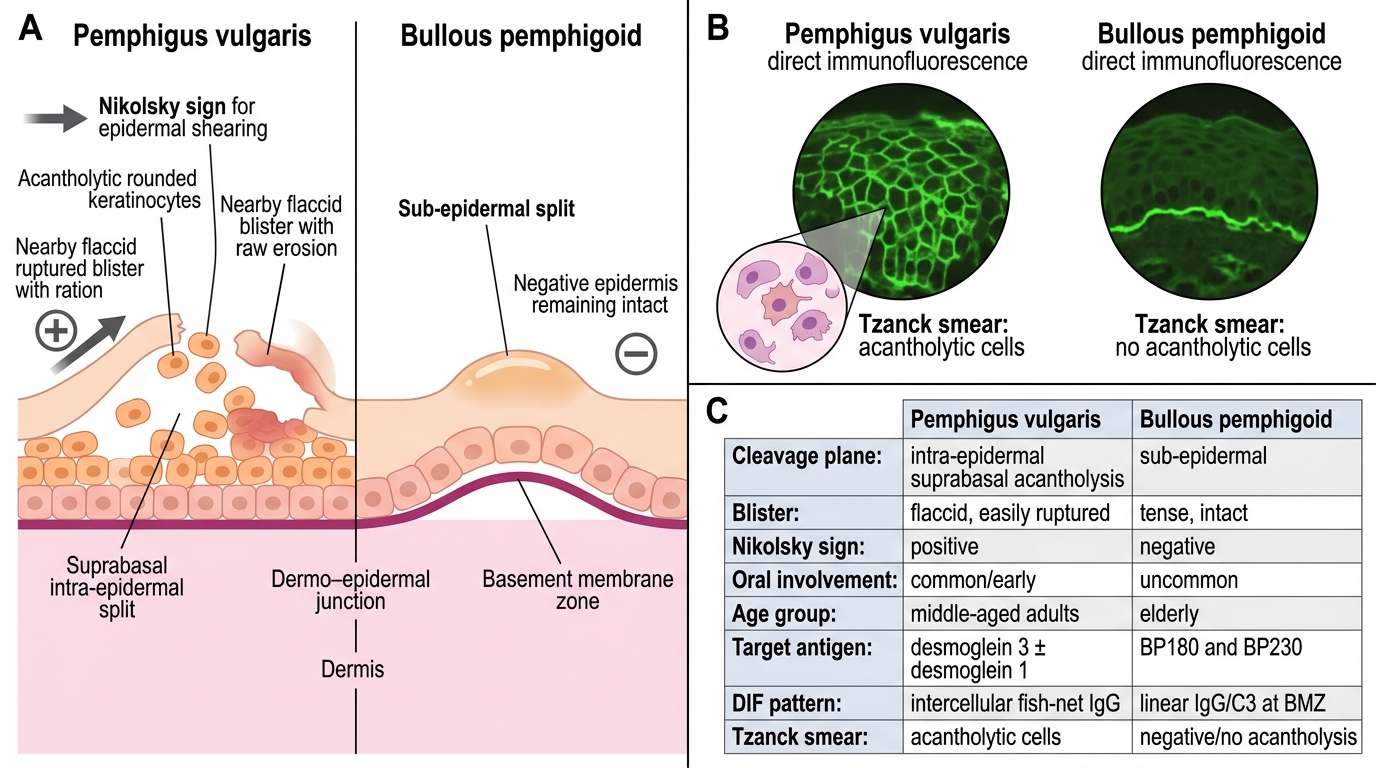
The clinical differences you just learned to observe are the direct, mechanical consequence of where in the skin an autoantibody attacks. Both pemphigus vulgaris and bullous pemphigoid are autoimmune diseases in which IgG antibodies bind structural adhesion proteins, but they target different molecules at different depths, and that single fact explains almost everything else. In pemphigus vulgaris, IgG antibodies are directed against desmoglein 3 (and, in patients with skin as well as mucosal disease, desmoglein 1) — the desmosomal proteins that bind keratinocytes together. When these are blocked, keratinocytes lose their grip on one another and round up, a process called acantholysis, producing a split within the epidermis, just above the basal layer (suprabasal). In bullous pemphigoid, IgG antibodies target the hemidesmosomal proteins BP180 (type XVII collagen) and BP230, which anchor the epidermis to the dermis; complement activation and inflammation then separate the whole epidermis from the dermis, producing a sub-epidermal split. Because the desmoglein-3-rich oral mucosa is heavily involved in pemphigus, oral erosions are often the earliest sign — whereas bullous pemphigoid, driven by basement-membrane antibodies, largely spares the mouth.
The split level dictates the rest of the clinical picture:
- Pemphigus vulgaris — anti-desmoglein 3/1 → intra-epidermal (suprabasal) acantholytic split → flaccid bullae, Nikolsky POSITIVE, oral involvement common, middle-aged onset.
- Bullous pemphigoid — anti-BP180/BP230 → sub-epidermal split → tense bullae, Nikolsky NEGATIVE, mouth usually spared, elderly onset.
- Direct immunofluorescence (DIF) confirms the target: pemphigus shows intercellular IgG/C3 in a "fish-net" pattern around keratinocytes; bullous pemphigoid shows a linear IgG/C3 band along the basement membrane zone.
Level of Blister Formation in Pemphigus Vulgaris and Bullous Pemphigoid
Clinical Features of Pemphigus Vulgaris
Clinical Features of Pemphigus Vulgaris
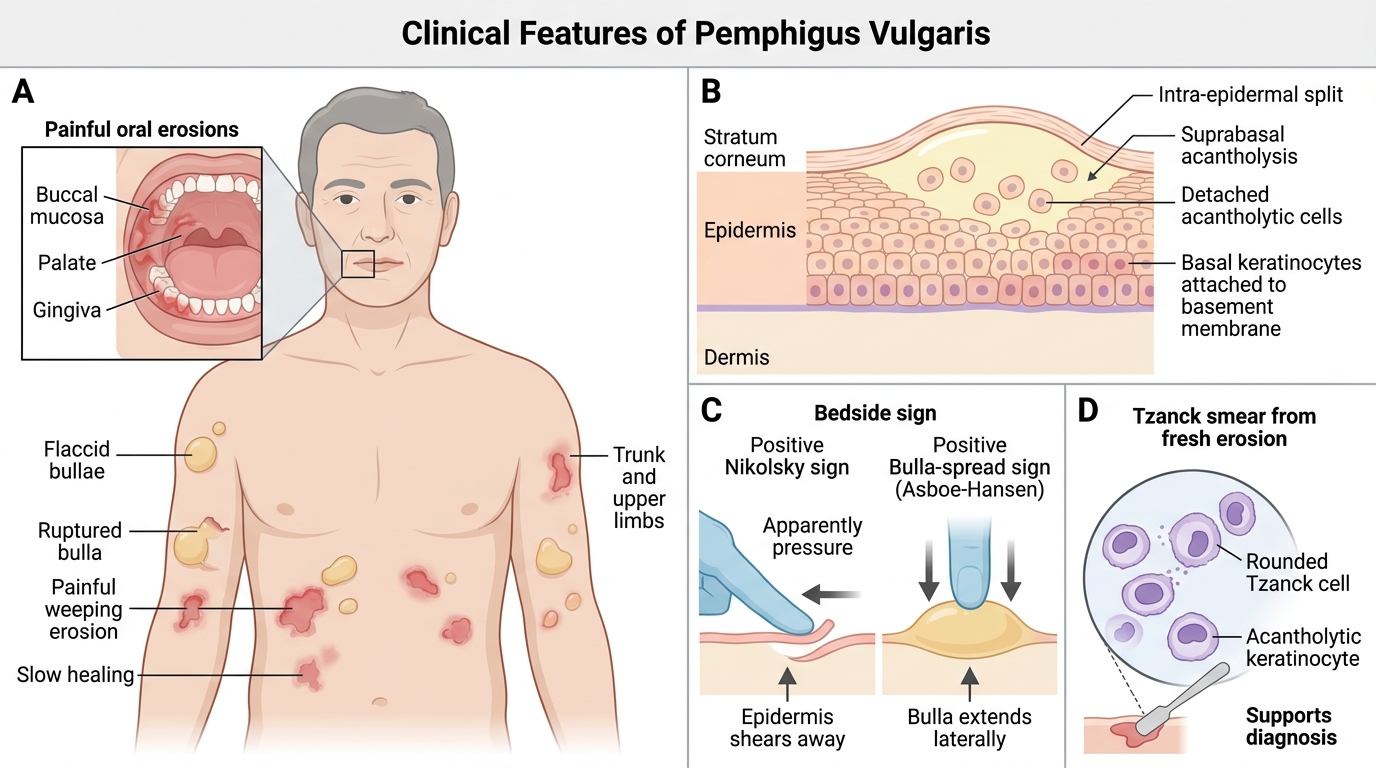
Pemphigus vulgaris is the prototype intra-epidermal autoimmune blistering disease, and recognising its pattern is the core of this competency. It usually presents in middle age, and in roughly half of patients the disease begins in the mouth — painful, slowly enlarging erosions on the buccal mucosa, palate or gingiva that fail to heal and are frequently mistaken for aphthous ulcers or candidiasis for weeks before the skin is involved. When cutaneous lesions appear, they are characteristically flaccid bullae that rupture easily, leaving painful, weeping erosions that enlarge at the periphery and are slow to re-epithelialise. Because the split is high in the epidermis, the skin around lesions is mechanically fragile: lateral pressure on apparently normal skin causes the superficial epidermis to shear away — a positive Nikolsky's sign — and downward pressure on an intact bulla makes it extend sideways — a positive Bulla-spread (Asboe-Hansen) sign. A bedside Tzanck smear taken from the floor of a fresh erosion shows rounded, detached acantholytic (Tzanck) cells, a quick clue that supports the diagnosis while you arrange confirmatory tests.
The diagnostic signature of pemphigus vulgaris:
- Onset: middle-aged adults; oral erosions often the first and most persistent feature.
- Skin: flaccid bullae and widespread painful erosions, not intact tense blisters.
- Bedside signs: Nikolsky's sign POSITIVE; Bulla-spread sign positive.
- Tzanck smear: acantholytic cells present.
- Immunopathology: intercellular (fish-net) IgG/C3 on DIF; circulating anti-desmoglein 3 (± desmoglein 1) antibodies on ELISA.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Pemphigus Vulgaris vs Bullous Pemphigoid
SELF-CHECK
A 50-year-old woman has two months of non-healing oral erosions followed by flaccid skin blisters that rupture into raw areas. Lateral pressure on normal-looking skin shears off the surface. Which combination correctly describes the likely diagnosis?
A. Bullous pemphigoid — sub-epidermal split, Nikolsky negative, anti-BP180/BP230
B. Pemphigus vulgaris — intra-epidermal acantholysis, Nikolsky positive, anti-desmoglein 3/1
C. Bullous pemphigoid — intra-epidermal split, Nikolsky positive, anti-desmoglein 3
D. Pemphigus vulgaris — sub-epidermal split, Nikolsky negative, anti-BP180
Reveal Answer
Answer: B. Pemphigus vulgaris — intra-epidermal acantholysis, Nikolsky positive, anti-desmoglein 3/1
Flaccid bullae, prominent oral involvement and a positive Nikolsky's sign point to pemphigus vulgaris, which is an INTRA-epidermal (suprabasal) acantholytic disease caused by IgG against desmoglein 3 (and desmoglein 1 when skin is involved). Bullous pemphigoid is the opposite on every axis: a SUB-epidermal split, tense bullae, Nikolsky NEGATIVE, and antibodies against BP180/BP230. Options that mix these features (intra-epidermal + Nikolsky positive attributed to pemphigoid, or sub-epidermal pemphigus) reverse the cleavage plane and are incorrect.