Page 5 of 18
FM2.{16,25},FM14.6 | Conducting & Reporting the Medico-legal Autopsy — SDL Guide (Part 2)
Post-mortem Artefacts: Recognition and Distinction from Injuries
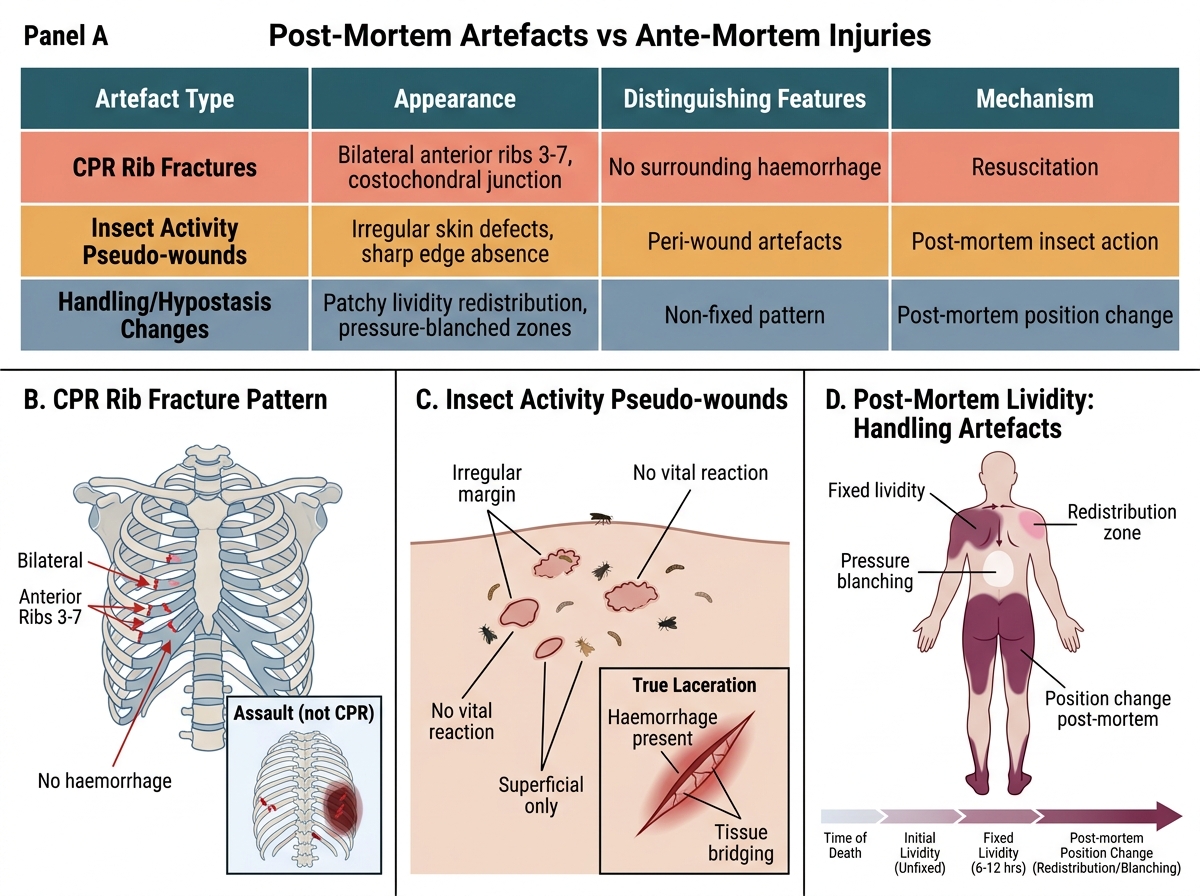
Post-mortem artefacts are changes in the body that occur after death — due to resuscitation attempts, handling, transport, insect activity, or decomposition — that can mimic or obscure ante-mortem injuries. Failure to recognise artefacts is one of the most consequential errors in forensic pathology: misattributing a CPR fracture to a homicidal assault, or failing to recognise insect pseudo-wounds as post-mortem, can change the manner-of-death determination and alter the course of criminal proceedings.
Resuscitation artefacts are the most practically important category for practising clinicians because they are created by healthcare providers:
- Anterior rib fractures (typically ribs 3–7 bilaterally, near the costochondral junction) from external cardiac compression during CPR — these are stereo-typically anterior and bilateral, unlike assault rib fractures which are often unilateral and posterior
- Sternal fractures from CPR — typically transverse, mid-sternum
- Laryngeal and tracheal contusions and mucosal lacerations from endotracheal intubation
- Needle marks and subcutaneous bruising from IV access, arterial lines, or emergency injections
- Defibrillation burns — small, well-defined, oval marks on the chest corresponding to electrode pad positions
- Gastric distension and aspiration from bag-mask ventilation
The key to differentiating resuscitation artefacts from ante-mortem injuries is the clinical history and the pattern: bilateral anterior rib fractures in a known resuscitation case are almost certainly artefactual; isolated posterior rib fractures in a person who was never resuscitated require injury explanation.
Insect activity artefacts occur primarily at natural orifices — mouth, nose, eyes, anus, genitalia — where blowfly larvae (maggots) create tissue defects that can resemble lacerations or excoriations. In advanced decomposition, these may be extensive. The forensic physician must distinguish the irregular, shallow, progressive defects of insect activity from the directed, patterned defects of ante-mortem injury.
Handling and transport artefacts include: skin pressure marks from body bags or transport surfaces (mimicking ligature marks); postural lividity changes if the body was moved before livor fixation; and abrasions from body movement across surfaces.
Decomposition artefacts include: blebs and blistering (mimicking burns or ante-mortem contusions); skin slippage (making precise injury measurement impossible); green discolouration masking bruises; and bloating that distorts facial and body landmarks.
The documentation strategy: when artefacts are present, record them specifically, explain their probable cause, and distinguish them explicitly from the findings attributed to ante-mortem events in your opinion section.
Post-Mortem Artefacts vs Ante-Mortem Injuries: Recognition and Differentiation
SELF-CHECK
At autopsy of a man who collapsed at home and was resuscitated by paramedics, you find bilateral anterior rib fractures at ribs 4–6, consistent with the costal arch. The MOST LIKELY explanation is:
A. Homicidal assault with a blunt object
B. Resuscitation artefact from external cardiac compression
C. Pathological fractures from underlying bone disease
D. Deceleration injury from a fall
Reveal Answer
Answer: B. Resuscitation artefact from external cardiac compression
Bilateral anterior rib fractures at ribs 3–7, particularly near the costochondral junction, are the classic pattern of CPR-related resuscitation artefacts. The history of paramedic resuscitation, combined with the bilateral anterior location, makes this the correct interpretation. Assault fractures are typically unilateral, posterior, and associated with surrounding soft-tissue injury patterns.
Applied Practice: Writing the PM Report and Opinion
The post-mortem report is the primary output of the medico-legal autopsy and the document on which criminal and civil proceedings depend. Competency FM14.6 requires you to prepare PM reports for at least 15 cases of varied aetiology in supervised or simulated practice. Understanding the structure of the report and the standards for the opinion section is therefore a core competency, not an adjunct.
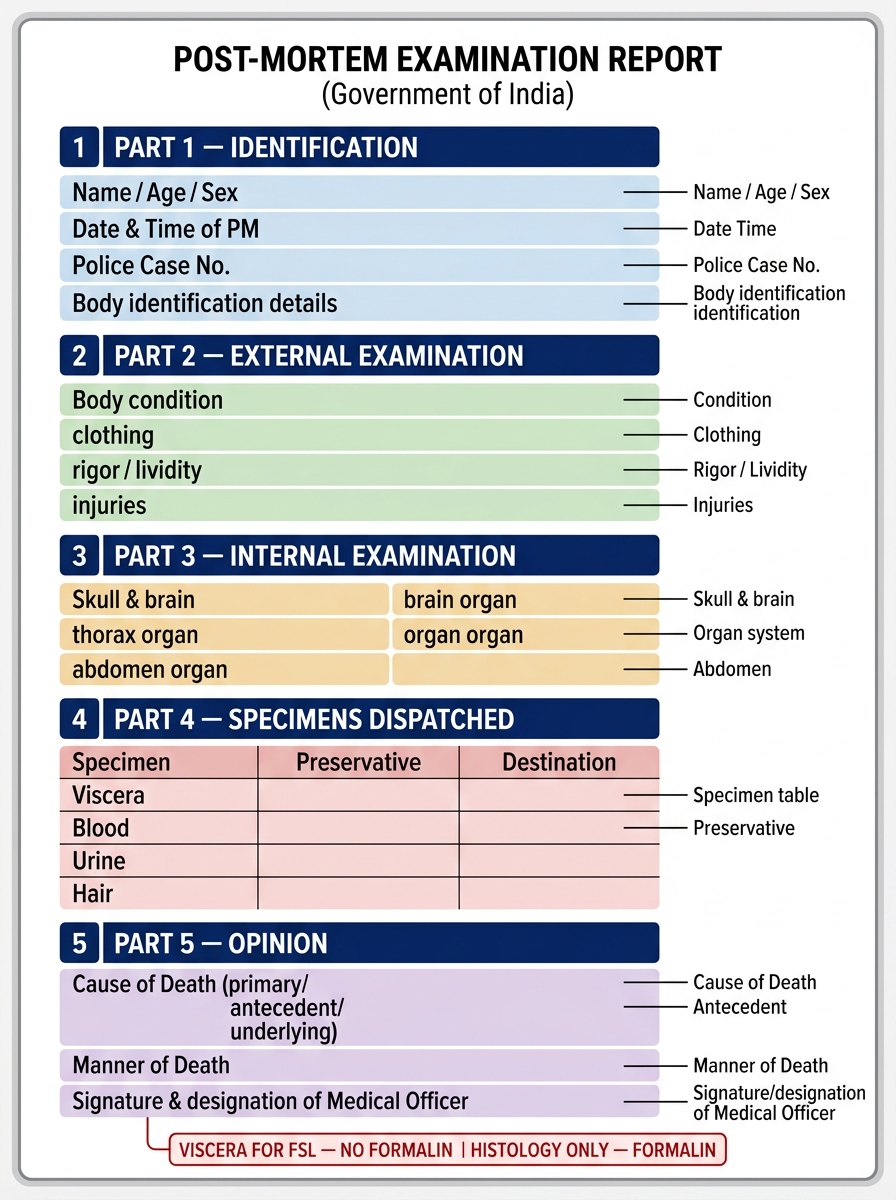
The standard government PM report form in India has the following structure:
Part 1 — Identification details: case number, date, time, authority (CRPC provision and form number), identity of deceased, referring officer details.
Part 2 — External examination findings: post-mortem changes (state and time estimate), build, identifying features, clothing, injuries (each numbered, described with location/size/type/direction/age).
Part 3 — Internal examination findings: each body cavity in sequence; organ descriptions; fluid collections; specific pathological findings.
Part 4 — Specimens preserved and dispatched: complete list of all specimens, preservatives, containers, FSL forwarding number.
Part 5 — Opinion: the forensic physician's professional conclusions, structured as:
- (a) Cause of death — in ICD three-part format: immediate cause, antecedent cause, underlying cause
- (b) Manner of death — natural/accidental/homicidal/suicidal/undetermined, with referenced findings
- (c) Mechanism of death — the physiological pathway
- (d) Other conclusions — PMI estimate, presence of ante-mortem injuries, identity of wounds
- (e) Provisional vs final opinion — where FSL results are awaited, the opinion must be clearly marked 'provisional pending toxicology'
The opinion section demands absolute discipline. Two rules must never be broken: (1) every conclusion in the opinion must be referenced to specific numbered findings in the observations section — 'homicide based on findings 3, 7, and 12'; (2) the physician must distinguish between what is directly observed ('incised wound measuring 4 cm × 2 cm over the left temporal region') and what is inferred ('consistent with a sharp-edged weapon'). The word 'consistent with' is the appropriate hedge — not 'caused by' (which implies certainty the examination cannot provide) and not 'probably from' (which is imprecise).
For FM14.6's simulated environment, practice writing reports for: drowning, hanging, firearm injuries, blunt force trauma, sharp force trauma, and poisoning cases — the core repertoire of medico-legal autopsy aetiologies.
Structure of the Standard Indian Government Post-Mortem Report Form (Five Parts)
CLINICAL PEARL
Pearl: Never put formalin in viscera destined for the FSL. This is the single most common specimen-handling error in Indian forensic practice. Formalin (10% formaldehyde) cross-links proteins and destroys volatile and non-volatile toxic substances, rendering toxicological analysis invalid. Viscera for chemical/toxicological examination must go into clean, dry glass jars with no preservative — or with sodium fluoride for blood/urine. Histology specimens (for tissue diagnosis) go separately in formalin. If you mix them up, you have both destroyed the toxicology and contaminated the histology with blood or organ fluids. Always label clearly: 'FOR FSL — NO FORMALIN' and 'FOR HISTOLOGY — FORMALIN' on the respective jars.
SELF-CHECK
Which of the following is the correct preservative for blood specimens collected at autopsy for toxicological analysis?
A. 10% formalin
B. Sodium fluoride
C. 70% ethanol
D. Saturated salt solution
Reveal Answer
Answer: B. Sodium fluoride
Sodium fluoride is the correct preservative for blood collected for toxicological analysis. It acts as both an anticoagulant and a metabolic inhibitor (preventing post-collection glucose fermentation to alcohol — important in blood alcohol analysis). Formalin destroys toxic substances; ethanol interferes with alcohol analysis; saturated salt solution is not used for blood preservation in forensic toxicology.