Page 6 of 12
DR13.2 | Nikolsky Sign and Bulla Spread Sign — SDL Guide (Part 2)
Interpreting Findings: What a Positive or Negative Result Means
Provided image
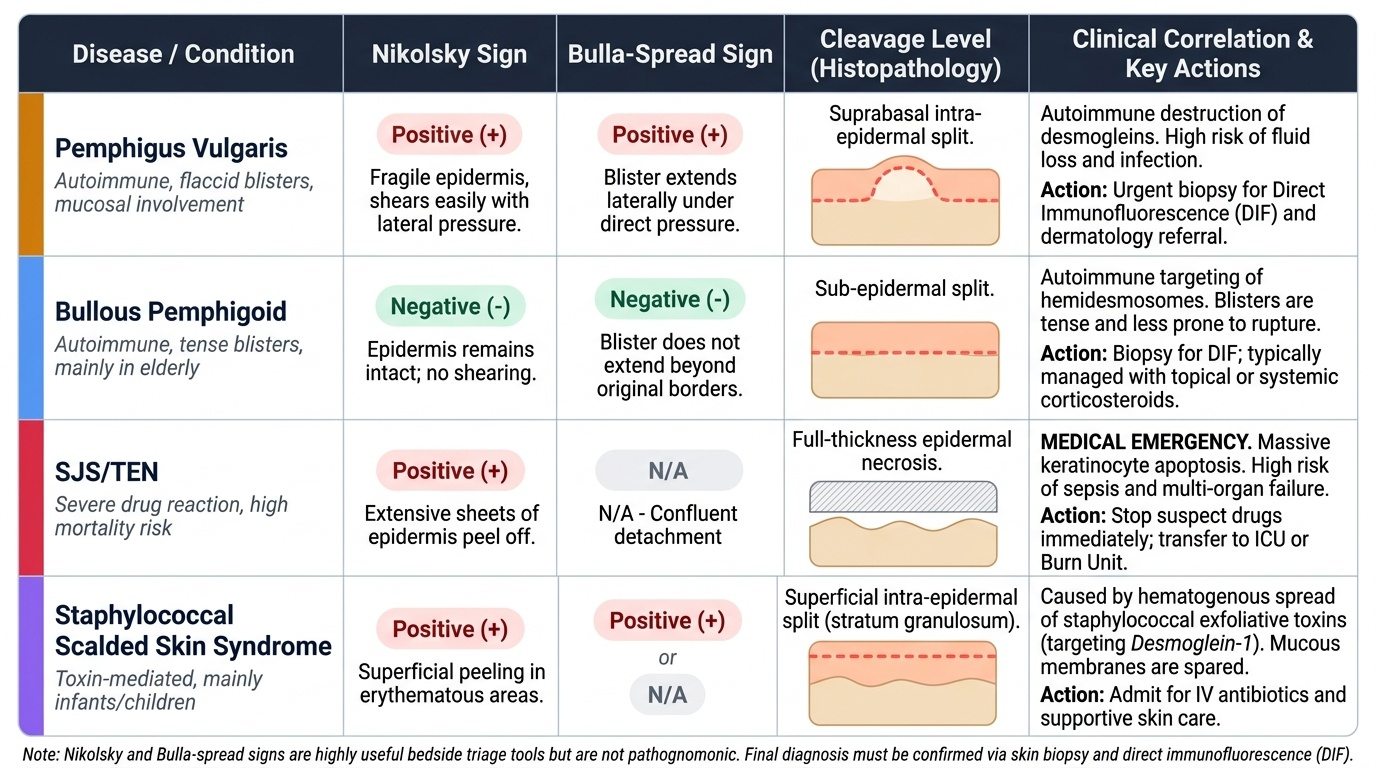
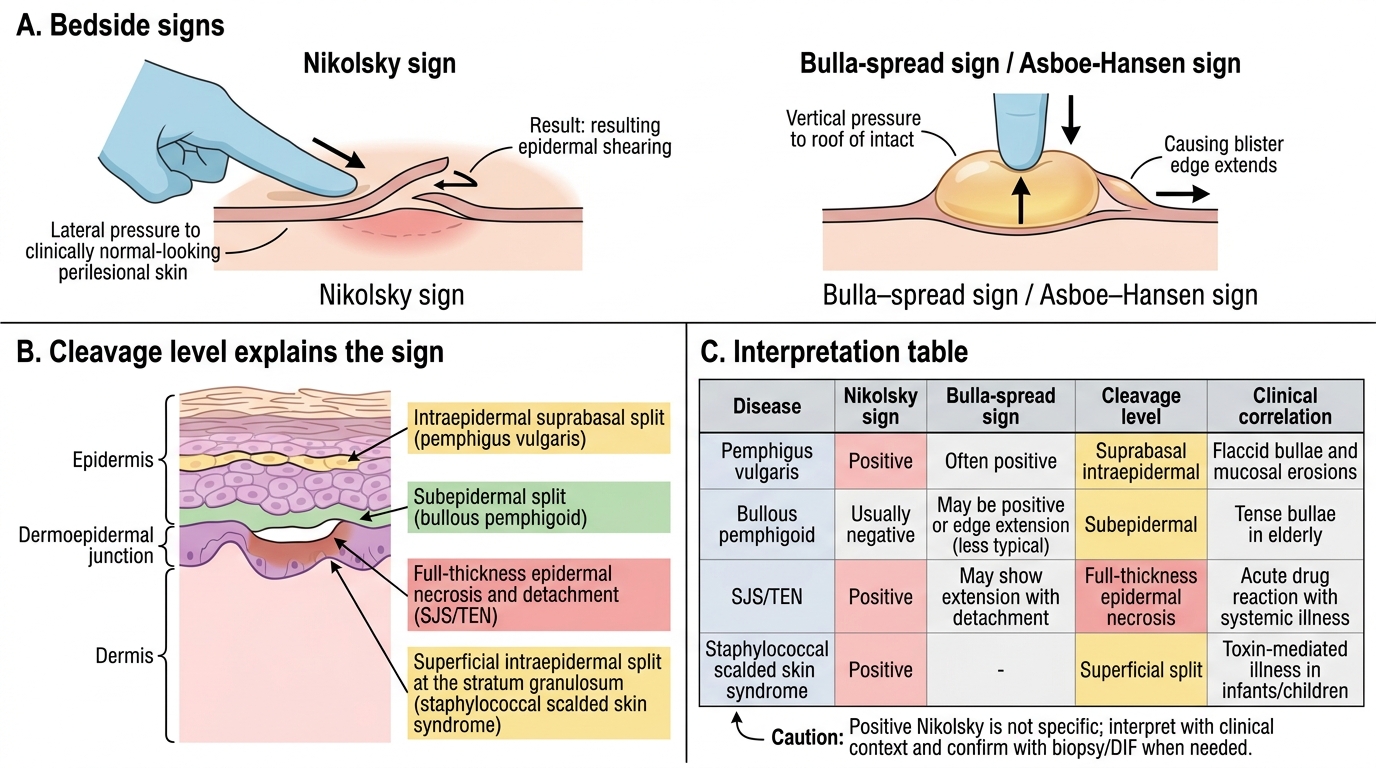
A sign is only as useful as your interpretation of it, and these two must always be read alongside the clinical picture rather than in isolation. A positive Nikolsky's sign indicates that the epidermis is fragile and shears easily, which points to an intra-epidermal process — classically pemphigus vulgaris — and, when extensive, flags a potentially severe disease needing careful handling and prompt referral. A negative Nikolsky's sign in a blistering patient points instead toward a sub-epidermal disease such as bullous pemphigoid, where the epidermis stays intact. A positive Bulla-spread sign reinforces an intra-epidermal cleavage plane. Crucially, a positive Nikolsky's sign is not unique to pemphigus: it is also positive in Stevens-Johnson syndrome / toxic epidermal necrolysis (drug-induced epidermal necrosis) and in staphylococcal scalded skin syndrome (toxin-mediated, mainly in children) — both of which can be life-threatening and must be distinguished by history and context. The signs therefore triage and raise suspicion; they do not, by themselves, make a final diagnosis, which still requires biopsy with direct immunofluorescence. Treat any positive sign in an unwell patient as a prompt to act and refer, not as a reason to wait for certainty.
Reading the results:
- Nikolsky POSITIVE → fragile epidermis, intra-epidermal split → pemphigus vulgaris (also SJS/TEN, SSSS — distinguish by context).
- Nikolsky NEGATIVE → epidermis intact → sub-epidermal disease such as bullous pemphigoid.
- Bulla-spread POSITIVE → supports an intra-epidermal cleavage plane (pemphigus).
- Limitation: the signs triage and raise suspicion but are not pathognomonic — confirm with biopsy and DIF.
Nikolsky and Bulla-Spread Signs: Interpretation by Disease
SELF-CHECK
A junior doctor reports a positive Nikolsky's sign in an acutely unwell patient with widespread skin detachment and recent new medication. Which statement is correct?
A. A positive Nikolsky's sign is specific for pemphigus vulgaris, so no other diagnosis need be considered
B. A positive Nikolsky's sign also occurs in Stevens-Johnson syndrome / toxic epidermal necrolysis and in staphylococcal scalded skin syndrome, so the result must be read with the clinical context and confirmed by biopsy/DIF
C. A positive Nikolsky's sign rules out any drug reaction
D. A positive Nikolsky's sign confirms bullous pemphigoid
Reveal Answer
Answer: B. A positive Nikolsky's sign also occurs in Stevens-Johnson syndrome / toxic epidermal necrolysis and in staphylococcal scalded skin syndrome, so the result must be read with the clinical context and confirmed by biopsy/DIF
Nikolsky's sign indicates a fragile epidermis but is NOT specific to pemphigus. It is also positive in SJS/TEN (drug-induced keratinocyte necrosis) and in staphylococcal scalded skin syndrome (toxin-mediated). A recent new drug with acute widespread detachment should raise concern for SJS/TEN. The sign triages and raises suspicion; definitive diagnosis still needs biopsy with direct immunofluorescence. It never confirms bullous pemphigoid, in which the sign is negative.
Primary Management Before Referral
Primary Management Before Dermatology Referral
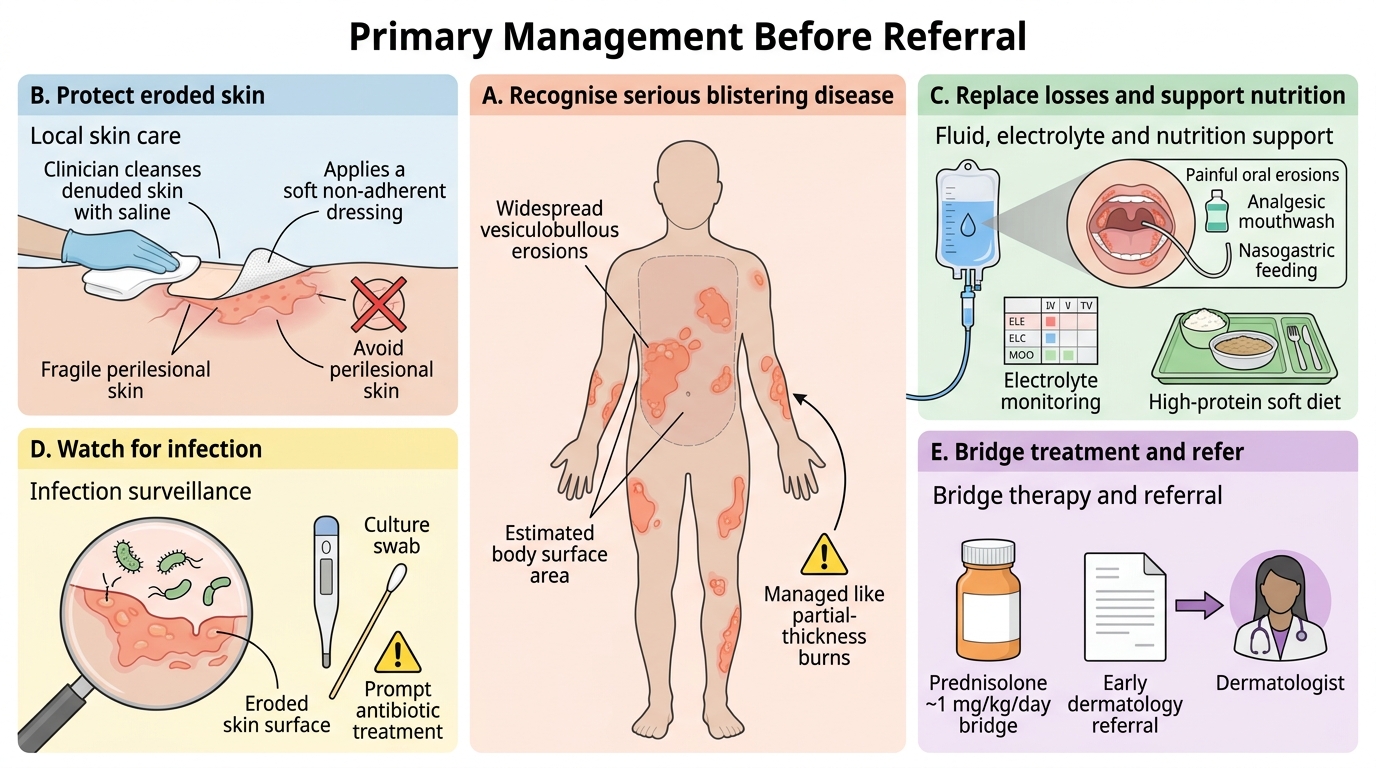
Once you have used the signs to recognise a serious blistering disease, the heart of competency DR13.2 is the primary management you provide before the dermatologist takes over — and most of this is supportive care of the eroded skin and the whole patient, not specialist drugs. Treat extensive erosions much as you would partial-thickness burns. Protect the denuded skin with gentle, non-adherent dressings and saline cleansing, and never apply adhesive tape to fragile perilesional skin, which will only enlarge the erosions. Because large raw areas leak fluid and protein, monitor fluid and electrolyte balance and give intravenous fluids when erosions are extensive; support nutrition with a high-protein soft diet, and where painful oral erosions prevent eating, use analgesic mouthwashes and consider nasogastric feeding. Erosions are a portal for infection, the leading cause of death, so practise scrupulous infection surveillance and treat secondary bacterial infection promptly. A short course of systemic corticosteroid (for example prednisolone around 1 mg/kg/day) may be started to slow active blistering as a bridge — but definitive, long-term immunosuppression is the specialist's decision, so refer early to dermatology with clear documentation. Any confirmed or strongly suspected autoimmune blistering disease, extensive erosions (a fluid-loss concern when above roughly 20-30% of body surface area), or an inability to maintain oral intake should trigger urgent referral.
Primary management checklist before referral:
- Wound/erosion care: non-adherent dressings, saline cleansing; never adhesive tape on fragile skin.
- Fluid/electrolyte: monitor balance; IV fluids for extensive erosions (treat like partial-thickness burns; concern above ~20-30% BSA).
- Oral care and nutrition: analgesic mouthwash, soft high-protein diet; nasogastric feeding if oral intake fails.
- Infection: daily surveillance of erosions; prompt antibiotics for secondary bacterial infection.
- Bridging treatment: short-course prednisolone (~1 mg/kg/day) to slow blistering — NOT definitive immunosuppression.
- Referral: refer early to dermatology with documentation; urgent if extensive erosions or failure of oral intake.
SELF-CHECK
A 45-year-old with suspected pemphigus has extensive trunk erosions and painful oral ulcers preventing him from eating or drinking. Which is the MOST appropriate primary management before dermatology referral?
A. Apply adhesive tape dressings firmly over the erosions and discharge with oral antibiotics
B. Provide non-adherent wound care, monitor and replace fluid/electrolytes, give analgesic mouthwash with nutritional support, watch for infection, consider short-course prednisolone as a bridge, and refer urgently
C. Start high-dose rituximab immediately in casualty before any referral
D. Reassure and review in one month with no fluid or nutritional assessment
Reveal Answer
Answer: B. Provide non-adherent wound care, monitor and replace fluid/electrolytes, give analgesic mouthwash with nutritional support, watch for infection, consider short-course prednisolone as a bridge, and refer urgently
Primary management before referral is supportive and protective: non-adherent (never adhesive-tape) wound care, fluid/electrolyte monitoring and replacement because extensive erosions leak like burns, analgesic mouthwash and nutritional support when oral intake fails, infection surveillance, and a short bridging course of corticosteroid to slow blistering — then prompt referral. Adhesive tape worsens erosions; rituximab and definitive immunosuppression are specialist decisions, not casualty interventions; and a one-month review with no assessment ignores the real risks of fluid loss and sepsis.
Self-Assessment: Sign Elicitation and Primary Management
Bedside Signs and Primary Management in Vesiculobullous Lesions
Consolidate both halves of this competency by reasoning through the prompts below, because DR13.2 is assessed on your ability to act, not just to recognise. Picture the patient in front of you and rehearse, in sequence, how you would elicit and interpret the bedside signs and then deliver safe primary management before referral. Hold two anchors steady as you work: first, that a positive Nikolsky's sign reflects a fragile intra-epidermal disease (classically pemphigus, but also SJS/TEN and SSSS) and a negative sign points to sub-epidermal disease such as bullous pemphigoid; and second, that the immediate threats to life in extensive blistering are fluid loss and infection, which your primary management exists to prevent. If any step feels uncertain, return to the relevant section rather than improvising, since the cost of error here is measured in avoidable harm.
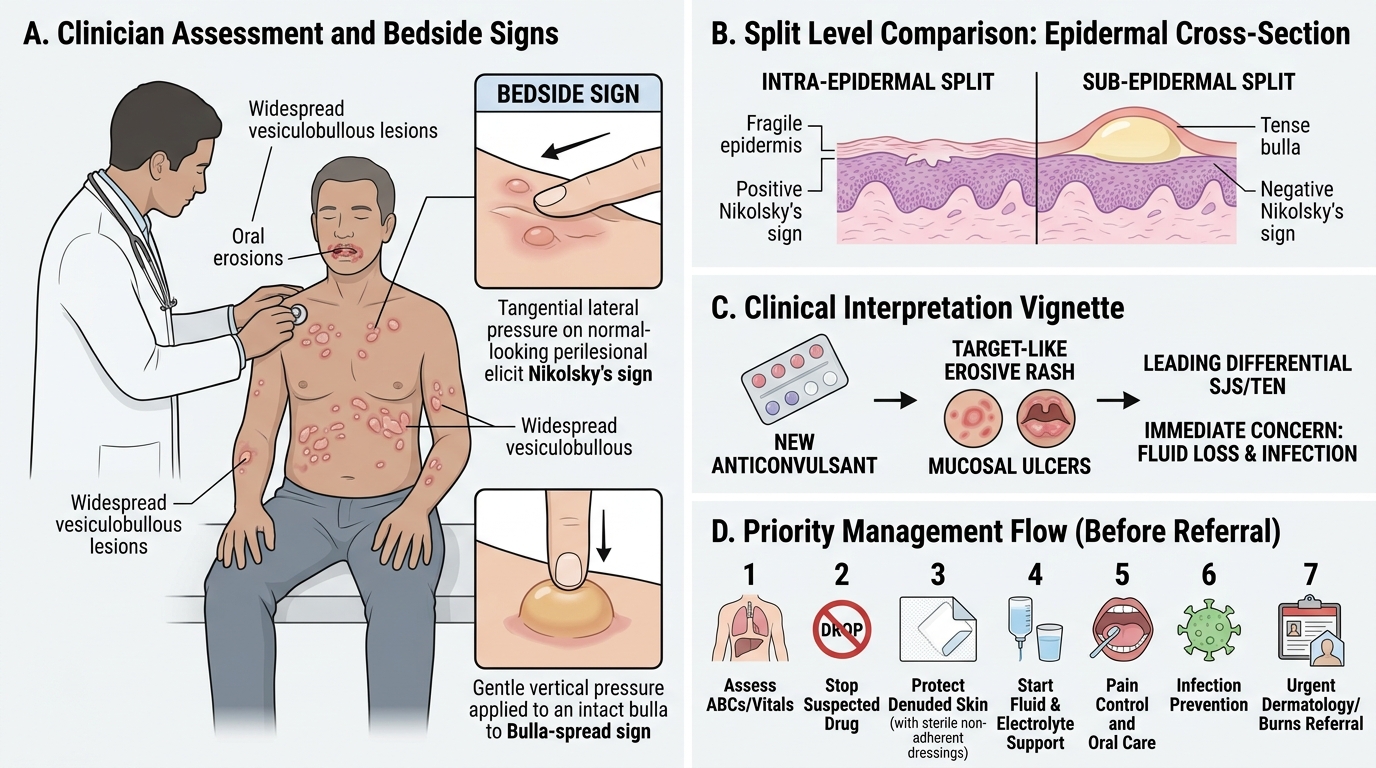
- Technique: Describe, step by step, how you would elicit Nikolsky's sign and the Bulla-spread sign, and name the two technique errors that cause false results.
- Interpretation: A patient has a positive Nikolsky's sign after starting a new anticonvulsant. State your leading differential and your immediate concern.
- Primary management: For a patient with erosions over much of the trunk and painful oral ulcers, list, in priority order, the primary management steps you would deliver before referral.
- Referral judgement: Name three findings that would make you refer this patient urgently rather than routinely.
CLINICAL PEARL
Remember that the bedside sign and the bedside care are two halves of one duty. The sign costs nothing but is not pathognomonic — a positive Nikolsky's sign points to a fragile intra-epidermal disease (pemphigus) yet is also positive in SJS/TEN and staphylococcal scalded skin syndrome, so always read it with the history and never let it substitute for biopsy and direct immunofluorescence. And the moment the sign tells you the disease is serious, your job shifts to primary management: in extensive blistering, the patient dies not of the blisters but of fluid loss and sepsis from eroded skin — so protect the skin without adhesive tape, replace fluid, guard nutrition and the airway-to-gut route when the mouth is involved, watch relentlessly for infection, and refer early. Doing the sign well but neglecting the supportive care is a half-completed competency.