Page 6 of 14
FM2.1-2,FM14.5 | Cause-of-Death Certification: MCCD & ICD-11 — SDL Guide
Learning Objectives
- Describe the legal framework governing death certification in India and identify who is authorised to complete the MCCD
- Complete the MCCD Form 4A correctly, including the Part I causal chain (Ia/Ib/Ic) and Part II contributory conditions
- Select the appropriate underlying cause of death per MCCD/ICD-11 principles and apply ICD-11 codes
- Demonstrate MCCD completion in simulated clinical scenarios, including common error avoidance
- Identify deaths that cannot be certified on the MCCD and describe the correct referral pathway
INSTRUCTIONS
Every doctor will, at some point in their career, be required to complete a Medical Certificate of Cause of Death (MCCD). This document is not just a formality — it is a legal instrument, a public health record, and the basis for cause-of-death statistics that drive national health policy. An incorrect MCCD can conceal a homicide, delay insurance claims, create legal liability for the certifying doctor, and corrupt vital statistics data. This module teaches the structure, logic, and practical completion of the MCCD, and shows how to apply ICD-11 coding to the certified underlying cause of death.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old man with known type 2 diabetes mellitus and hypertension is admitted with pneumonia and dies on day 3 of hospitalisation. The treating junior resident is asked to complete the MCCD before the ward round. She stares at the form, uncertain: should she write 'cardiorespiratory arrest' in the immediate cause box? Is the diabetes a Part I or Part II condition? Should hypertension go anywhere on the certificate? And what exactly is the 'underlying cause'? She is not alone — MCCD errors are among the most common documentation failures in Indian hospitals, and they have real consequences beyond the administrative. Let us work through the logic systematically.
WHY THIS MATTERS
The MCCD is simultaneously a legal document, a clinical record, and a public health instrument. As a legal document, it is required for registration of the death under the Registration of Births and Deaths Act 1969 and for obtaining a burial/cremation permit. As a clinical record, it is prima facie evidence of the cause of death and may be used in insurance claims, pension applications, and estate proceedings. As a public health instrument, the underlying cause of death data aggregated from millions of MCCDs drives WHO Global Burden of Disease statistics and the National Health Mission's disease burden estimates. A doctor who writes 'cardiac arrest' as the cause of death on every certificate without specifying the underlying cause contributes to cause-of-death statistics that are meaningless. A doctor who certifies a homicide as a natural death may inadvertently obstruct justice. ICD-11 coding ensures that the underlying cause identified on the MCCD is translated into a globally comparable, computerised record.
RECALL
Recall from fp2: the distinction between natural and unnatural death determines whether the MCCD can be issued at all — only natural deaths (and unnatural deaths after forensic autopsy and case closure) are certifiable on the MCCD. Recall from fp1: the concept of the immediate cause of death (the final mechanism, e.g. cardiorespiratory failure) versus the underlying disease (the original condition that started the fatal chain). Recall from fp3: post-mortem changes help confirm death has occurred and can guide the attending physician in estimating when death occurred, which is recorded on the MCCD. And from Year 1 pathology: the difference between a direct complication (Part I) and an associated condition (Part II) — for example, hyponatraemia caused by the tumour goes in Part I if it caused death; hypertension present as a comorbidity but not directly causing death goes in Part II.
Legal and Professional Context of MCCD
The Medical Certificate of Cause of Death (MCCD) in India is issued on Form 4A under the Registration of Births and Deaths Act 1969 (RBD Act). This Act makes it mandatory to register every death with the local registrar within the prescribed period. The MCCD is the primary document used for this registration and is the legal basis for death registration.
Who can issue the MCCD? The certifying physician must be a registered medical practitioner who:
- Was in attendance on the deceased during the last illness, OR
- Examined the body after death
The certifying doctor must have personal knowledge of the case — a doctor who was never involved in the care of the patient cannot sign the certificate, even if they are the most senior doctor in the hospital. In cases where the patient was treated by multiple specialists, the primary treating doctor (or their nominated representative from the team) signs. The doctor signs a declaration on the form stating that they certify, to the best of their knowledge and belief, the cause of death as stated.
When MCCD cannot be issued by the attending physician:
- Deaths within 24 hours of admission where the cause is not known
- Deaths under suspicious or unnatural circumstances
- Deaths in medico-legal cases (road traffic accidents, industrial accidents, alleged poisoning, etc.)
- Maternal deaths
- Deaths in police or judicial custody
In these cases, the body must be referred to the police or magistrate; an inquest may be held; and a forensic autopsy is performed. Only after the forensic process establishes the cause of death can the MCCD (or equivalent forensic certificate) be completed.
Legal weight and consequences of an incorrect MCCD:
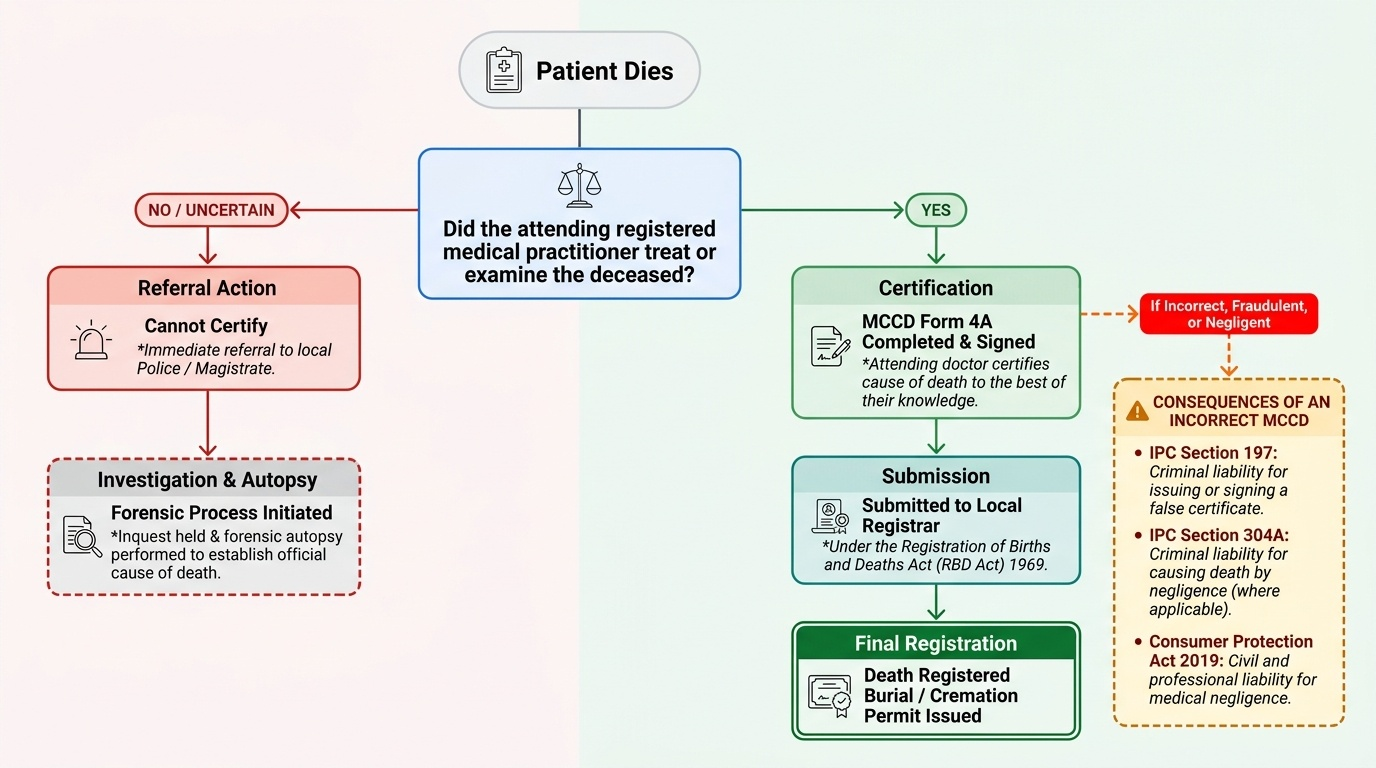
Provided image
- A negligently or fraudulently completed MCCD exposes the doctor to IPC 304A (negligence causing death if the error was due to negligence), IPC 197 (issuing a false certificate), and potential action under the Consumer Protection Act 2019
- Insurance companies and courts challenge MCCDs that are incomplete, internally inconsistent, or inconsistent with known clinical facts
- From a public health perspective, MCCD data are used by the Registrar General of India and WHO; systematically incorrect certification corrupts national cause-of-death statistics
MCCD Structure: Part I Causal Chain and Part II Contributory Conditions
The MCCD form follows the internationally standardised WHO certificate of cause of death structure, adapted for India as Form 4A. Understanding the internal logic of the form is the foundation for completing it correctly.
Part I — The Direct Cause-of-Death Chain
Part I contains three rows (Ia, Ib, Ic), each asking for a cause of death in a specific position in the causal chain:
- Row Ia: Immediate (direct) cause of death — the final disease or complication that directly caused death. This is what the body did in its last hours: respiratory failure, acute myocardial infarction, septic shock, acute renal failure. Note: 'cardiac arrest' or 'cardiorespiratory arrest' should NOT be written here — these are the mechanism of death (a mode), not a disease. They add no diagnostic information (every person who dies has a cardiac arrest). Instead, write the disease that caused the cardiac arrest.
- Row Ib: Antecedent (intermediate) cause — the disease or condition that led to Ia; i.e. due to which disease did the person develop the Ia condition? For example: 'Ia: respiratory failure — due to — Ib: bacterial pneumonia'
- Row Ic: Underlying cause — the original disease or condition that started the entire chain of events, and that is present in the Ib row as a complication. This is the most important row for public health coding. For example: 'Ia: respiratory failure — due to — Ib: bacterial pneumonia — due to — Ic: bronchogenic carcinoma'. The bronchogenic carcinoma is the underlying cause — the first link in the fatal chain. If there is no intermediate step (the underlying cause directly caused death without an intermediate step), Ib is left blank and Ic contains the underlying cause.
The key rule: The UNDERLYING CAUSE (Row Ic, or Row Ib if Ic is blank, or Row Ia if only one cause) is the cause that is entered into ICD-11 for coding and public health statistics.Part II — Contributing Conditions Part II is for significant conditions that were present at the time of death and may have contributed to the death but did NOT form part of the direct causal chain in Part I. Examples: - Diabetes mellitus (in a patient who died from coronary artery disease: diabetes is a risk factor and contributed, but the direct chain is MI → cardiac arrest; diabetes goes in Part II) - Hypertension (similarly — a contributing risk factor for the coronary disease, but not in the direct chain) - Immunosuppression from HIV in a patient who died from tuberculosis (tuberculosis is Part I; HIV goes in Part II as a contributing condition)Common Part I errors:- Writing symptoms (dyspnoea, chest pain) or terminal events (cardiac arrest) as causes - Leaving Ic blank when there IS an underlying condition - Reversing the chain (writing the underlying cause in Ia and the immediate cause in Ic) - Putting the same condition in both Part I and Part II IMAGE_NEEDED: annotated diagram of the Indian MCCD Form 4A showing Part I (three rows Ia immediate cause, Ib antecedent cause, Ic underlying cause with arrows showing the causal chain direction) and Part II (contributory conditions), with a worked example filled in for a patient dying from pneumonia due to bronchogenic carcinoma with COPD as a contributory condition | MCCD Section | Row | Content | ICD coding target? | |---|---|---|---| |Part I| Ia | Immediate (final) cause | No | |Part I| Ib | Intermediate cause ('due to Ia') | No | |Part I| Ic | Underlying cause ('due to Ib') |Yes| |Part II | — | Contributing conditions (not in causal chain) | No |
SELF-CHECK
A 55-year-old diabetic woman dies from acute renal failure caused by diabetic nephropathy. She also had hypertension which likely contributed to the progression of her renal disease. How should the MCCD be completed?
A. Part I Ia: Acute renal failure; Part I Ib: blank; Part I Ic: blank; Part II: blank
B. Part I Ia: Cardiac arrest; Part I Ib: Acute renal failure; Part I Ic: Diabetic nephropathy; Part II: Diabetes mellitus, hypertension
C. Part I Ia: Acute renal failure; Part I Ib: Diabetic nephropathy; Part I Ic: Diabetes mellitus; Part II: Hypertension
D. Part I Ia: Diabetic nephropathy; Part I Ib: Acute renal failure; Part I Ic: Diabetes mellitus; Part II: Hypertension
Reveal Answer
Answer: C. Part I Ia: Acute renal failure; Part I Ib: Diabetic nephropathy; Part I Ic: Diabetes mellitus; Part II: Hypertension
The correct causal chain is: Ia (immediate/final cause) = acute renal failure → Ib (intermediate cause that led to Ia) = diabetic nephropathy → Ic (underlying/original cause) = diabetes mellitus. Hypertension contributed to disease progression but was not in the direct causal chain, so it belongs in Part II as a contributing condition. The chain flows from immediate (Ia) back to underlying (Ic), not the other way around. Option A is incomplete — there IS a known underlying cause that should be stated. Option B incorrectly puts 'cardiac arrest' in Ia (which is a mode, not a disease) and puts diabetes in Part II when it IS the underlying cause. Option D reverses the causal chain direction.
ICD-11 Coding: Applying the Classification to Cause of Death
The International Classification of Diseases, 11th Revision (ICD-11) is the global standard for health data, clinical records, and cause-of-death statistics, published by the World Health Organisation (WHO). The 11th revision was adopted by the World Health Assembly in 2019 and came into effect on 1 January 2022, replacing ICD-10. India is transitioning to ICD-11 coding; for mortality certification purposes, the underlying cause of death in MCCD Part I is the entity that is assigned an ICD-11 code.
The ICD-11 coding system uses an alphanumeric code structure: each disease or condition has a unique code consisting of letters and numbers (e.g. 'BA80.0 Atherosclerotic coronary artery disease'; 'CA20 Type 2 diabetes mellitus'). The full classification is available at icd.who.int via the WHO ICD-11 browser, which includes a search function allowing coding by disease name, synonym, or clinical term. The mortality coding guidelines specify rules for selecting the underlying cause of death when the MCCD provides a chain, and for handling common certification errors.
Why the underlying cause is what gets coded (not the immediate cause):
The underlying cause of death — the original disease that started the fatal chain — is the single most important piece of public health information. It tells us: what disease killed this person? If we coded the immediate cause (e.g. 'respiratory failure'), we would know only the final mechanism, not the original disease — and all respiratory deaths would be attributed to 'respiratory failure' regardless of whether they came from pneumonia, lung cancer, pulmonary embolism, or drowning. Coding the underlying cause is what makes cause-of-death statistics meaningful for disease prevention and health policy.
Applying ICD-11 in three steps:
1. Identify the underlying cause of death from the completed MCCD (Row Ic, or Row Ia if no chain exists)
2. Search the ICD-11 browser at icd.who.int using the name of the underlying condition (e.g. 'ischaemic heart disease', 'pulmonary tuberculosis', 'breast cancer')
3. Select the most specific code that matches the clinical diagnosis — ICD-11 codes go from broad to specific (e.g. BA80 = ischaemic heart disease → BA80.0 = atherosclerotic coronary artery disease → BA80.00 = stable angina within it)
Key ICD-11 coding scenarios for FM/clinical practice:
- Tuberculosis: DA90 (pulmonary) — distinguish pulmonary from extrapulmonary; code the site
- Ischaemic heart disease: BA80 and subtypes
- Stroke: cerebral infarction (8B11), intracerebral haemorrhage (8B00), subarachnoid haemorrhage (8B01)
- Maternal deaths: special Chapter 18 codes (JA and related); maternal cause must always be coded
- Injury deaths (unnatural): external cause codes (Chapter 22-23) PLUS the nature of injury code
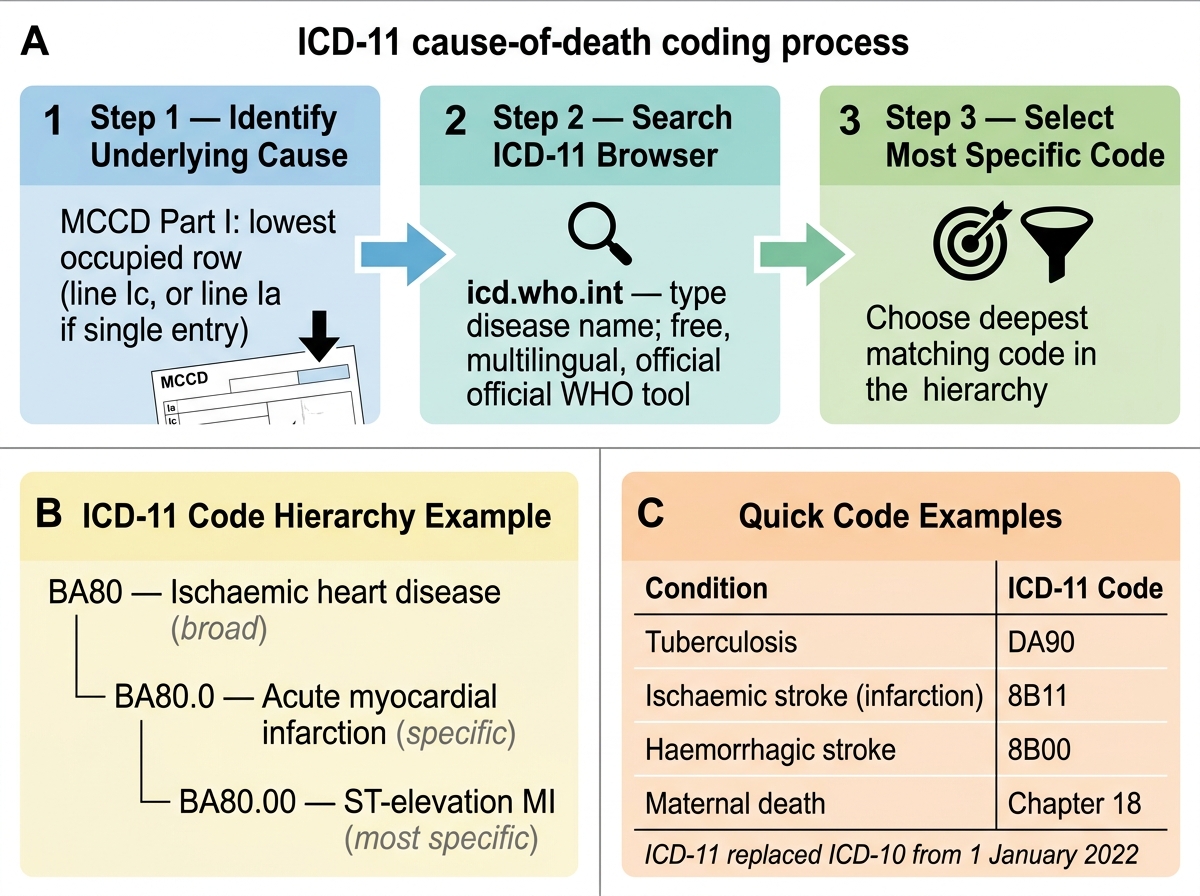
ICD-11 Coding of Underlying Cause of Death: Three-Step Process and Code Hierarchy
- ICD-11 browser: icd.who.int — free, searchable, available in multiple languages
- The underlying cause (MCCD Part I lowest populated row) is the ICD-11 coding target
- ICD-11 replaced ICD-10 effective 1 January 2022