Page 10 of 22
DR8.3 | Varicella Zoster Recognition — SDL Guide (Part 3)
Self-Assessment: Varicella Zoster Recognition
Recognising Varicella, Zoster and Herpes Simplex
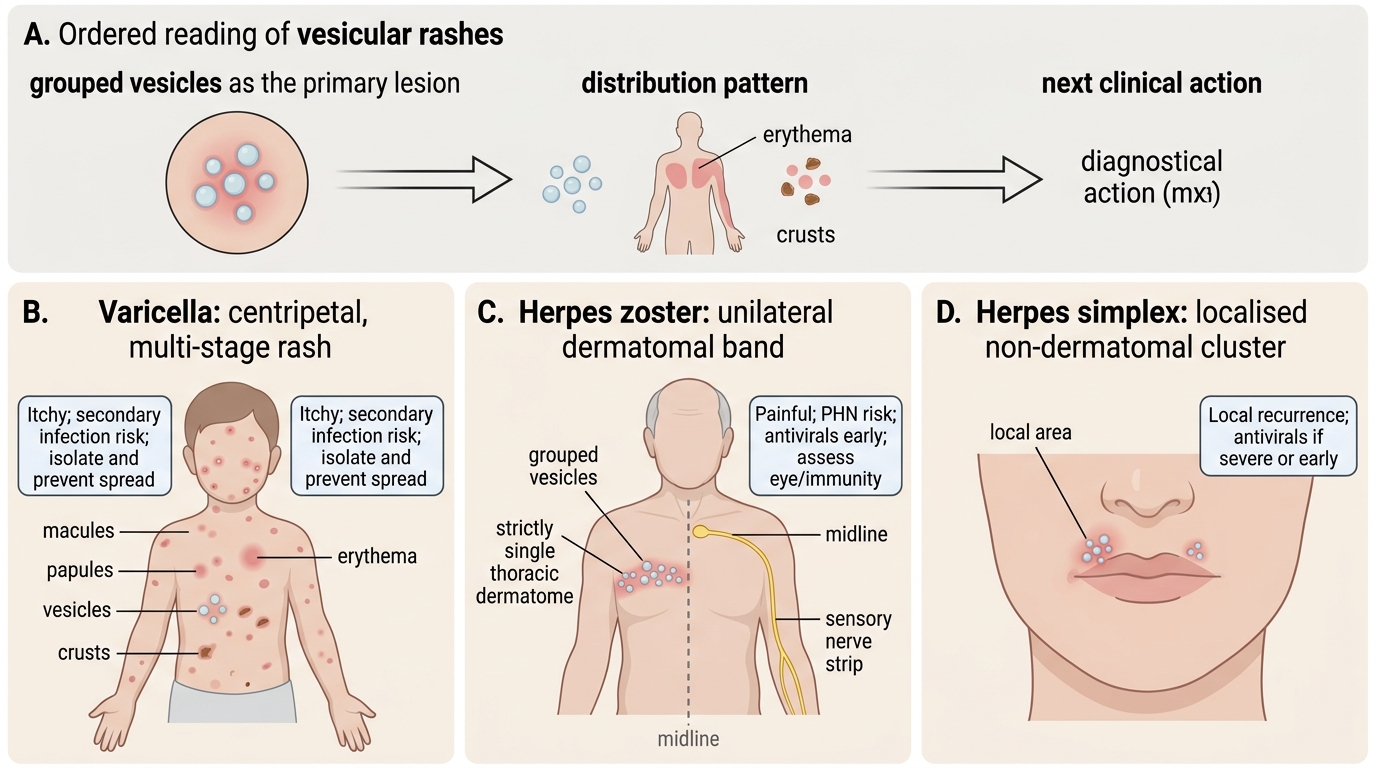
The aim of this closing section is to confirm that you can separate varicella, herpes zoster and herpes simplex on sight and choose the right next step for each. Recognition is an ordered reading: identify the primary lesion (grouped vesicles), then read the distribution — centripetal with lesions in different stages points to varicella, a unilateral dermatomal band that stops at the midline points to zoster, and a localised non-dermatomal cluster points to herpes simplex. From the pattern you then anticipate complications (post-herpetic neuralgia, zoster ophthalmicus, secondary infection) and decide on antivirals, pain control, referral and prevention. The scenarios you should be able to handle include the itchy multi-stage rash of a child with chickenpox, the painful dermatomal band in an elderly patient, and the widespread or atypical zoster that should prompt a search for immunosuppression. Use the self-check below to rehearse this sequence.
For each scenario, ask in order:
- What is the primary lesion, and what is its distribution (centripetal/multi-stage, dermatomal, or localised)?
- Does the pattern fit varicella, zoster or herpes simplex — and does it cross the midline?
- What complication must I anticipate (PHN, ophthalmicus, secondary infection), and does the host raise the risk?
- Does early antiviral therapy change the outcome here, and is referral or prevention advice needed?
SELF-CHECK
An elderly patient has a 3-day history of burning pain followed by grouped vesicles on an erythematous base along the right T5 dermatome that stop at the midline. What is the diagnosis and the most appropriate immediate management?
A. Herpes simplex; reassure, no antiviral needed
B. Herpes zoster; start aciclovir or valaciclovir early (within ~72 hours of rash onset) and provide adequate pain control
C. Varicella; isolate and treat with topical antibiotics
D. Contact dermatitis; prescribe a topical corticosteroid
Reveal Answer
Answer: B. Herpes zoster; start aciclovir or valaciclovir early (within ~72 hours of rash onset) and provide adequate pain control
A unilateral, dermatomal eruption of grouped vesicles preceded by dermatomal pain and respecting the midline is herpes zoster (VZV reactivation). The most appropriate immediate management is early antiviral therapy with aciclovir or valaciclovir — ideally within 72 hours of rash onset — which shortens the illness and reduces complications, together with adequate analgesia for the often severe pain. Herpes simplex is localised but not dermatomal; varicella is centripetal with lesions in different stages, not a single dermatomal band; and contact dermatitis is not vesicular in a strictly dermatomal, midline-respecting pattern. Early recognition and treatment also help reduce the risk of post-herpetic neuralgia.
CLINICAL PEARL
A unilateral dermatomal rash that stops at the midline is herpes zoster until proven otherwise — and the pain may precede the rash by days, masquerading as cardiac, pleuritic or abdominal pain. Start aciclovir or valaciclovir within 72 hours of rash onset to shorten the illness and cut complications. Always examine for ophthalmic-division involvement: zoster ophthalmicus is sight-threatening and needs urgent ophthalmology referral. Remember that the same virus causes chickenpox (centripetal, lesions in different stages at once) and shingles (one dermatome), and that widespread, multidermatomal or atypical zoster — especially in a young, otherwise healthy adult — should prompt a search for underlying immunosuppression such as HIV.