Page 5 of 12
DR13.2 | Nikolsky Sign and Bulla Spread Sign — SDL Guide
Learning Objectives
- State the clinical indication for eliciting Nikolsky's sign and the Bulla-spread sign in a patient with blisters.
- Explain the biomechanical basis of each sign in terms of the level of epidermal adhesion failure.
- Demonstrate the correct bedside technique for eliciting Nikolsky's sign and the Bulla-spread (Asboe-Hansen) sign.
- Interpret positive and negative results, including the major Nikolsky-positive mimics, and recognise the signs' limitations.
- Provide structured primary management for a patient with a vesiculobullous disorder before referral — wound and oral care, fluid/electrolyte and infection management, and appropriate, timely referral.
INSTRUCTIONS
Competency DR13.2 asks you to provide primary management for a patient with a vesiculo-bullous disorder before referral. Two simple bedside signs — Nikolsky's sign and the Bulla-spread sign — sit at the front of that pathway: they cost nothing, need no equipment beyond gloves, and in seconds tell you whether you are dealing with a fragile intra-epidermal disease. But eliciting the sign is only the first half of the skill. The patient in front of you, often with extensive painful erosions, also needs immediate care — protection of denuded skin, attention to fluid and protein loss, prevention of infection, relief of oral pain — and a safe, well-timed referral to dermatology. This module trains both halves: the bedside sign as a procedure, and the primary management that must follow before the specialist takes over.
References
- Neena Khanna — Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed., Ch. on Vesiculobullous Disorders (textbook)
- IADVL Textbook of Dermatology, 4th ed., Section on Immunobullous Diseases and Clinical Examination (textbook)
- Roxburgh's Common Skin Diseases, 18th ed., Ch. on Bullous Disorders (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 42-year-old man is brought to a district hospital casualty at night with widespread raw, weeping skin and several large flaccid blisters, unable to eat because of painful mouth ulcers. The intern on duty is unsure whether this is a burn, a severe drug rash, or an infection, and is reluctant to touch the skin. You pull on gloves, place a fingertip on apparently normal skin beside a blister, and press sideways: the top layer of skin slides away under your finger. In under five seconds, that single manoeuvre — a positive Nikolsky's sign — has told you the epidermis is coming apart from within, and reframed your entire plan. But the sign is only the beginning. This man is losing fluid and protein through his denuded skin, his erosions are an open door to infection, and he cannot eat. What you do in the next hour — before any dermatologist arrives — will shape his outcome.
WHY THIS MATTERS
As the first doctor a blistering patient meets, you are expected not merely to suspect the diagnosis but to keep the patient safe until specialist care is available — which is exactly what competency DR13.2 requires. Two clinical skills carry most of that responsibility. First, eliciting Nikolsky's and the Bulla-spread signs lets you recognise a fragile, potentially severe autoimmune blistering disease at the bedside with nothing more than gloved hands. Second, and just as important, primary management before referral — protecting eroded skin, replacing fluid, preventing and treating infection, relieving oral pain and maintaining nutrition, and starting appropriate bridging treatment — is what prevents an avoidable death while the patient waits for dermatology. Sepsis from infected erosions and fluid loss across large denuded areas, not the blisters themselves, are the killers. Mastering both halves of this skill is the difference between a holding action that harms and one that saves.
RECALL
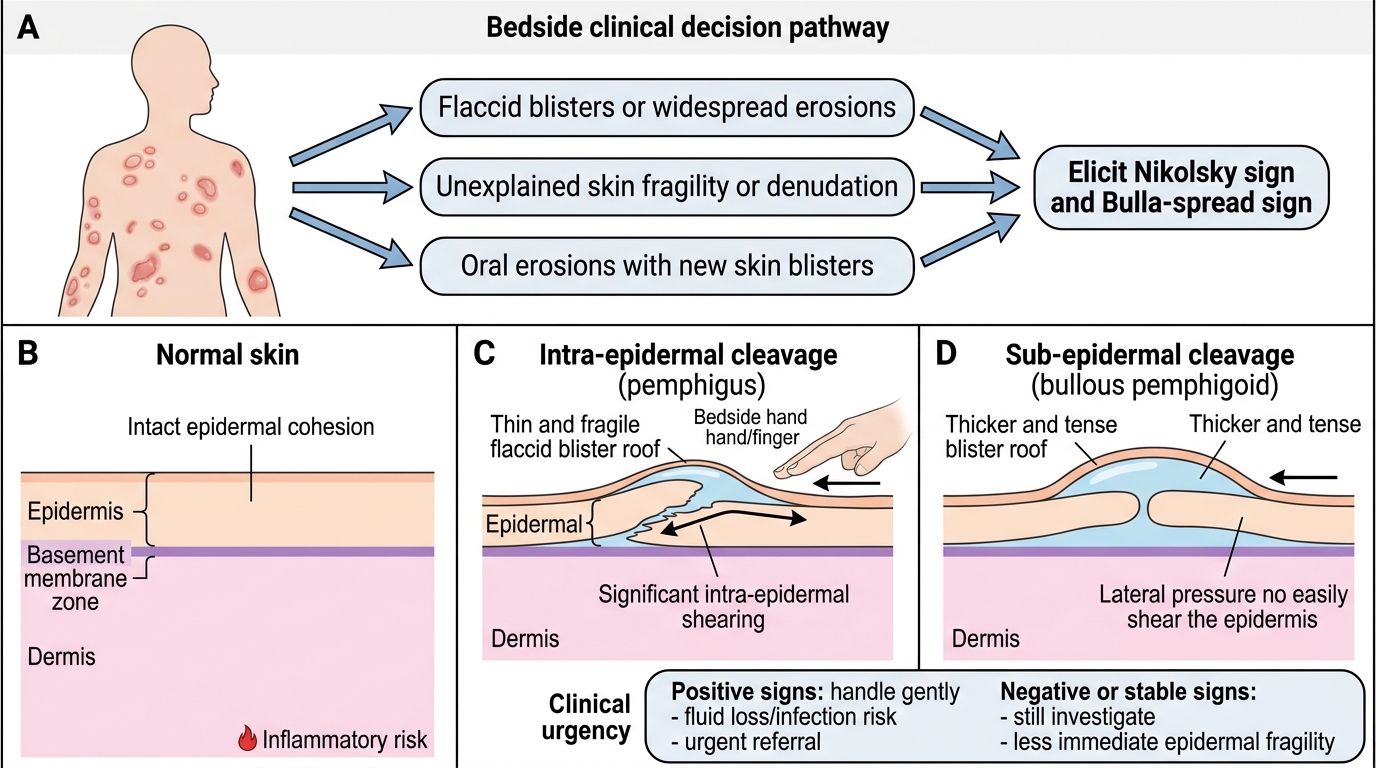
Recall from the companion diagnosis module how the level of the epidermal split determines a blister's behaviour. In pemphigus vulgaris, IgG antibodies against desmoglein 3/1 dissolve the adhesion between keratinocytes, producing an intra-epidermal (suprabasal) split — so the epidermis is mechanically fragile and shears easily. In bullous pemphigoid, IgG antibodies against BP180/BP230 attack the hemidesmosomes anchoring epidermis to dermis, producing a deeper sub-epidermal split — but the epidermis itself stays firmly stuck together, so its surface does not shear under sideways pressure. Hold onto that contrast, because it is the entire mechanical explanation for why Nikolsky's sign is POSITIVE in pemphigus and NEGATIVE in bullous pemphigoid. Recall too, from your surgery and physiology learning, that large areas of lost skin behave like partial-thickness burns: they leak fluid and protein and admit bacteria — the basis for the primary management you will give.
Clinical Indication: When and Why to Elicit Nikolsky and Bulla-Spread Signs
When to Elicit Nikolsky and Bulla-Spread Signs
The first question to settle is when these signs are worth eliciting and what decision their result will drive. You reach for Nikolsky's sign and the Bulla-spread sign whenever a patient presents with blisters, widespread erosions, or unexplained skin fragility — the very situations where you must quickly judge how serious the underlying disease is and how urgently to act. Their value is that they are immediate and free: they let you separate, at the bedside and before any laboratory result, a fragile intra-epidermal process (in which the epidermis shears apart, as in pemphigus) from a more stable sub-epidermal one (as in bullous pemphigoid). That distinction matters because it shapes how gently you must handle the skin, how worried you should be about extensive fluid loss and infection, and how quickly you arrange referral and confirmatory tests. A positive sign in a patient with extensive erosions tells you that you are dealing with a potentially life-threatening disease that needs careful primary management now and prompt specialist involvement.
Reach for these signs when you see:
- Flaccid blisters or widespread erosions suggesting an intra-epidermal process.
- Unexplained skin fragility or denudation where a burn, drug reaction or autoimmune disease is possible.
- Non-healing oral erosions with new skin blisters — a common pemphigus presentation.
- Any blistering patient in whom you must rapidly judge severity and referral urgency.
Principle: Epidermal Adhesion and the Mechanical Basis of the Signs
Mechanical Basis of Nikolsky and Bulla-Spread Signs
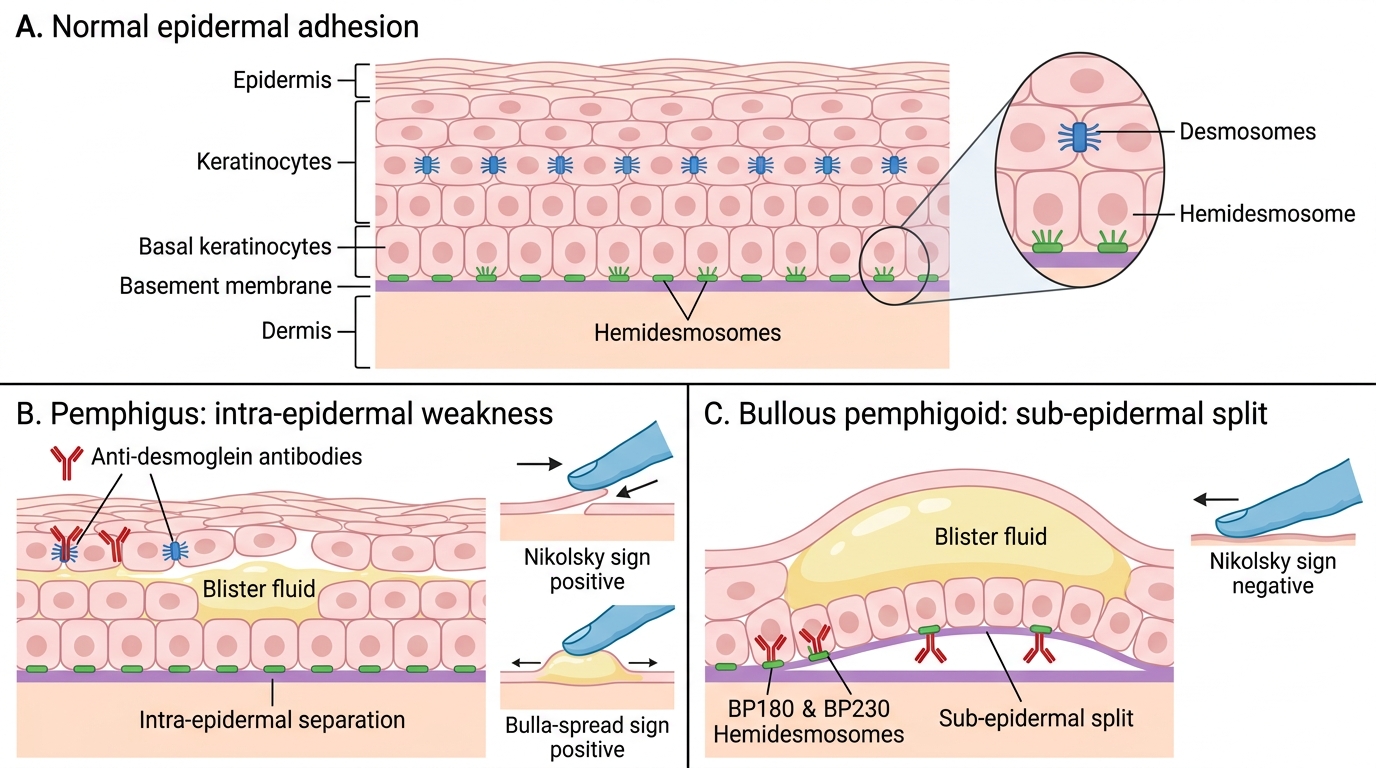
Both signs are pure applied anatomy: they probe how strongly the layers of the skin are stuck together, so understanding the adhesion explains the result without any memorisation. Keratinocytes are bound to one another by desmosomes (anchored by the desmogleins) and the basal layer is fixed to the dermis by hemidesmosomes (which include BP180 and BP230). When anti-desmoglein antibodies in pemphigus weaken keratinocyte-to-keratinocyte adhesion, the epidermis becomes internally fragile: sliding pressure on the surface makes the upper epidermis shear off (a positive Nikolsky's sign), and pressure on an intact blister lets fluid track easily through the loosened intra-epidermal plane, spreading the bulla sideways (a positive Bulla-spread sign). In bullous pemphigoid the antibodies attack the deeper hemidesmosomal anchorage, but the keratinocytes above remain tightly bound, so the surface does not shear under lateral pressure and Nikolsky's sign is NEGATIVE. No special equipment is needed — only clean gloved hands, good lighting, and a gentle, controlled touch. The skill lies entirely in applying the right kind and amount of pressure and reading the response.
The mechanical logic in brief:
- Intra-epidermal weakness (pemphigus, anti-desmoglein) → surface shears → Nikolsky POSITIVE; bulla spreads easily → Bulla-spread positive.
- Sub-epidermal split with intact epidermis (bullous pemphigoid, anti-BP180/BP230) → surface holds → Nikolsky NEGATIVE; bulla does not spread readily.
- Equipment: gloves and good lighting only — no instruments required.
SELF-CHECK
Why is Nikolsky's sign positive in pemphigus vulgaris but negative in bullous pemphigoid?
A. Pemphigus has a sub-epidermal split while pemphigoid is intra-epidermal, so pemphigus skin is more fragile
B. In pemphigus, anti-desmoglein antibodies weaken adhesion BETWEEN keratinocytes (intra-epidermal), so the surface shears; in pemphigoid the keratinocytes stay bound and only the deeper sub-epidermal junction is attacked, so the surface holds
C. Pemphigoid antibodies target desmoglein and pemphigus antibodies target BP180
D. Both signs depend on blood pressure rather than skin adhesion
Reveal Answer
Answer: B. In pemphigus, anti-desmoglein antibodies weaken adhesion BETWEEN keratinocytes (intra-epidermal), so the surface shears; in pemphigoid the keratinocytes stay bound and only the deeper sub-epidermal junction is attacked, so the surface holds
Nikolsky's sign tests adhesion within the epidermis. In pemphigus vulgaris, IgG against desmoglein 3/1 loosens keratinocyte-to-keratinocyte adhesion (an INTRA-epidermal defect), so lateral pressure shears the surface — POSITIVE. In bullous pemphigoid, IgG against BP180/BP230 attacks the deeper hemidesmosomal (SUB-epidermal) anchorage while the keratinocytes above stay firmly bound, so the surface does not shear — NEGATIVE. The option reversing the split levels or swapping the target antigens is incorrect.
Technique: Eliciting Nikolsky Sign and Bulla-Spread Sign Step-by-Step
Eliciting Nikolsky Sign and Bulla-Spread Sign
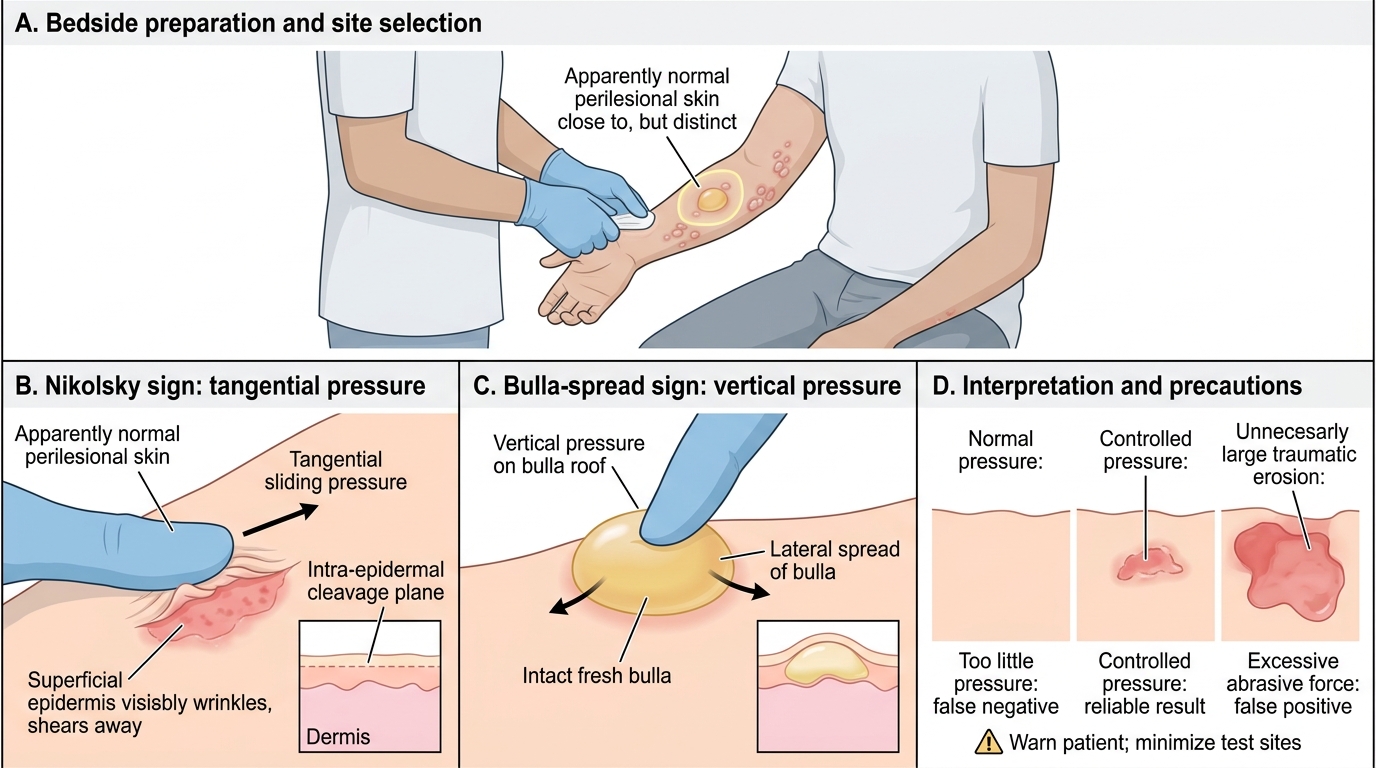
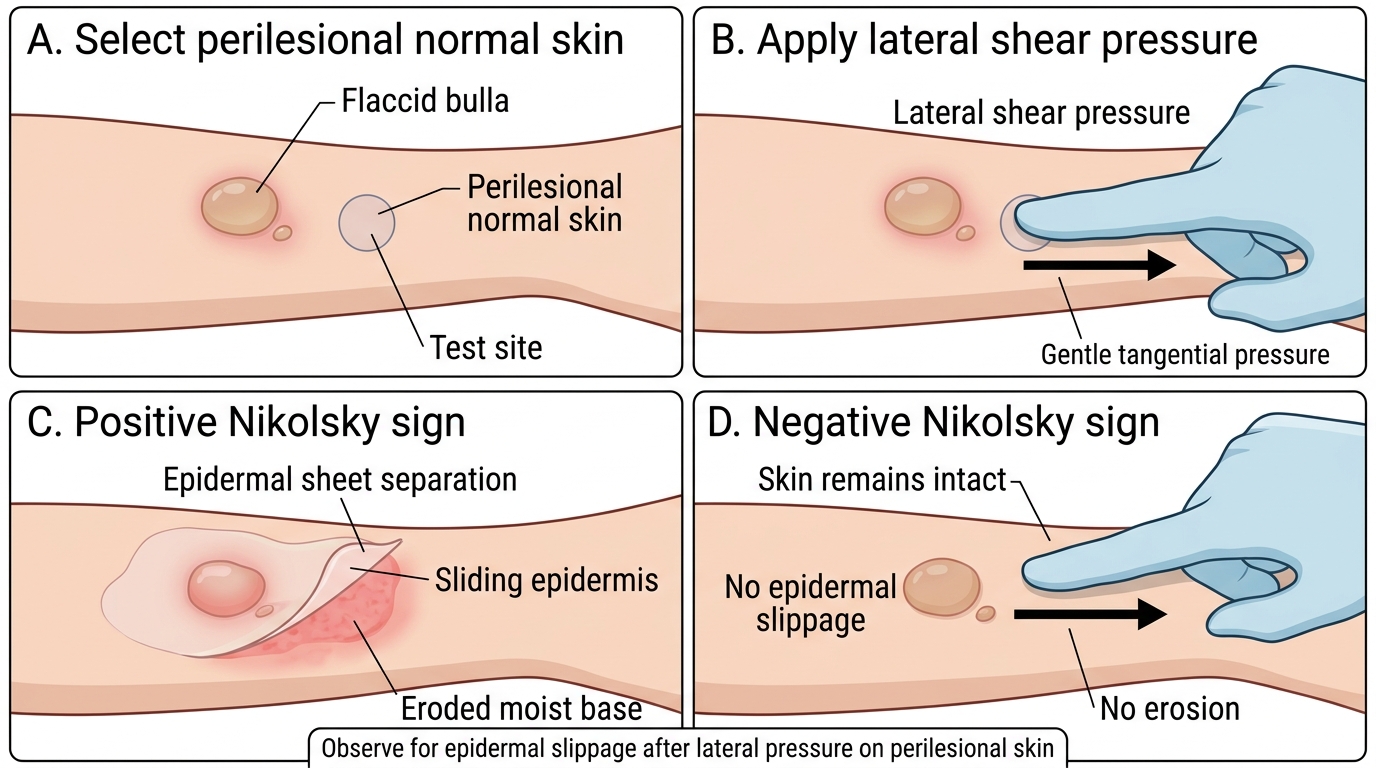
Performed carelessly, these signs mislead; performed correctly, they are reliable and reproducible, so technique matters. To elicit Nikolsky's sign, put on gloves, choose an area of apparently normal skin close to (but not on) a lesion, and apply firm but gentle tangential (sliding, sideways) pressure with a fingertip or thumb, watching whether the superficial epidermis wrinkles and slides off to leave a moist erosion. A clean shearing-away is a positive result; if the skin stays intact the sign is negative. To elicit the Bulla-spread (Asboe-Hansen) sign, find an intact, fresh bulla and apply gentle vertical (downward) pressure on its roof, observing whether the blister extends laterally into adjacent skin — lateral spread is positive, indicating that fluid is tracking through a loosened intra-epidermal plane. Two errors are common and opposite: too little pressure gives a false-negative Nikolsky's sign, while excessive, abrasive force can shear even normal skin and give a false-positive — so apply controlled pressure, compare with truly normal skin, and document exactly what you did and saw. Always warn the patient and minimise the number of sites tested, because each positive test creates a new erosion.
Step-by-step at the bedside:
- Prepare: glove up, ensure good lighting, explain to the patient, and select perilesional normal-looking skin.
- Nikolsky's sign: apply firm, gentle tangential (sliding) pressure; observe for the epidermis shearing off (positive) or staying intact (negative).
- Bulla-spread sign: apply gentle downward pressure on an intact fresh bulla; observe for lateral extension (positive).
- Avoid pitfalls: not too gentle (false negative) and not abrasive (false positive); test the fewest sites needed and document the technique and result.
Nikolsky Sign: Step-by-Step Clinical Demonstration