Page 12 of 22
DR8.4 | Viral Wart Recognition — SDL Guide
Learning Objectives
- Recognise the four clinical types of viral wart — common, plantar, plane and filiform — and their morphological signatures
- Explain HPV pathogenesis in the skin, including keratinocyte infection, koilocytes and the Koebner phenomenon
- Examine and describe each wart type by site and surface features, including thrombosed capillaries (black dots)
- Differentiate viral warts from corn/callus, molluscum contagiosum and other mimics, and outline destructive and keratolytic management
INSTRUCTIONS
Viral warts are an extremely common reason for dermatology and general-practice consultation in all age groups, and confident recognition spares patients unnecessary investigation and inappropriate treatment. This SDL builds the skill of reading the four wart types — the rough common wart, the inward-growing painful plantar wart, the flat plane wart, and the thread-like filiform wart — by their surface texture, the tell-tale black dots of thrombosed capillaries, and the disruption of skin lines. It also drills the everyday differential that trips clinicians up: distinguishing a plantar wart from a corn. Caused by HPV, warts have no systemic antiviral, so recognition leads to destructive or keratolytic treatment or to watchful waiting.
References
- Khanna N. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Viral Infections (Warts) (textbook)
- Sacchidanand S (ed). IADVL Textbook of Dermatology, 4th ed. Section: Human Papillomavirus Infections / Warts (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 12-year-old is brought in because of a painful lump on the sole of his foot that makes walking uncomfortable, and which his family has been trying to pare down for weeks, mistaking it for a corn. When you pare the surface yourself, the skin lines do not run through it — they stop at its edge — and tiny black dots appear in its centre. Those black dots are thrombosed capillaries, and they tell you this is not a corn at all but a plantar wart, caused by human papillomavirus. Recognising warts by their surface texture, their interrupted skin lines, and these characteristic black dots — and telling them apart from corns and molluscum — is the everyday skill this SDL builds.
WHY THIS MATTERS
Viral warts are one of the commonest skin complaints you will manage, in children and adults alike. They are benign but can be painful (plantar warts), cosmetically distressing (facial plane and filiform warts), socially stigmatising, and prone to spread by autoinoculation. The most frequent practical error is confusing a plantar wart with a corn — leading to the wrong treatment and ongoing pain — or confusing warts with molluscum. Because warts are caused by HPV and have no systemic antiviral cure, recognising them correctly directs you to the right management: keratolytics, cryotherapy or other destructive methods, or watchful waiting when spontaneous resolution is likely. Confident recognition saves unnecessary tests and gives patients accurate advice on a self-limiting but contagious condition.
RECALL
Recall from the viral foundations SDL and from Microbiology that human papillomavirus is a non-enveloped DNA papillomavirus that infects keratinocytes and drives them to proliferate, and that — unlike the herpesviruses — it does NOT establish latency in nerve ganglia. Recall that the histological hallmark of HPV infection is the koilocyte (a keratinocyte with a perinuclear clear halo), and that warts spread by direct contact and autoinoculation, so they characteristically appear along lines of trauma (the Koebner phenomenon). Recall too that, because warts are local epidermal proliferations rather than vesicular eruptions, a Tzanck smear is not relevant — there are no multinucleate giant cells. Keep these mechanisms in mind; they explain the surface features and spread pattern you will learn to recognise.
Recognising Viral Warts: Common, Plantar, Plane and Filiform
Clinical Morphology and Growth Patterns of the Four Viral Wart Types
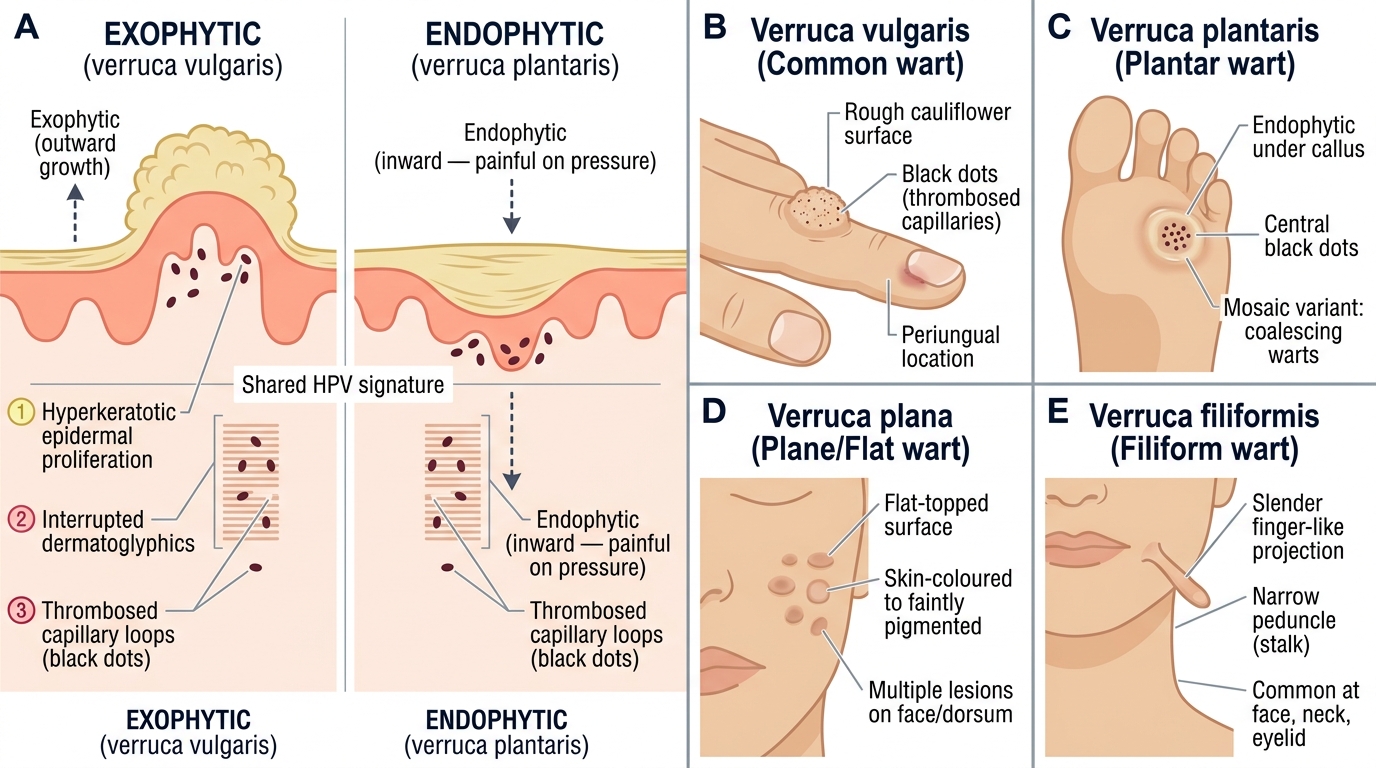
Viral warts come in four clinical types whose differing appearances all share a unifying signature: a hyperkeratotic epidermal growth in which the normal skin lines (dermatoglyphics) are interrupted rather than running through the lesion, often studded with tiny black dots that are thrombosed capillaries. Learning to read this signature, and then to place the lesion into one of the four types by its site and surface, is the core recognition skill. The growth pattern differs strikingly between types — the common wart is exophytic (grows outward into a rough cauliflower surface), whereas the plantar wart is endophytic (grows inward under the pressure of body weight, which is why it hurts) — and recognising the growth direction is part of the picture.
The four types and their signatures are:
- Verruca vulgaris (common wart): a firm, rough, hyperkeratotic, exophytic papule with a cauliflower-like surface and black dots; commonly on the dorsum of the hands, fingers and around the nails (periungual).
- Verruca plantaris (plantar wart): an inward-growing (endophytic) hyperkeratotic lesion on the sole, painful on direct pressure, with central black dots; a 'mosaic' variant is several coalescing plantar warts.
- Verruca plana (plane/flat wart): small, flat-topped, skin-coloured or slightly pigmented papules, often multiple, on the face and dorsum of the hands, frequently arranged in lines (Koebner).
- Filiform wart: thread-like, finger-shaped projections, typically perioral, perinasal or on the eyelids.
Clinical Morphology of Viral Wart Types
HPV Pathogenesis in the Skin

HPV Pathogenesis in Cutaneous Warts
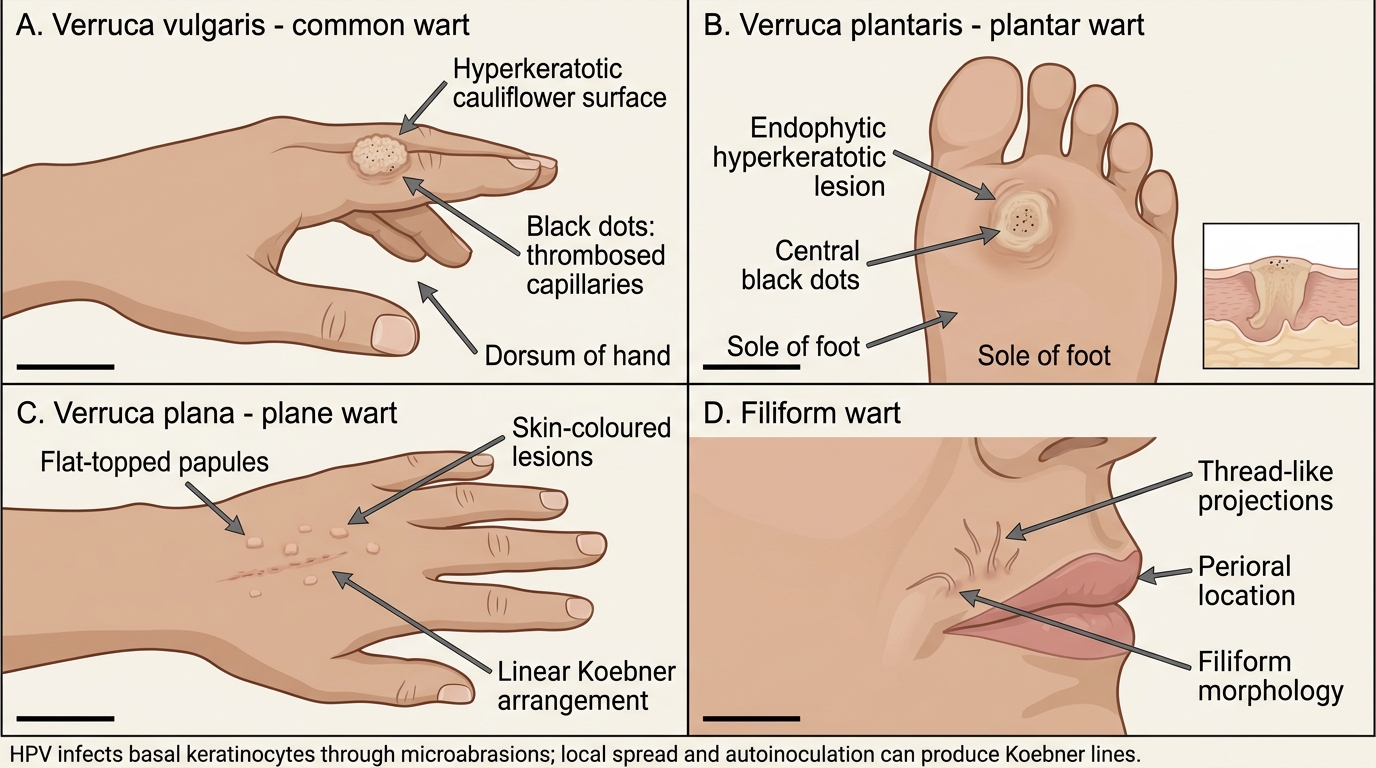
The surface features and the spread pattern of warts both follow directly from how HPV behaves in the epidermis, so a brief grasp of the pathogenesis makes recognition more intelligible. HPV enters the basal keratinocytes through tiny breaks or abrasions in the skin — which is why warts favour sites of friction and trauma such as the hands and the soles. As the infected basal cells divide and their daughter cells differentiate and migrate toward the surface, the virus drives excess proliferation and abnormal keratinisation, building up the thickened, verrucous lesion. The histological signature of this process is the koilocyte, a superficial keratinocyte with a characteristic perinuclear clear halo. Importantly, HPV does not travel to or hide in nerve ganglia, so warts have no latency–reactivation cycle; instead they spread locally and by autoinoculation, seeding new lesions along scratch lines — the Koebner phenomenon — and to contacts by direct skin contact.
The pathogenetic points that explain recognition are:
- HPV infects basal keratinocytes via skin microabrasions → favours friction/trauma sites (hands, soles).
- Virus-driven proliferation and abnormal keratinisation build the hyperkeratotic verrucous lesion; koilocytes are the histological hallmark.
- No ganglion latency — warts spread locally, by autoinoculation along trauma lines (Koebner phenomenon) and by contact, not by nerve-territory recurrence.
- The black dots seen clinically are thrombosed dermal capillaries within the proliferating lesion.
SELF-CHECK
Why do new plane (flat) warts often appear in a straight line along a scratch mark?
A. Because HPV reactivates from a nerve ganglion along the dermatome
B. Because the virus spreads by autoinoculation into the broken skin of the scratch — the Koebner phenomenon
C. Because plane warts are caused by a poxvirus that replicates in the cytoplasm
D. Because thrombosed capillaries migrate along the line of the scratch
Reveal Answer
Answer: B. Because the virus spreads by autoinoculation into the broken skin of the scratch — the Koebner phenomenon
Warts spread by direct contact and autoinoculation: HPV from an existing lesion is implanted into broken skin, so scratching seeds the virus along the scratch line, producing a row of new warts. This is the Koebner phenomenon (the isomorphic response), and plane warts show it particularly well. HPV does not establish ganglion latency, so there is no dermatomal reactivation (that is a herpesvirus behaviour); warts are not caused by a poxvirus (that is molluscum); and thrombosed capillaries are a feature within lesions, not a mechanism of linear spread.
Clinical Features: Type-by-Type Examination
Clinical Examination of Common Warts
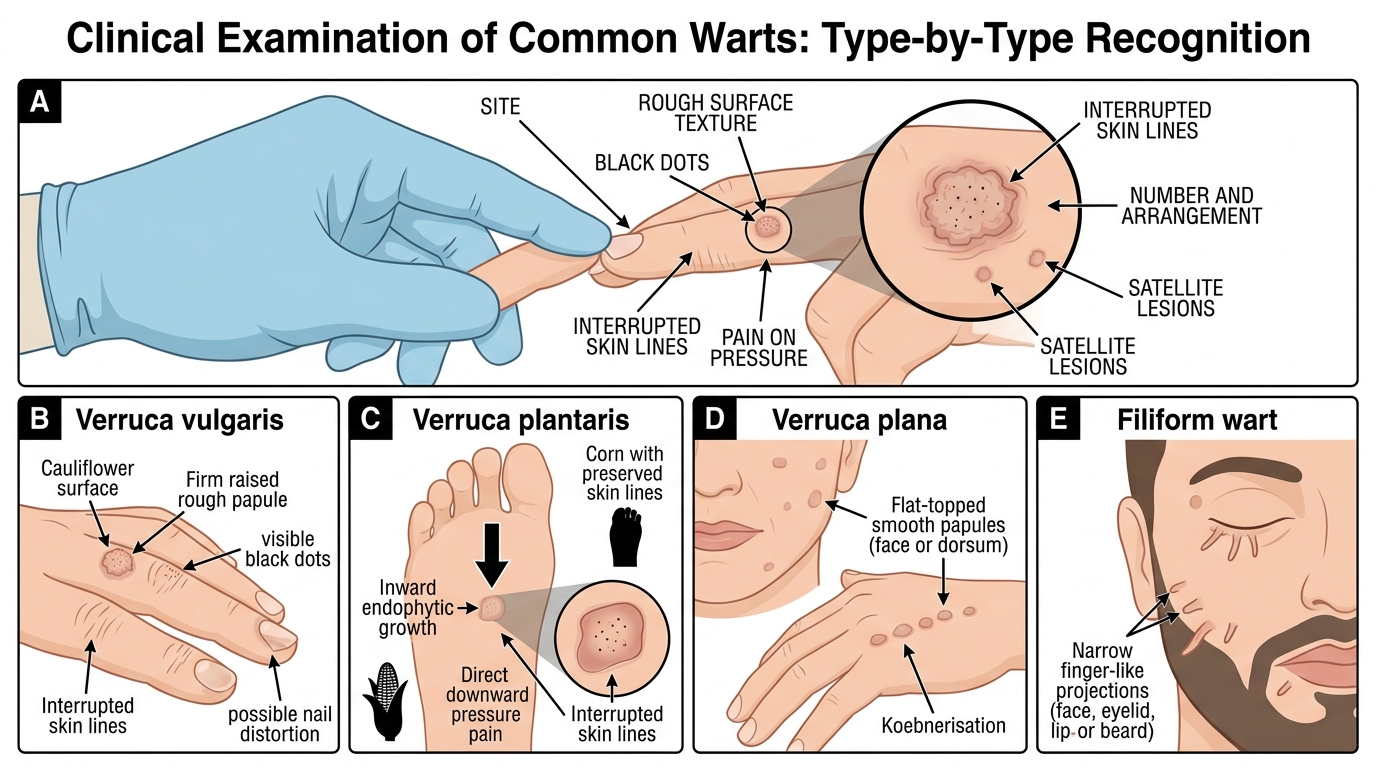
Examining a wart systematically — site, surface texture, the presence of black dots, the behaviour of the skin lines, and pain on pressure — both confirms that it is a wart and identifies which type, and this disciplined reading is what separates confident recognition from guesswork. The same paring manoeuvre that reveals black dots and interrupted skin lines also helps distinguish a plantar wart from a corn at the bedside, which is why gentle paring is part of the examination rather than only of treatment. A good examination also notes the number and arrangement of lesions (solitary, multiple, or linear from Koebnerisation), since the distribution itself often points to the type, and it checks neighbouring skin for satellite lesions that betray autoinoculation. Each of the four types has a characteristic examination profile that you should be able to elicit and describe, and rehearsing these profiles is what makes recognition quick and reliable in the clinic.
The type-by-type examination findings are:
- Verruca vulgaris: firm, rough, raised papule with a cauliflower surface and visible black dots; interrupted skin lines; common on the dorsum of hands, fingers and periungually (where it can distort nail growth).
- Verruca plantaris: on the sole, often flush with the surface because of inward (endophytic) growth under pressure; painful on direct (downward) pressure; paring reveals central black dots and a sharp margin where the skin lines stop; the mosaic variant is a plaque of coalescing warts.
- Verruca plana: multiple small, flat-topped, skin-coloured to light-brown papules, smooth rather than rough, often on the face and dorsa of hands, frequently in linear (Koebner) arrangement.
- Filiform wart: a slender, finger-like or thread-like projection, usually solitary or few, around the mouth, nose or eyelids; easily recognised by its frond-like shape.