Page 2 of 12
DR13.1 | Autoimmune Vesiculobullous Disorder Diagnosis — SDL Guide (Part 2)
Clinical Features of Bullous Pemphigoid
Clinical Features of Bullous Pemphigoid
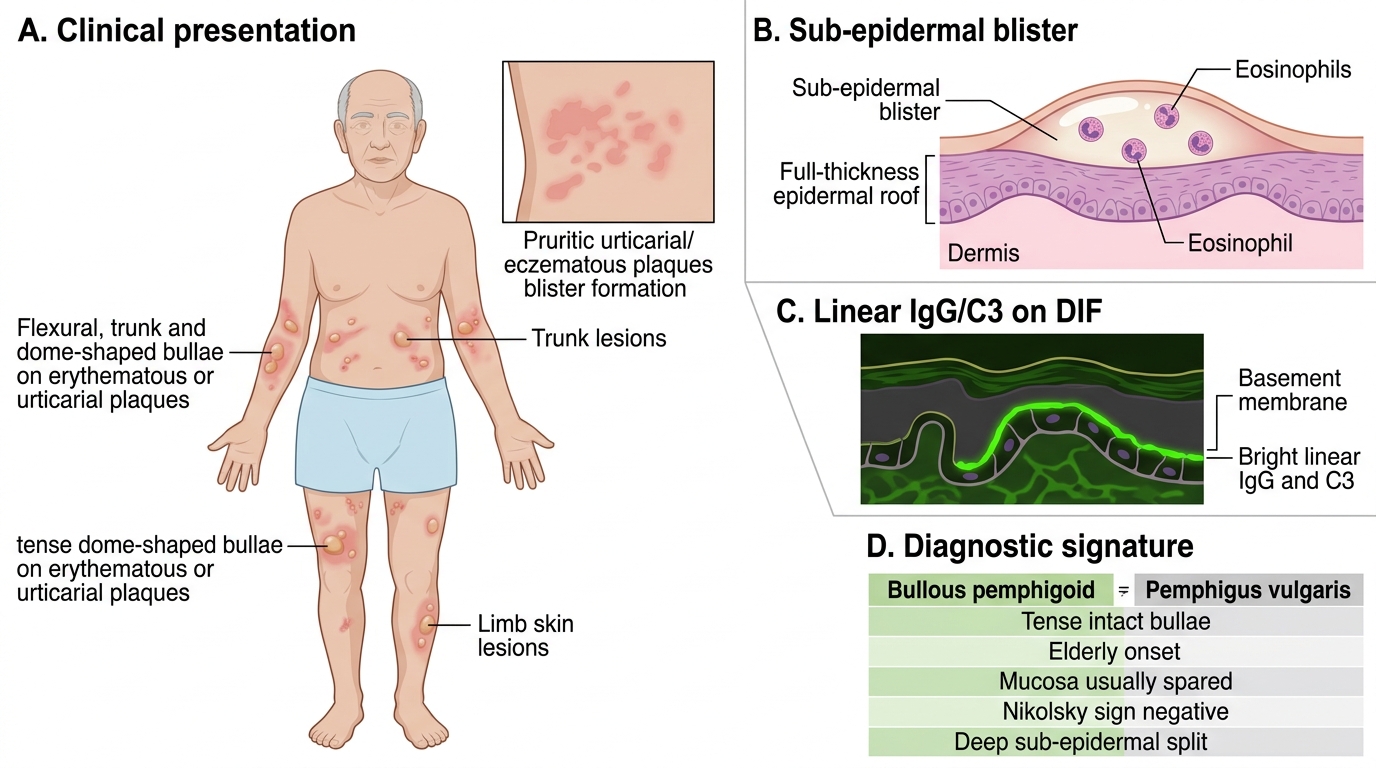
Bullous pemphigoid is the most common sub-epidermal autoimmune blistering disease and, in almost every respect, the clinical mirror image of pemphigus vulgaris — which is precisely why the two are taught together. It is a disease of the elderly, typically beyond the seventh decade. Many patients pass through a prodromal phase of intensely itchy, urticarial or eczematous plaques for weeks or months before any blister appears, so early bullous pemphigoid is easily mistaken for eczema or urticaria. When blisters develop they are tense, dome-shaped bullae arising on normal or erythematous/urticarial skin, often on the flexures, trunk and limbs; because the split is deep (sub-epidermal) the roof is full-thickness epidermis and the blisters resist rupture, so intact tense bullae — unlike in pemphigus — are usually still present when the patient is examined. The oral mucosa is usually spared or only mildly involved. Critically, because the basement membrane and the epidermis above it remain firmly held together, Nikolsky's sign is NEGATIVE and the Bulla-spread sign is not prominent. Confirmation rests on a sub-epidermal blister on H&E (often with eosinophils) and a linear band of IgG/C3 along the basement membrane zone on DIF, with circulating anti-BP180 antibodies on ELISA.
The diagnostic signature of bullous pemphigoid:
- Onset: elderly patients; may begin as a pruritic urticarial/eczematous prodrome.
- Skin: tense bullae on erythematous or normal skin; intact blisters often present.
- Mucosa: usually spared.
- Bedside signs: Nikolsky's sign NEGATIVE; Bulla-spread sign not prominent.
- Immunopathology: linear IgG/C3 along the basement membrane zone on DIF; anti-BP180/BP230 antibodies.
Differential Diagnosis and Diagnostic Investigations
Differential Diagnosis and Workup of Vesiculobullous Lesions
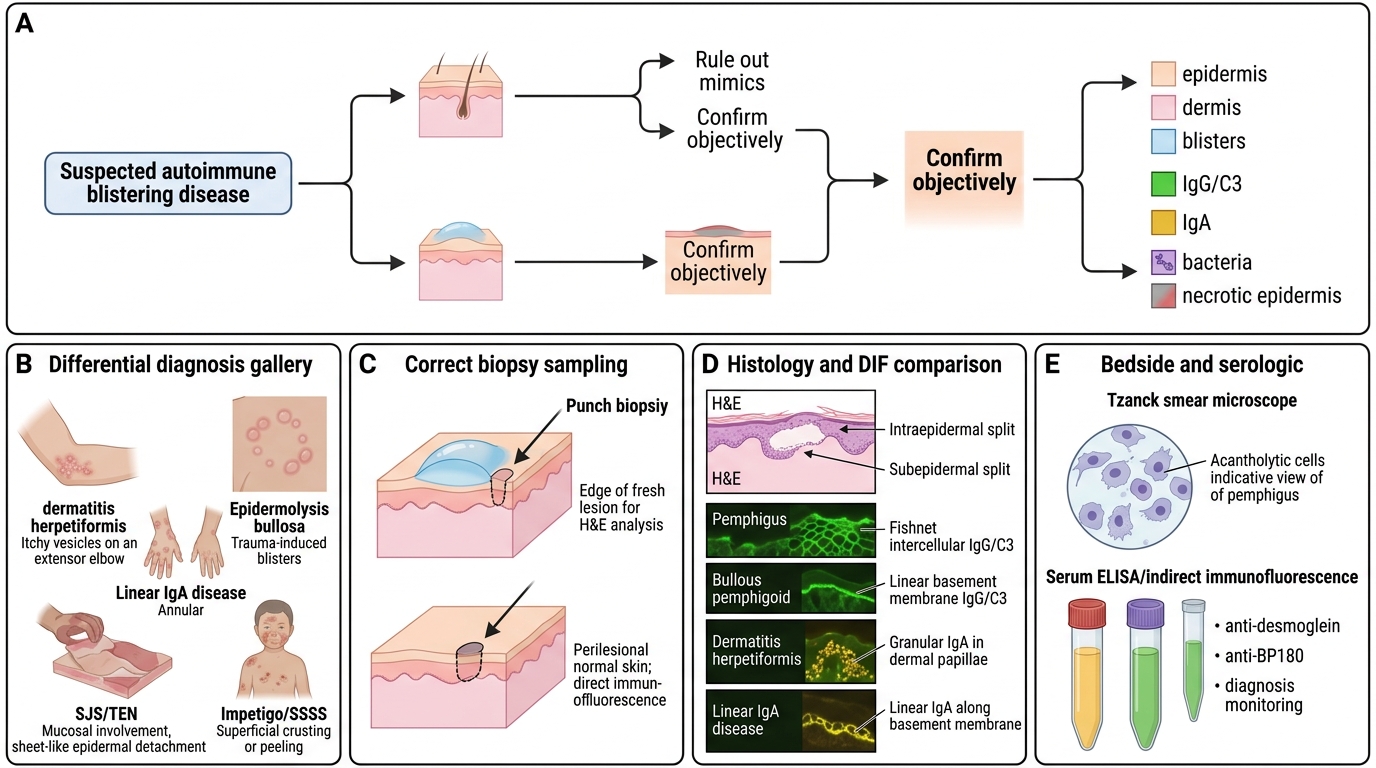
Once you suspect an autoimmune blistering disease, you must place it within a wider differential and confirm it objectively, because the morphology overlaps with several other conditions and the treatments differ sharply. The key alternatives to consider are dermatitis herpetiformis (intensely itchy grouped vesicles on extensor surfaces, IgA-mediated, linked to coeliac disease), linear IgA disease, epidermolysis bullosa (mechanobullous, often from childhood), drug-induced Stevens-Johnson syndrome / toxic epidermal necrolysis (acute, with mucosal involvement and sheet-like detachment — a Nikolsky-positive mimic driven by keratinocyte necrosis, not acantholysis), and bacterial impetigo or staphylococcal scalded skin syndrome in children. The confirmatory workhorse is the skin biopsy: one specimen from the edge of a fresh lesion for routine H&E (which shows whether the split is intra- or sub-epidermal), and a second specimen of perilesional normal skin for direct immunofluorescence (DIF), which is the gold standard for distinguishing the immunobullous diseases. A Tzanck smear gives a rapid bedside clue (acantholytic cells in pemphigus), and serum ELISA / indirect immunofluorescence quantifies circulating anti-desmoglein or anti-BP180 antibodies, useful both for diagnosis and for monitoring.
A practical investigation pathway:
- Tzanck smear from a fresh erosion — acantholytic cells support pemphigus.
- Lesional biopsy (H&E) — defines the split level: intra-epidermal (pemphigus) vs sub-epidermal (pemphigoid).
- Perilesional biopsy for DIF — intercellular fish-net IgG/C3 (pemphigus) vs linear basement-membrane IgG/C3 (pemphigoid).
- Serum ELISA / IIF — anti-desmoglein 3/1 (pemphigus) or anti-BP180/BP230 (pemphigoid); also tracks disease activity.
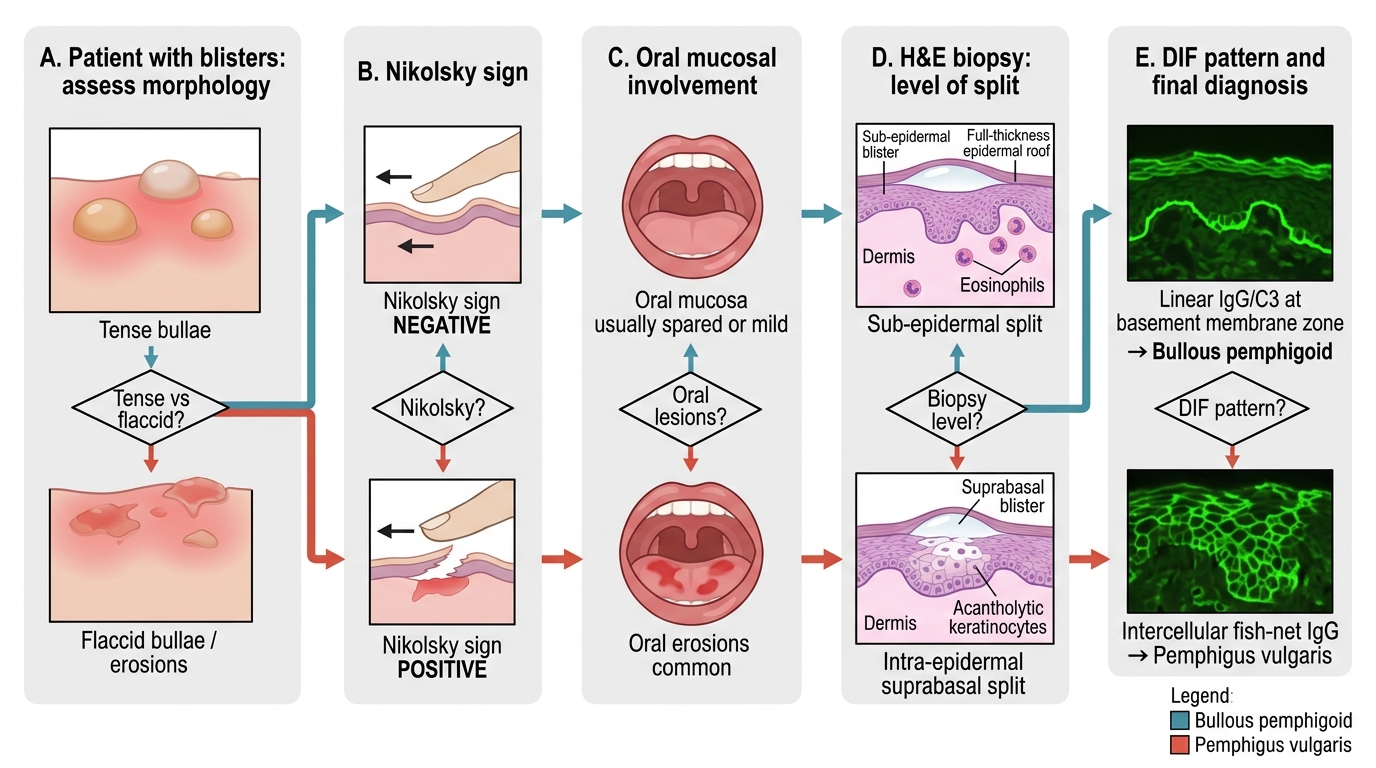
Diagnostic Algorithm for Vesiculobullous Lesions
SELF-CHECK
Which single investigation is considered the gold standard for distinguishing pemphigus vulgaris from bullous pemphigoid, and what is the characteristic finding in each?
A. Tzanck smear — acantholytic cells in both diseases
B. Routine H&E of a lesional biopsy — identical in both diseases
C. Direct immunofluorescence of perilesional skin — intercellular fish-net IgG/C3 in pemphigus vs linear basement-membrane IgG/C3 in bullous pemphigoid
D. Serum potassium — raised in pemphigus, normal in pemphigoid
Reveal Answer
Answer: C. Direct immunofluorescence of perilesional skin — intercellular fish-net IgG/C3 in pemphigus vs linear basement-membrane IgG/C3 in bullous pemphigoid
Direct immunofluorescence (DIF) on perilesional skin is the gold standard. Pemphigus vulgaris shows IgG/C3 deposited intercellularly around keratinocytes in a 'fish-net' or 'chicken-wire' pattern (reflecting anti-desmoglein antibodies); bullous pemphigoid shows a LINEAR band of IgG/C3 along the basement membrane zone (reflecting anti-BP180/BP230 antibodies). A Tzanck smear only suggests acantholysis and H&E shows the split level but not the immune pattern; neither is the definitive discriminator.
Management of Autoimmune Vesiculobullous Disorders
Management of Autoimmune Vesiculobullous Disorders
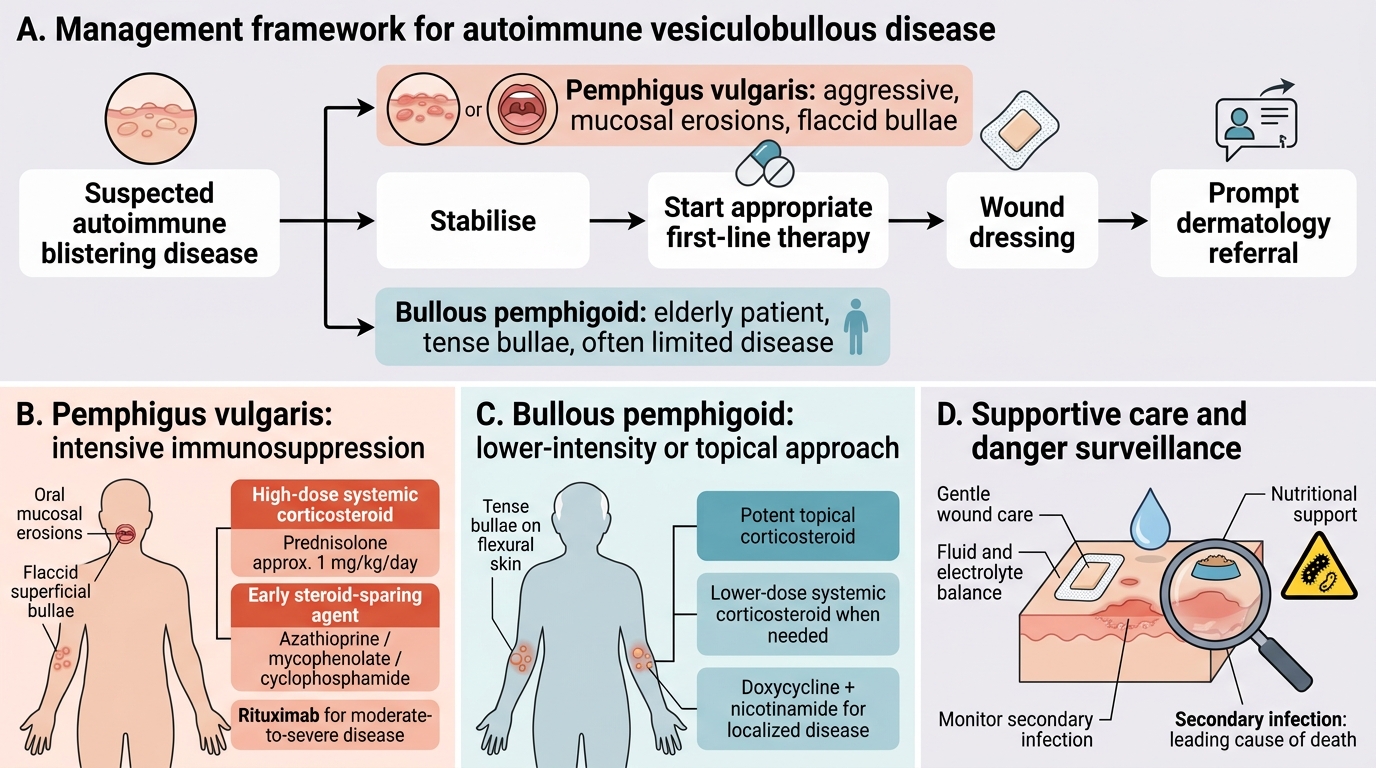
Although DR13.1 is a diagnostic competency, you must understand the management framework so that your early decisions and your referral are appropriate. The cornerstone of treatment for both diseases is systemic corticosteroids, because both are antibody-mediated and respond to immunosuppression — but the intensity differs. Pemphigus vulgaris is the more aggressive disease and generally requires high-dose corticosteroids (for example, oral prednisolone around 1 mg/kg/day) combined early with a steroid-sparing immunosuppressant such as azathioprine, mycophenolate mofetil or cyclophosphamide; rituximab is now an established option for moderate-to-severe disease in specialist hands. Bullous pemphigoid, often more limited and in frail elderly patients, may be controlled with potent topical corticosteroids or lower-dose systemic steroids, and localised disease can sometimes be managed with the anti-inflammatory combination of doxycycline and nicotinamide. Beyond drugs, both diseases demand attention to the eroded skin: gentle wound care, monitoring of fluid and electrolyte balance, nutritional support (especially when oral erosions impair eating), and vigilant surveillance for secondary infection, which remains the leading cause of death. The general practitioner's role is to stabilise, begin appropriate first-line treatment, and refer promptly to dermatology for confirmation and long-term immunosuppression.
Management priorities by disease:
- Pemphigus vulgaris: high-dose systemic corticosteroids + early steroid-sparing agent (azathioprine / mycophenolate / cyclophosphamide); rituximab for moderate-severe disease.
- Bullous pemphigoid: potent topical or lower-dose systemic corticosteroids; doxycycline + nicotinamide for milder disease.
- Both: wound care, fluid/electrolyte and nutritional support, infection surveillance, and early dermatology referral.
SELF-CHECK
An 80-year-old man has tense, intact bullae on an urticarial base over the trunk and limbs, no oral lesions, and a negative Nikolsky's sign. Which statement about his likely diagnosis is correct?
A. It is pemphigus vulgaris; expect intercellular fish-net IgG on DIF and anti-desmoglein 3 antibodies
B. It is bullous pemphigoid; expect a sub-epidermal split, linear basement-membrane IgG/C3 on DIF, and anti-BP180/BP230 antibodies
C. It is bullous pemphigoid; expect acantholytic cells on Tzanck smear and a positive Nikolsky's sign
D. It is pemphigus vulgaris because the patient is elderly and the mouth is spared
Reveal Answer
Answer: B. It is bullous pemphigoid; expect a sub-epidermal split, linear basement-membrane IgG/C3 on DIF, and anti-BP180/BP230 antibodies
Tense bullae in an elderly patient with the mouth spared and a NEGATIVE Nikolsky's sign are classic for bullous pemphigoid — a SUB-epidermal disease with linear IgG/C3 along the basement membrane on DIF and anti-BP180/BP230 antibodies. Pemphigus vulgaris would instead show flaccid bullae, oral involvement, a POSITIVE Nikolsky's sign, acantholytic cells on Tzanck smear, intercellular fish-net IgG, and anti-desmoglein antibodies. Age and mucosal sparing favour pemphigoid, not pemphigus.