Page 9 of 22
DR8.3 | Varicella Zoster Recognition — SDL Guide (Part 2)
Clinical Features and Diagnosis of Varicella and Zoster
Varicella and Herpes Zoster: Clinical Features, Distribution, and Diagnosis
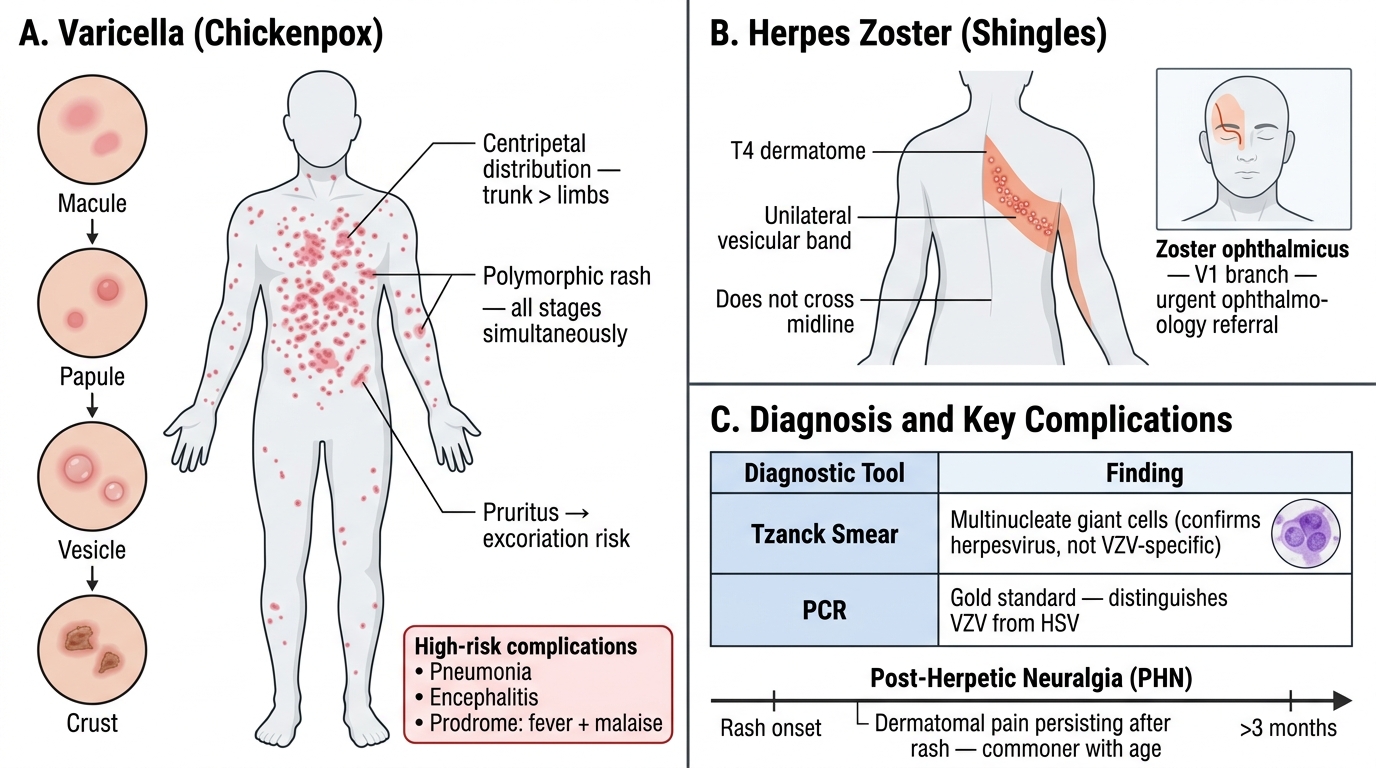
A systematic reading of clinical features confirms the diagnosis and flags the complications that change management. For varicella, beyond the polymorphic centripetal rash, note the preceding fever and malaise, the intense pruritus that risks secondary bacterial infection from scratching, and — particularly in adults, pregnant women and the immunocompromised — the risk of more serious complications including varicella pneumonia and, rarely, encephalitis. For herpes zoster, the cardinal complication is post-herpetic neuralgia (PHN) — dermatomal pain persisting for more than three months after the onset of the rash — which becomes commoner with age; zoster ophthalmicus threatens sight and warrants urgent ophthalmology referral. Diagnosis in both is usually clinical, supported where needed by a Tzanck smear (multinucleate giant cells, confirming a herpesvirus but not distinguishing VZV from HSV) and confirmed by PCR when certainty is required.
The clinical and diagnostic points are:
- Varicella: fever/malaise prodrome; polymorphic centripetal rash; pruritus → risk of secondary bacterial infection; serious complications (pneumonia, encephalitis) chiefly in adults, pregnancy and immunocompromise.
- Herpes zoster: dermatomal vesicles; post-herpetic neuralgia (pain >3 months after rash onset); zoster ophthalmicus (sight-threatening); risk rises with age and immunosuppression.
- Diagnosis: clinical in most cases; Tzanck smear (multinucleate giant cells — herpesvirus, not subtype); PCR (gold standard) and DFA when confirmation or subtyping is needed.
Differential Diagnosis and Investigations
Differential Diagnosis and Investigations of Varicella and Zoster
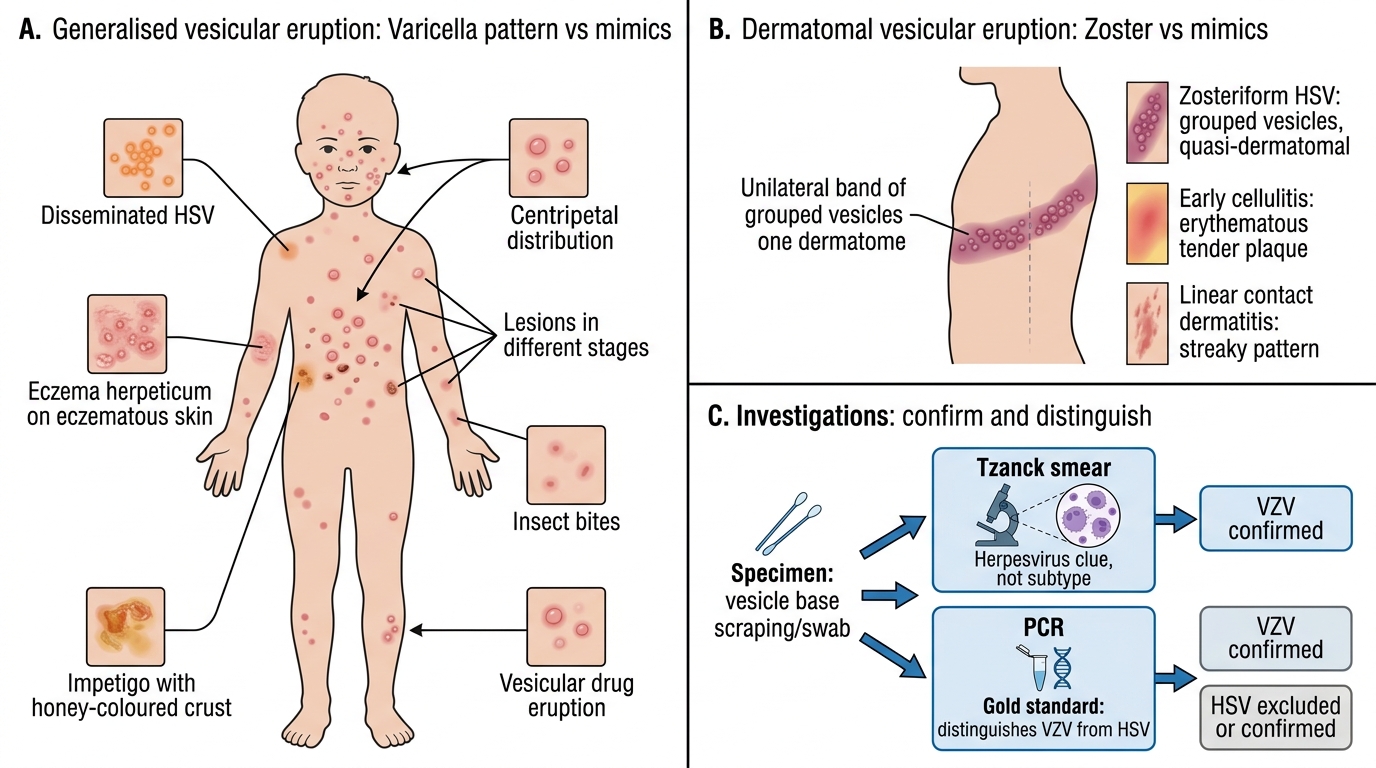
Although the classic patterns are distinctive, both varicella and zoster have mimics that disciplined differentiation will exclude. For a generalised vesicular eruption resembling varicella, consider disseminated herpes simplex, eczema herpeticum (HSV on eczematous skin), impetigo, insect bites and a vesicular drug eruption; the simultaneous-different-stages, centripetal pattern usually settles it in favour of varicella. For a dermatomal eruption resembling zoster, the chief differential is zosteriform herpes simplex — HSV can occasionally produce a grouped eruption in a quasi-dermatomal distribution, and only PCR reliably distinguishes the two — along with early cellulitis and contact dermatitis in a streaky pattern. Investigations confirm the clinical impression rather than replace it, and the choice follows the suspected diagnosis: a Tzanck smear gives a rapid herpesvirus clue, while PCR is the gold standard and is the test that distinguishes VZV from HSV when the distinction matters.
The differential and investigation points are:
- Varicella mimics: disseminated HSV, eczema herpeticum, impetigo, insect bites, vesicular drug eruption — distinguished by varicella's centripetal, multi-stage pattern.
- Zoster mimics: zosteriform herpes simplex (PCR distinguishes), early cellulitis, linear/streaky contact dermatitis.
- Investigations: Tzanck smear (multinucleate giant cells — herpesvirus, not subtype); PCR (gold standard, distinguishes VZV from HSV); DFA.
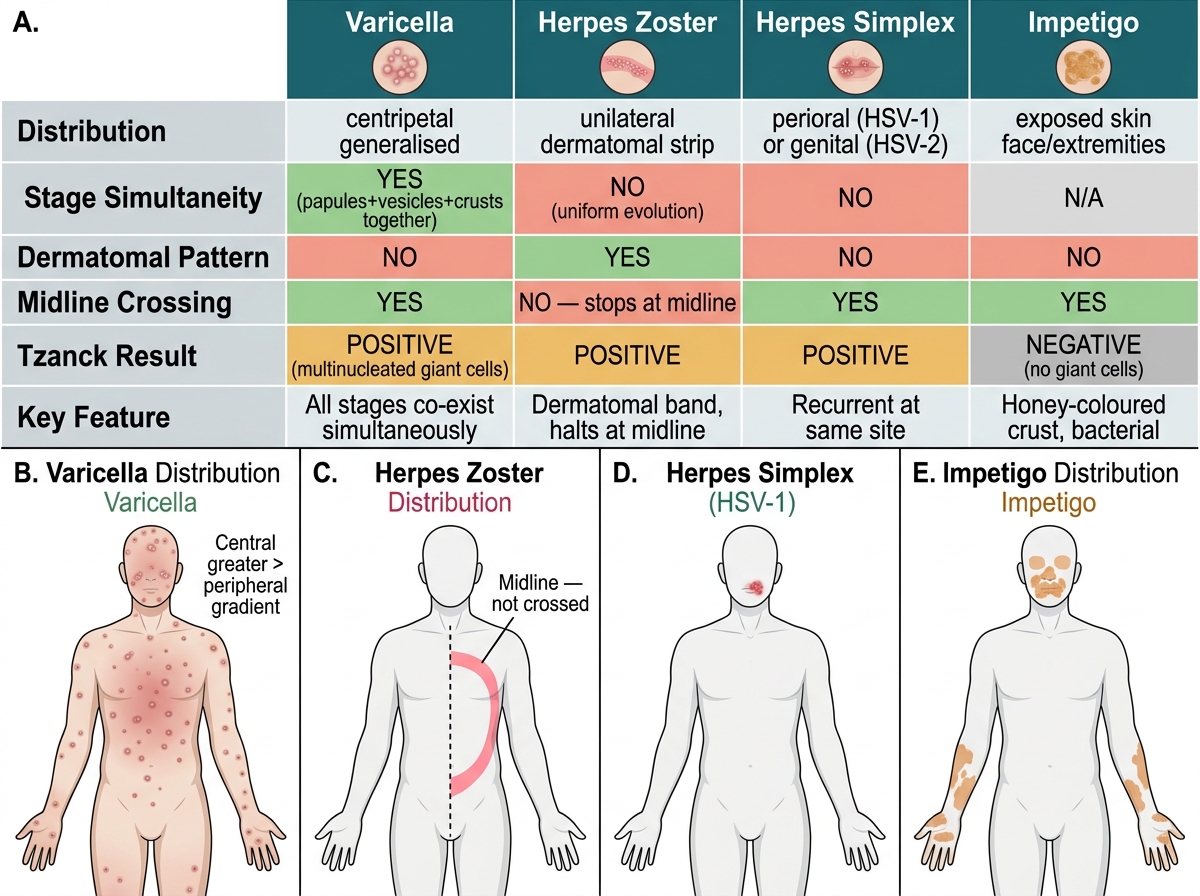
Distinguishing Features of Common Vesicular and Pustular Skin Infections
SELF-CHECK
What is post-herpetic neuralgia (PHN), and which patient group is at greatest risk?
A. Pain during the acute zoster rash only; greatest risk in children
B. Dermatomal pain persisting for more than three months after the onset of the zoster rash; greatest risk in the elderly
C. Pain caused by secondary bacterial infection of varicella lesions; greatest risk in neonates
D. Pain from zoster ophthalmicus only; greatest risk in pregnant women
Reveal Answer
Answer: B. Dermatomal pain persisting for more than three months after the onset of the zoster rash; greatest risk in the elderly
Post-herpetic neuralgia is dermatomal neuropathic pain that persists for more than three months (>90 days) after the onset of the herpes zoster rash, in the territory of the affected nerve. Its incidence and severity rise markedly with increasing age, making the elderly the group at greatest risk; immunosuppression also increases risk. It is distinct from the pain of the acute eruption and from secondary bacterial infection of varicella. Early antiviral therapy and adequate acute pain control may reduce the likelihood and severity of PHN, which is why prompt recognition of zoster matters.
Management: Antivirals, Complications and Prevention
Management and Prevention of VZV Disease
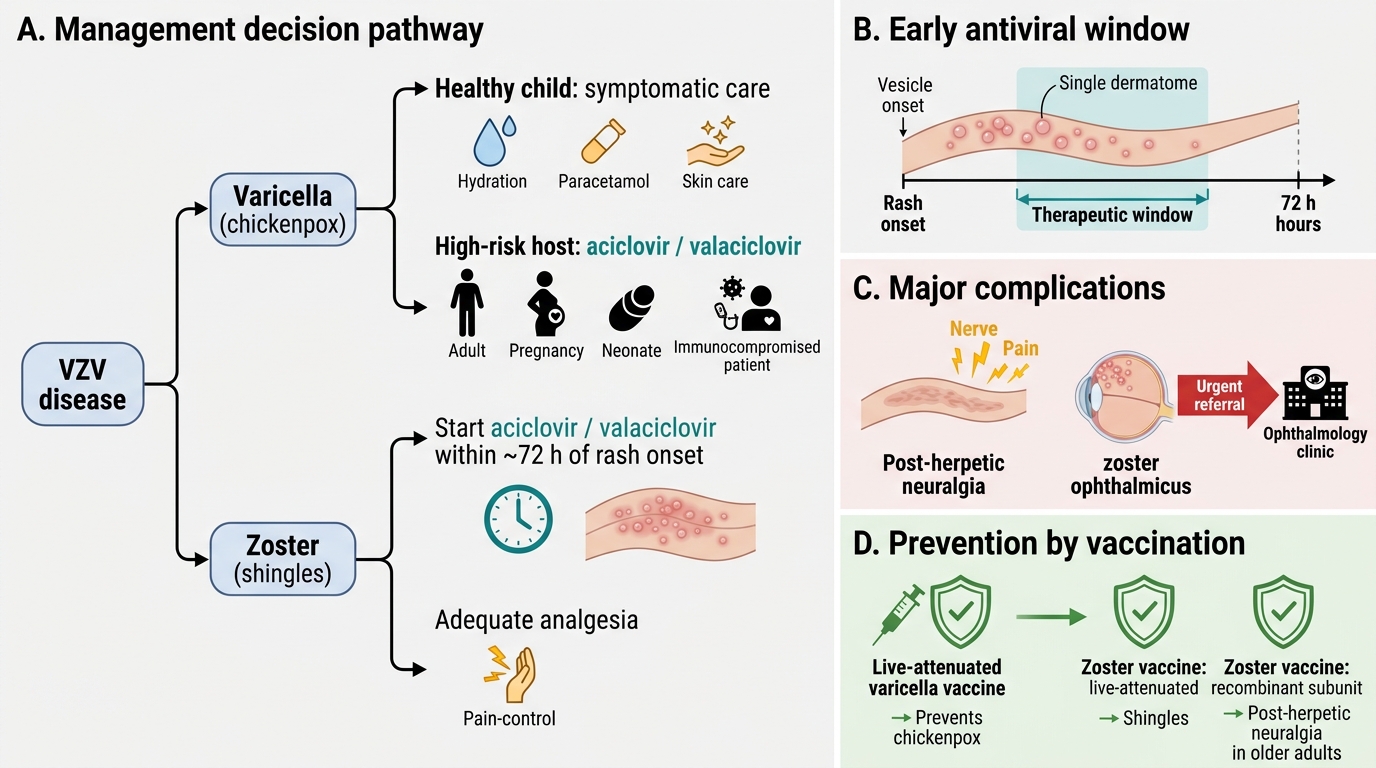
Management of VZV disease combines antiviral therapy, attention to complications, and prevention through vaccination, with the threshold for treatment depending on the host and the site. Antiviral therapy with aciclovir or valaciclovir shortens the illness and reduces complications and is most effective when started early — within 72 hours of rash onset for zoster. For varicella, antivirals are reserved largely for those at risk of severe disease (adults, pregnant women, neonates, the immunocompromised), while healthy children are usually managed symptomatically. For zoster, early antivirals plus adequate pain control are the priority, and post-herpetic neuralgia is managed with neuropathic agents. Zoster ophthalmicus requires urgent ophthalmology referral. Prevention rests on vaccination: a live-attenuated varicella vaccine prevents chickenpox, and zoster vaccines (live-attenuated or recombinant subunit) reduce the incidence of shingles and PHN in older adults.
The management principles are:
- Antivirals (aciclovir/valaciclovir): start early (within ~72 h of zoster rash); for varicella, treat those at risk of severe disease (adults, pregnancy, neonates, immunocompromised), symptomatic care for healthy children.
- Post-herpetic neuralgia: neuropathic pain agents — amitriptyline, gabapentin, pregabalin; topical lidocaine or capsaicin.
- Zoster ophthalmicus: urgent ophthalmology referral to protect sight.
- Prevention: live-attenuated varicella vaccine; zoster vaccination (live-attenuated or recombinant subunit) in older adults to reduce shingles and PHN.
- Counsel on contagion: varicella and disseminated zoster are infectious (airborne/contact); avoid contact with susceptible high-risk people (pregnant women, neonates, the immunocompromised).