Page 13 of 22
DR8.4 | Viral Wart Recognition — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Differential Diagnosis of Warts: Plantar Wart vs Corn, Molluscum Contagiosum, and Seborrhoeic Keratosis
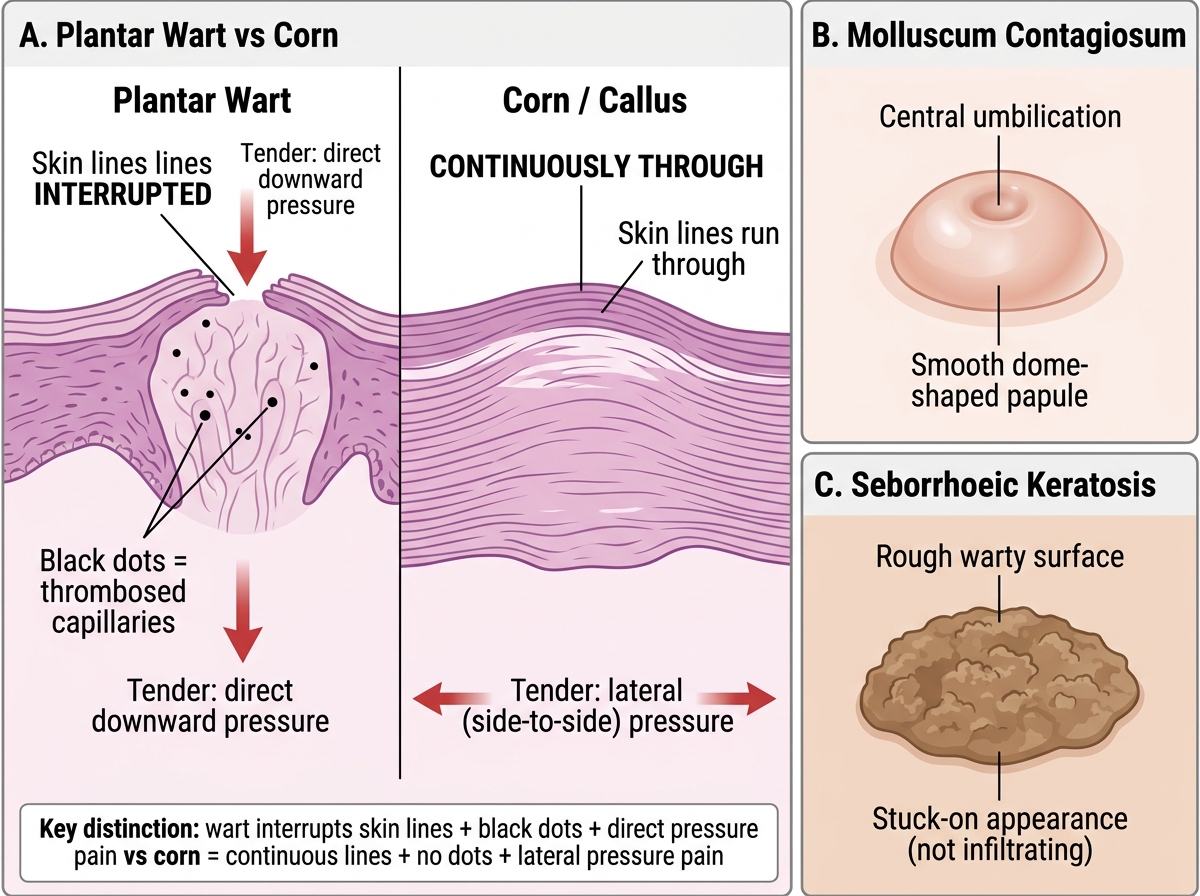
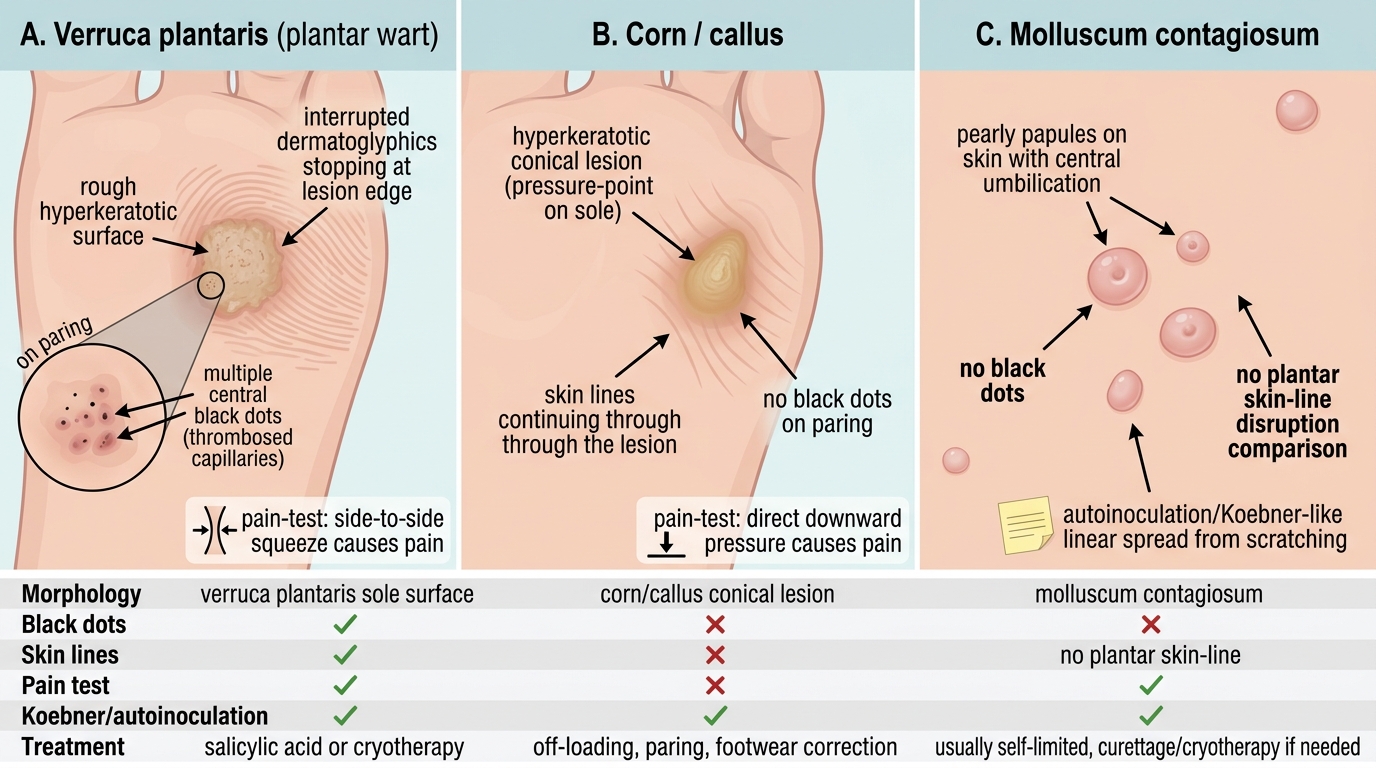
The differential diagnosis of a wart is usually settled at the bedside, and the single most important distinction in everyday practice is the plantar wart versus the corn (callus), because the two are managed quite differently and are easily confused. A corn is a focal area of protective hyperkeratosis over a pressure point: when pared, the skin lines run through it uninterrupted, there are no black dots, and it is tender on side-to-side (lateral) pressure rather than on direct downward pressure. A plantar wart, by contrast, interrupts the skin lines, shows central black dots, and hurts on direct pressure. The other key differential is molluscum contagiosum, which is a smooth, dome-shaped papule with a central umbilication, quite unlike the rough, black-dotted wart; seborrhoeic keratosis (stuck-on, warty plaques in older patients) and, rarely, amelanotic melanoma also enter the differential for an atypical lesion. Warts are a clinical diagnosis; dermoscopy and biopsy are reserved for genuinely uncertain or atypical lesions.
The differential and investigation points are:
- Corn/callus: skin lines run THROUGH the lesion, no black dots, tender on lateral pressure (vs wart: interrupted skin lines, black dots, tender on direct pressure).
- Molluscum contagiosum: smooth, umbilicated, dome-shaped papule (vs rough, black-dotted, verrucous wart).
- Seborrhoeic keratosis: stuck-on warty plaque in older adults; amelanotic melanoma: rare but must be excluded in atypical/persistent lesions.
- Investigations: clinical diagnosis is usually sufficient; dermoscopy (dotted/thrombosed vessels) and biopsy (koilocytes) only for atypical or diagnostically uncertain lesions.
Plantar Wart vs Corn vs Molluscum Contagiosum
SELF-CHECK
A patient has a painful hyperkeratotic lesion on the sole. Which finding most strongly indicates a plantar wart rather than a corn?
A. The skin lines (dermatoglyphics) run uninterrupted through the lesion
B. Paring reveals central black dots and the skin lines stop at the lesion's edge; pain is worst on direct downward pressure
C. The lesion is tender on side-to-side (lateral) pressure and has no black dots
D. The lesion is a smooth dome-shaped papule with a central dimple
Reveal Answer
Answer: B. Paring reveals central black dots and the skin lines stop at the lesion's edge; pain is worst on direct downward pressure
A plantar wart interrupts the skin lines (they stop at its margin rather than running through it), reveals central black dots (thrombosed capillaries) on paring, and is painful on direct downward pressure. A corn, by contrast, has skin lines running through it, no black dots, and is tender on lateral (side-to-side) pressure. A smooth dome-shaped papule with a central dimple describes molluscum contagiosum, not a wart. This bedside distinction matters because corns and plantar warts are managed differently, and confusing them leads to ineffective treatment and persistent pain.
Management of Viral Warts
Management of Viral Warts
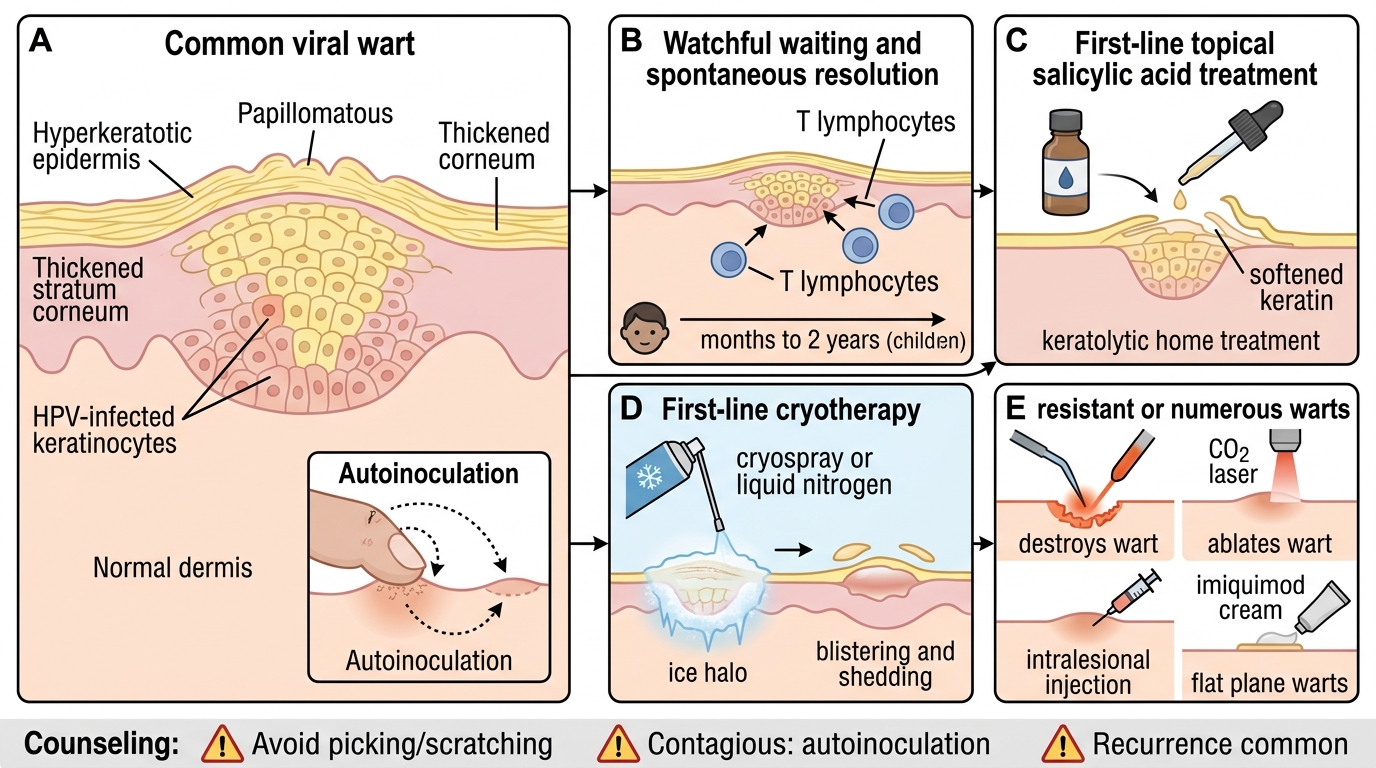
Management of viral warts is built on two facts: there is no systemic antiviral that cures HPV, and many warts resolve spontaneously over months to a couple of years as cell-mediated immunity develops, so watchful waiting is a legitimate option, especially in children. When treatment is chosen, it is essentially destructive or keratolytic — removing or destroying the infected epidermis and provoking an immune response — and the choice depends on the wart type, site, size and the patient's preference. First-line measures are topical salicylic acid (a keratolytic suitable for home use) and cryotherapy with liquid nitrogen; more resistant or numerous warts may need electrocautery, laser, intralesional agents or immunomodulators. Throughout, counsel patients that warts are contagious and spread by autoinoculation, so picking and scratching should be avoided, and that recurrence is common because treatment removes the lesion but does not eradicate the virus from surrounding skin.
The management principles are:
- Watchful waiting is reasonable — many warts self-resolve as immunity develops (particularly in children); there is no systemic antiviral for HPV.
- First-line: topical salicylic acid (keratolytic, home use) and cryotherapy (liquid nitrogen).
- Second-line / resistant or numerous warts: electrocautery, CO2 laser, intralesional bleomycin; imiquimod (immunomodulator) is useful for plane warts.
- Counsel: avoid picking/scratching (prevents autoinoculation/Koebner spread); warts are contagious; recurrence is common as treatment does not eradicate surrounding viral infection. Routine treatment of contacts is not required.
Self-Assessment: Viral Wart Recognition
Viral Wart Recognition: Classification and Key Differentials
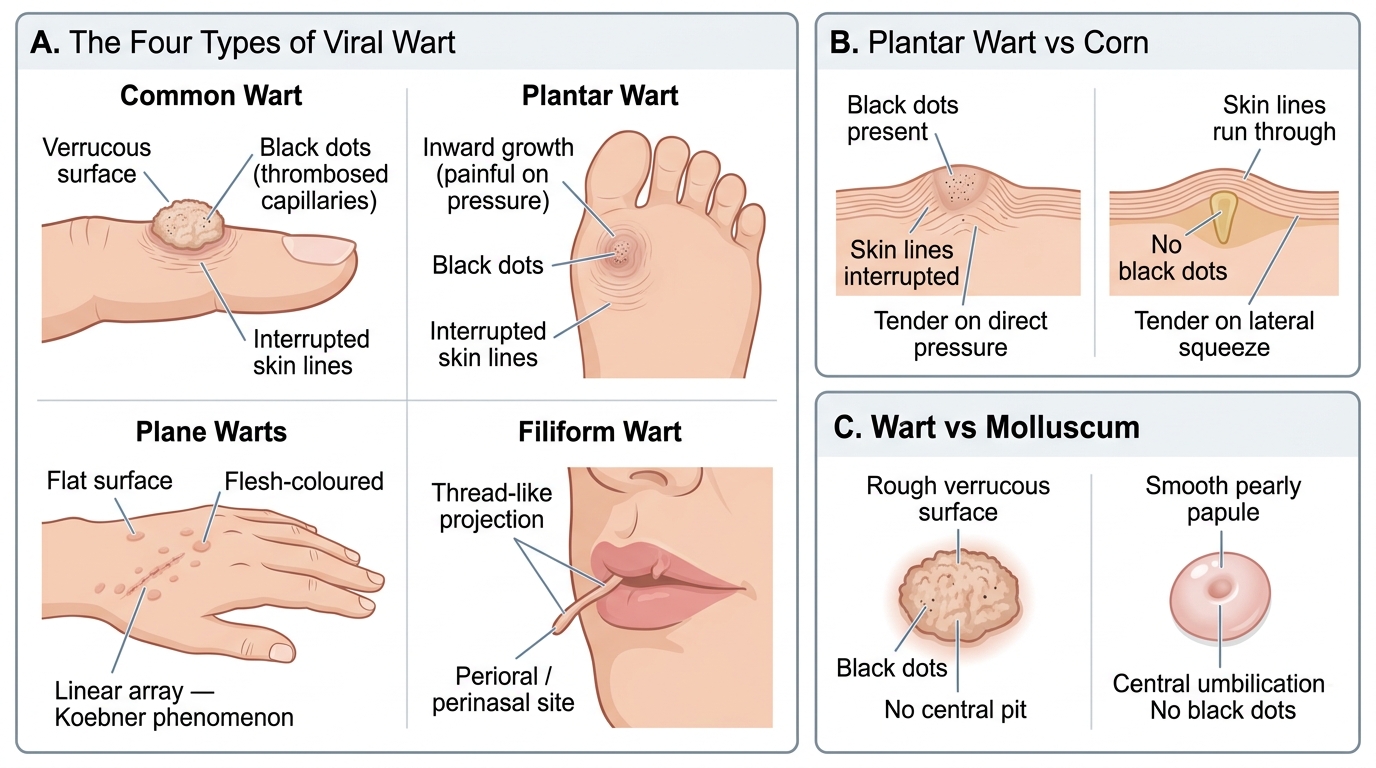
The aim of this closing section is to confirm that you can recognise a viral wart, assign it to one of the four types, and separate it cleanly from a corn and from molluscum. Recognition is an ordered reading: identify the hyperkeratotic, verrucous lesion with interrupted skin lines and black dots; place it by site and surface into common, plantar, plane or filiform; then run the key differentials — corn versus plantar wart, and wart versus molluscum — before choosing destruction, keratolysis or watchful waiting. The scenarios you should be able to handle include the rough black-dotted wart on a finger, the painful inward-growing lesion on a sole that must be told from a corn, the rows of flat plane warts following a scratch, and the thread-like filiform wart near the lip. Use the self-check below to rehearse moving from clinical appearance to type to management.
For each scenario, ask in order:
- Is the lesion hyperkeratotic and verrucous, with interrupted skin lines and black dots (a wart)?
- Which of the four types is it, by site and surface?
- Is the key differential a corn (skin lines run through, no black dots, lateral tenderness) or molluscum (smooth, umbilicated)?
- Is destruction/keratolysis indicated, or is watchful waiting appropriate, and what counselling does the patient need?
SELF-CHECK
Which statement about the management of viral warts is correct?
A. Oral aciclovir is the first-line treatment because warts are caused by a herpesvirus
B. There is no systemic antiviral for HPV; many warts self-resolve, and treatment when chosen is destructive/keratolytic (e.g. salicylic acid, cryotherapy)
C. All warts must be surgically excised to prevent malignant transformation
D. Treatment of all household contacts with antivirals is mandatory
Reveal Answer
Answer: B. There is no systemic antiviral for HPV; many warts self-resolve, and treatment when chosen is destructive/keratolytic (e.g. salicylic acid, cryotherapy)
Warts are caused by HPV, for which there is no systemic antiviral, so aciclovir (a herpesvirus drug) is not used. Many warts resolve spontaneously as cell-mediated immunity develops, making watchful waiting reasonable, especially in children. When treatment is chosen it is destructive or keratolytic — first-line options are topical salicylic acid and cryotherapy, with electrocautery, laser, intralesional agents or imiquimod for resistant or numerous warts. Routine surgical excision is not required and warts are benign, and treating all contacts with antivirals is neither indicated nor effective.
CLINICAL PEARL
Pare the lesion: a plantar wart interrupts the skin lines and reveals central black dots (thrombosed capillaries) and hurts on direct pressure, whereas a corn lets the skin lines run through, has no black dots, and hurts on lateral pressure. This single bedside manoeuvre resolves the commonest diagnostic confusion in wart management. Remember there is no systemic antiviral for HPV — treatment is destructive or keratolytic, and watchful waiting is legitimate because many warts clear as immunity develops, especially in children. Counsel patients not to pick or scratch, because autoinoculation seeds new warts along trauma lines (the Koebner phenomenon), and warn that recurrence is common since treatment removes the lesion but not the virus in the surrounding skin.