Page 5 of 14
FM2.9-11 | Post-mortem Changes & Time Since Death — SDL Guide
Learning Objectives
- Describe the early post-mortem changes (algor mortis, post-mortem lividity, rigor mortis) with their temperature-dependent timings and forensic significance
- Distinguish cadaveric spasm, cold stiffening, and heat stiffening from true rigor mortis
- Describe the late post-mortem changes — putrefaction, adipocere, mummification, and maceration — including the conditions that favour each
- Outline the multi-method approach to estimating post-mortem interval (PMI), including body temperature, rigor staging, stomach contents, entomology, and vitreous chemistry
- Apply post-mortem change findings to medicolegal conclusions in case scenarios
INSTRUCTIONS
When the police call in a forensic physician to examine a body found at a scene, the first question is almost always: 'How long has this person been dead?' The answer — the post-mortem interval (PMI) — is derived not from a single measurement but from reading the body's own biological clock. The changes that occur after death are predictable, sequential, and modifiable by environment — making them powerful forensic tools when interpreted correctly. This module covers all the post-mortem changes that you will encounter at autopsy, scene examination, and examination in the field, and shows how to integrate them into a defensible PMI estimate.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At 06:30 on a Monday morning, police are called to a locked apartment. They find a 38-year-old woman lying face-up on the floor of her bedroom. There is no obvious injury. The investigating officer asks the attending physician: 'When did she die? Her husband says he last saw her alive on Friday evening.' The physician notes: the body is cool to touch, pupils are fixed, there is obvious purple discolouration on the back and buttocks that does not blanch with pressure, and the jaw and neck muscles are stiff but the arms and legs are flaccid. A faint sweet odour is beginning. The physician needs to integrate these findings into a coherent PMI estimate — and each finding tells a different part of the story.
WHY THIS MATTERS
Post-mortem changes are the forensic physician's most important tools in the medicolegal investigation of death. The ability to estimate the time since death narrows the window of opportunity for potential assailants, corroborates or refutes alibi evidence, and helps identify whether a body has been moved (e.g. lividity in a position inconsistent with where the body was found). The colour of post-mortem lividity can provide the first clue to the cause of death — cherry-red lividity suggests carbon monoxide poisoning even before toxicology results are available. Cadaveric spasm can preserve the grip of the hand at the moment of death, distinguishing suicide from homicide. Understanding late changes — adipocere, mummification, and putrefaction — allows PMI estimation even in bodies discovered months or years after death. These are not theoretical concepts; they are the practical tools of every forensic field examination.
RECALL
Recall from fp1: somatic death is followed by cellular death, and the body begins to lose physiological homeostasis immediately. Temperature regulation ceases; bacterial containment breaks down; muscle physiology alters irreversibly. From Year 1 biochemistry, recall ATP's role: ATP is the energy currency that drives active ion transport (Na+/K+ ATPase), myosin ATPase for muscle relaxation, and cellular membrane integrity. When cardiac output stops and oxidative phosphorylation ceases, ATP is consumed and not regenerated. This ATP depletion is the molecular basis of rigor mortis. From physiology, recall that bacteria colonise the intestines during life but are contained by immune defences and bowel wall integrity; after death these defences fail, producing the gas and tissue degradation of putrefaction. These Year 1 foundations are directly applied in interpreting every post-mortem change.
Early Post-mortem Changes: Algor Mortis, Lividity, and Rigor Mortis
The early post-mortem changes are those that occur within the first 24-48 hours of death. They are the most useful for PMI estimation in the acute forensic setting because they are more temperature-sensitive and time-dependent than the late changes.
Algor mortis (post-mortem cooling) is the gradual decrease in body temperature from the normal ~37°C to ambient temperature after death, due to cessation of metabolic heat production. The rate of cooling is approximately 1.5°C per hour in the early post-mortem period under standard conditions (exposed body, ambient ~20-22°C), but this figure is a rough guide only — the actual rate depends on: ambient temperature, body weight and habitus (obese bodies cool more slowly), clothing and coverings, air currents, and humidity. The Henssge nomogram (a widely used mathematical model) provides a more accurate PMI estimate from rectal body temperature and ambient temperature, incorporating corrective factors for body weight and covering. The forensic rule: rectal temperature measurement is the most objective single PMI tool available in the early post-mortem period (up to ~24h).
Post-mortem lividity (also called hypostasis or livor mortis) is the gravitational settling of blood into the dependent (lowest) vessels and capillaries after the circulation stops. Blood is no longer being pumped, and under gravity it pools in the lowest vessels, producing a bluish-purple (blue-red, violaceous) discolouration of the skin in the dependent parts of the body. Post-mortem lividity:
- Begins within 30 minutes to 2 hours of death as a faint blush in dependent areas
- Becomes well-established and confluent over the next several hours
- Is initially non-fixed (mobile): if the body is turned before fixation, the lividity shifts to the new dependent position
- Becomes fixed at approximately 8-12 hours after death, when the extravasated blood has clotted or been absorbed into tissues; after this point, turning the body does NOT shift the lividity
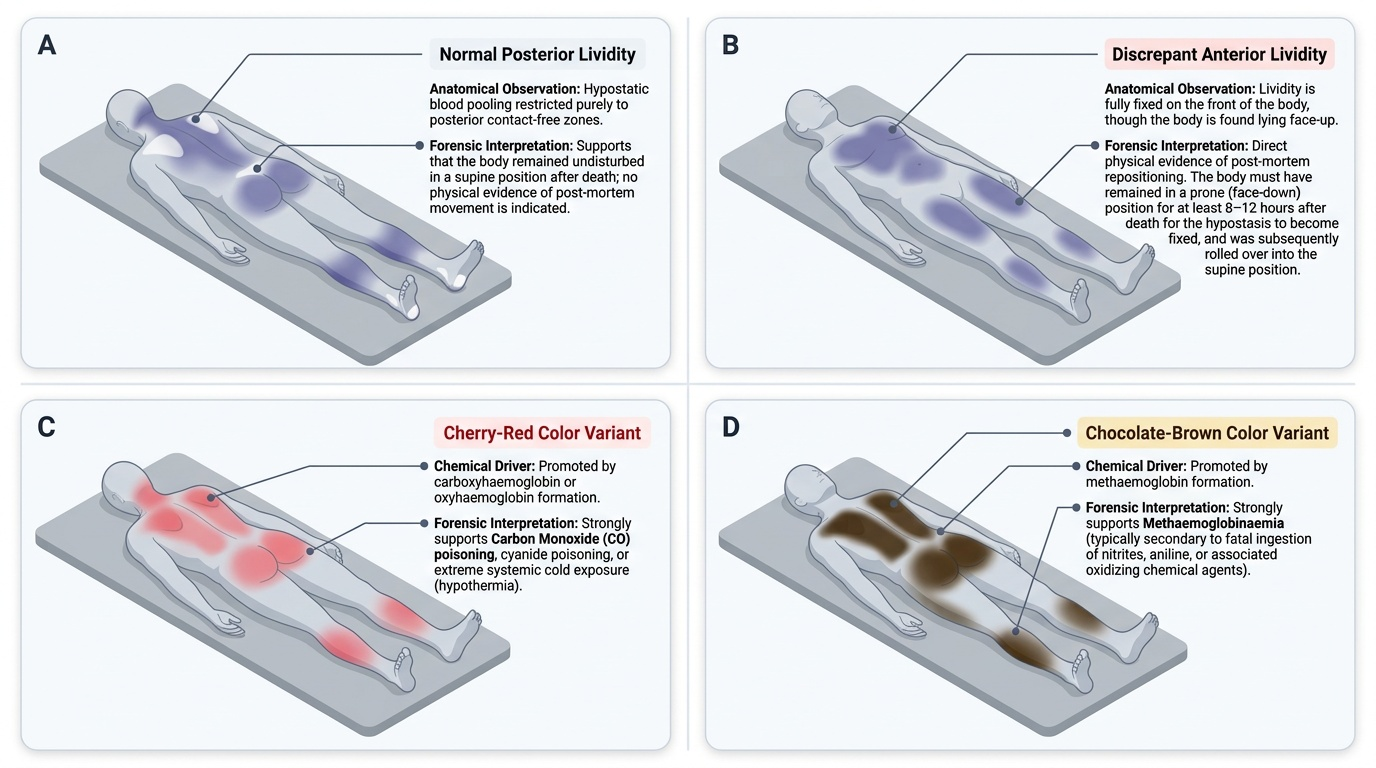
- The fixation at 8-12h is a key forensic landmark: if lividity is fixed in a position inconsistent with where the body is found (e.g. posterior lividity but body found face-down), the body has been moved after 8-12 hours
Post-mortem lividity colour is important:
- Normal (blue-purple to violaceous): usual colour of deoxygenated blood pooling
- Cherry-red or bright-red lividity: indicates carboxyhaemoglobin — the stable compound formed by carbon monoxide (CO) binding to haemoglobin; cherry-red lividity strongly suggests CO poisoning before any toxicology results are available; can also be seen in cyanide poisoning and cold environments (cold preserves oxyhaemoglobin)
- Chocolate-brown or dark-brown lividity: indicates methaemoglobinaemia — caused by agents that oxidise haemoglobin (e.g. nitrite, potassium chlorate, dapsone, phenacetin)
- Pale/absent lividity: seen in severe anaemia (minimal blood to pool)
Rigor mortis is the progressive stiffening of skeletal (and cardiac, and smooth) muscles occurring after death due to ATP depletion. After somatic death, ATP is consumed by ongoing cellular processes but not replenished; the actin-myosin cross-bridges (which normally detach during muscle relaxation, requiring ATP) become permanently locked, causing rigid stiffening. The sequence at ambient temperature of approximately 25-30°C (this temperature specification is mandatory — timings vary substantially at different temperatures):
- Onset: 1-2 hours after death — begins in small muscles of face and jaw (masseter muscles first, then neck)
- Fully established: 6-12 hours — involves all muscle groups; body is completely stiff
- Resolution: begins 24-36 hours — muscles begin to relax again as autolysis and bacterial proteolysis break down the cross-bridges
- In cold environments, rigor is delayed and prolonged; in hot environments, it develops faster and resolves sooner
- The 'rule of 12' is a teaching simplification: first 12h = establishing rigor; second 12h = fully rigid; third 12h = resolving
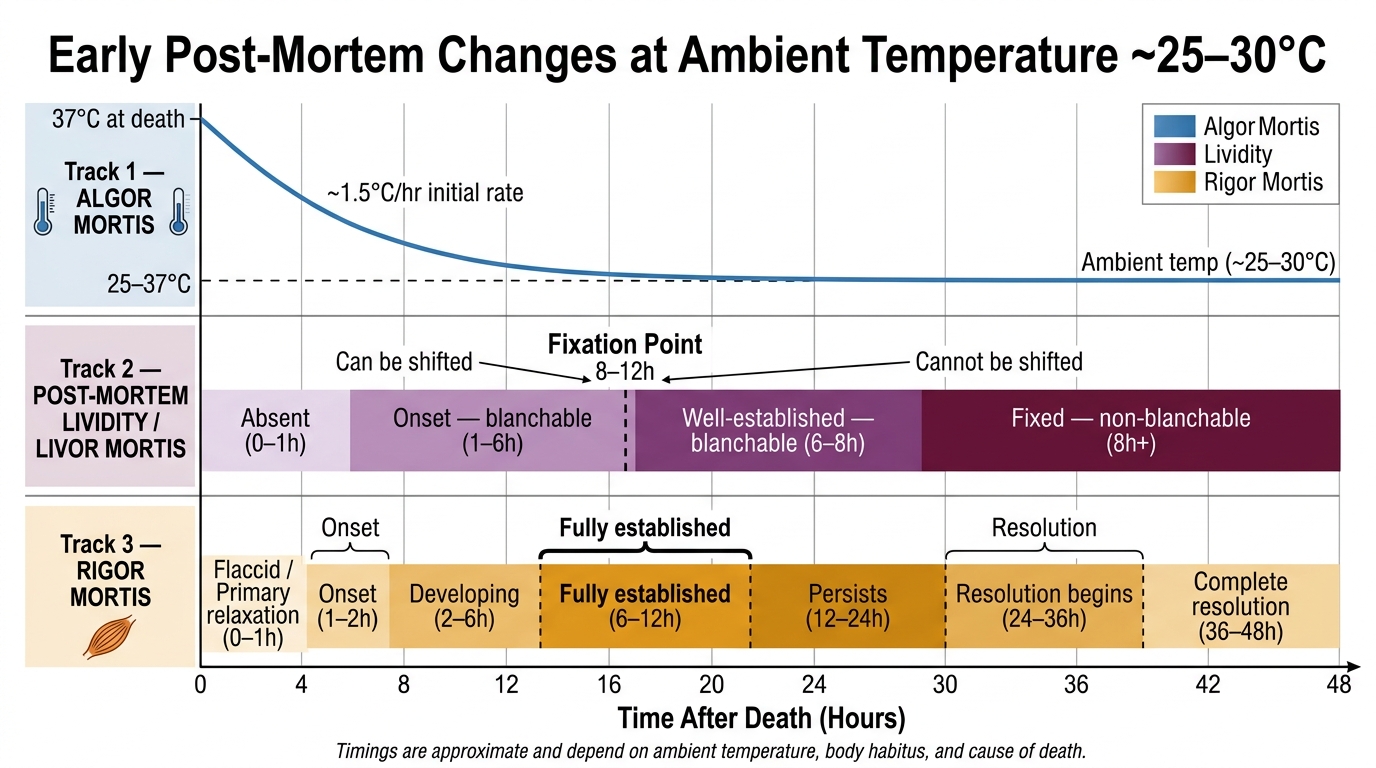
Timeline of Early Post-Mortem Changes (Ambient ~25–30°C)
Three conditions resembling but NOT being rigor mortis:
- Cadaveric spasm (instantaneous rigor, cataleptic rigidity) is the immediate, persistent muscular contraction occurring at the exact moment of death, without any preceding flaccid period. Unlike rigor mortis, cadaveric spasm does not involve ATP depletion — its mechanism involves sudden intense nervous discharge at the moment of death, creating immediate sustained contraction. It is seen in: sudden violent death, drowning (clutching drowning victim), electrocution, head wounds, extreme physical/emotional stress at death. Forensically crucial: cadaveric spasm preserves the exact posture, grip, and object held at the instant of death — a victim in cadaveric spasm clutching a knife handle in a 'suicide' death is a significant finding, since it is difficult to fabricate and indicates the person was holding the knife at the moment of dying
- Cold stiffening is rigidity of the body due to freezing of muscle fluids, fat, and joint fluids in sub-zero temperatures. It is NOT rigor mortis — it disappears completely on thawing, leaving a normal flaccid body (or normal rigor if the temperature is then suitable). A body found frozen solid in winter is in cold stiffening, not rigor.
- Heat stiffening occurs when the body is exposed to intense heat (fire, scalding). Muscle protein coagulates (like cooking an egg white), causing extreme rigid stiffening. The body often adopts the pugilistic attitude (boxer's stance) due to flexor muscle coagulation producing generalised flexion of all joints. Heat stiffening is NOT rigor mortis and does not follow the rigor mortis timeline.
SELF-CHECK
A body is found in a room maintained at 25°C. Rigor mortis is partially established in the jaw and neck but not yet present in the limbs. Lividity is present on the back and blanches with finger pressure. What is the most likely post-mortem interval?
A. Less than 1 hour
B. Approximately 2-4 hours
C. Approximately 12-18 hours
D. More than 24 hours
Reveal Answer
Answer: B. Approximately 2-4 hours
At ~25°C, rigor mortis begins at 1-2 hours and proceeds from small muscles (jaw/neck) to large muscles. Partial establishment in jaw/neck but not yet in limbs suggests early rigor, consistent with approximately 2-4 hours post-mortem. Lividity that still blanches with pressure indicates it has not yet fixed (fixation occurs at ~8-12h), supporting a PMI of less than 8-12 hours and consistent with the 2-4h estimate. Less than 1 hour would show minimal or no rigor and very faint lividity. 12-18 hours would show fully established or resolving rigor and fixed lividity. More than 24 hours would show rigor beginning to resolve and fixed lividity.
Late Post-mortem Changes: Putrefaction, Adipocere, Mummification, and Maceration
Provided image
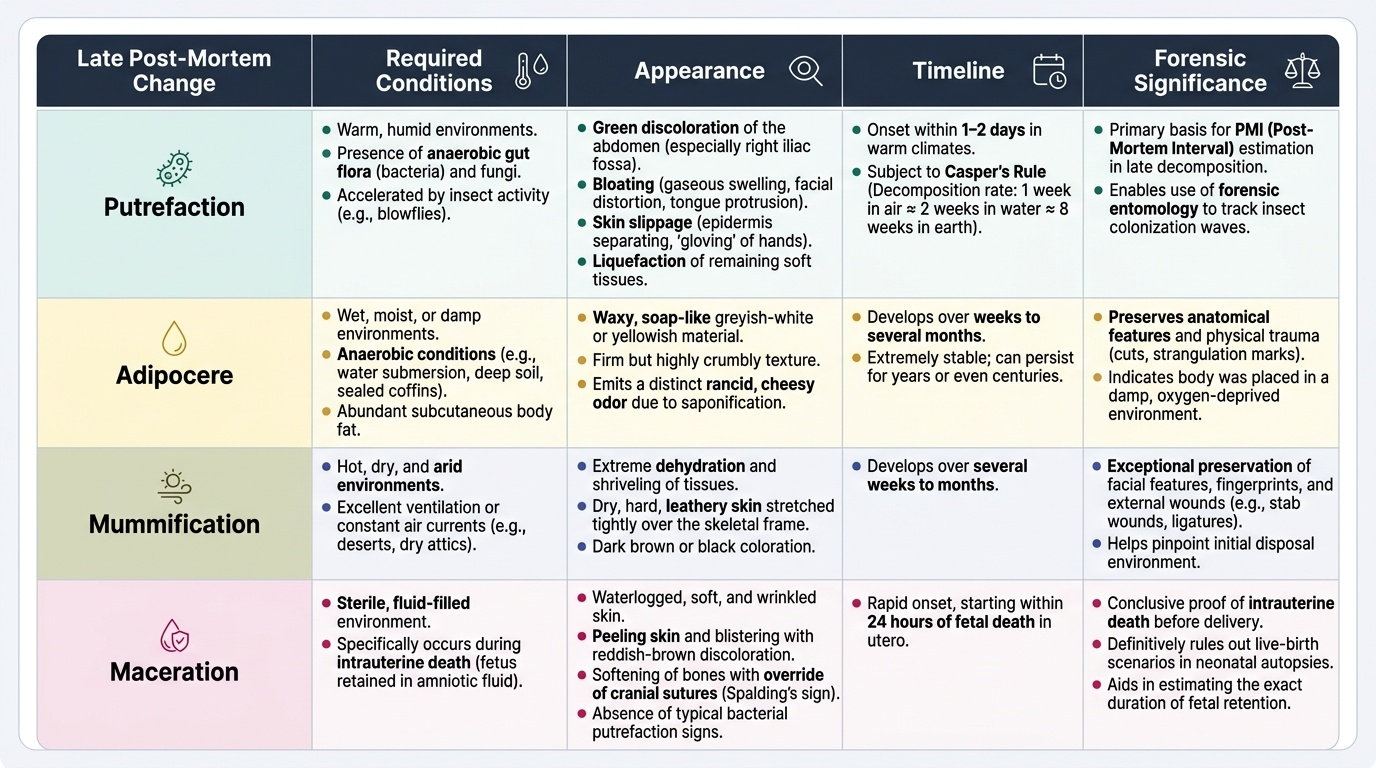
The late post-mortem changes occur days to weeks or months after death. They are most relevant for PMI estimation in cases of delayed discovery. Unlike the early changes, which are primarily physical and chemical, the late changes involve microbial activity, environmental chemistry, or intrauterine processes. Each produces a characteristic transformation of the body that has diagnostic and forensic significance.
Putrefaction is the decomposition of body tissues by the action of bacteria (primarily anaerobic gut flora that escape the intestine after bowel wall integrity is lost post-mortem) and fungi. It is the most common late post-mortem change. Putrefaction progresses through recognisable stages:
- Green discolouration of the abdomen (especially the right iliac fossa, where the caecum lies close to the surface) is typically the first visible external sign — usually apparent at 1-2 days in warm climates. The green colour is due to sulphhaemoglobin formed by bacterial hydrogen sulphide reacting with haemoglobin
- Bloating — gas accumulation in body cavities and tissues (hydrogen sulphide, methane, ammonia) causes facial distortion, protrusion of the tongue, scrotal/penile/labial swelling, and frothy blood-stained fluid from the mouth and nose
- Skin slippage — the epidermis separates from the dermis ('gloving' of the hands) and fills with blood-stained fluid (phlyctenae/blisters)
- Liquefaction — soft tissue is progressively liquefied; eventually only skeletal remains are left
The rate of putrefaction is profoundly affected by environment: warm humid conditions accelerate it dramatically (a body in tropical India begins to show putrefaction within 24-48 hours); cold, dry, or chemically hostile environments retard it. The presence of insects (especially blow flies, Calliphora and Lucilia species) dramatically accelerates soft tissue loss but also provides the basis for forensic entomology (see PMI estimation below). Casper's rule states that 1 week in the open air ≈ 2 weeks in water ≈ 8 weeks in earth — providing a rough cross-medium comparison of decomposition rates.
Adipocere (Latin: adeps = fat; cera = wax) is a waxy, soap-like transformation of body fat into a greyish-white or yellowish, firm, crumbly material with a rancid or cheesy odour. The process — saponification — involves the hydrolysis and hydrogenation of body fats (triglycerides) into saturated fatty acids, primarily ammonium salts of palmitic and stearic acids. Adipocere formation requires: warmth (optimal ~20-30°C), moisture (submerged bodies, buried in damp soil), and anaerobic conditions. It typically begins at 3-6 months and can persist for decades, preserving the general body shape. Forensic significance: (a) it helps establish identity of long-dead individuals by preserving body form; (b) it may preserve wound tracks and injuries within the fat; (c) PMI can be estimated in years if adipocere is extensive.
Mummification is the preservation of the body by desiccation — complete drying of the tissues before putrefactive organisms can destroy them. It requires: dry, warm (or arid), well-ventilated conditions. The body becomes dark brown, shrunken, leathery, hard, and odourless. Natural mummification can occur in desert environments, in well-ventilated attics or roof spaces, and in some burial sites. Mummified bodies may be centuries old. Forensically: wound patterns (especially sharp-force injuries) are sometimes preserved in mummified tissue, allowing identification of cause of death in very old cases. Mummified foetuses (foetus papyraceus in twin pregnancies) are an obstetric variant.
Maceration is the sterile autolytic softening and disintegration of tissues that occurs in a fluid environment without the action of bacteria, in either two contexts:
- Intrauterine maceration of a dead foetus: after foetal death in the womb, the foetus undergoes maceration without putrefaction (the uterus is sterile). The process begins within 12-24 hours of foetal death: the skin becomes red-brown, oedematous, and easily slips off (skin slippage); internal organs liquefy; the bones may overlap (Spalding's sign on X-ray — a classic radiological feature of intrauterine foetal death). Maceration is forensically important in medico-legal cases involving stillbirth — the degree of maceration indicates approximately how long the foetus was dead before delivery
- Maceration of a body in water: prolonged immersion causes skin wrinkling, swelling, and eventually detachment ('washerwoman's hands'); this is distinct from putrefaction (which also occurs in water) and represents physical/osmotic tissue change
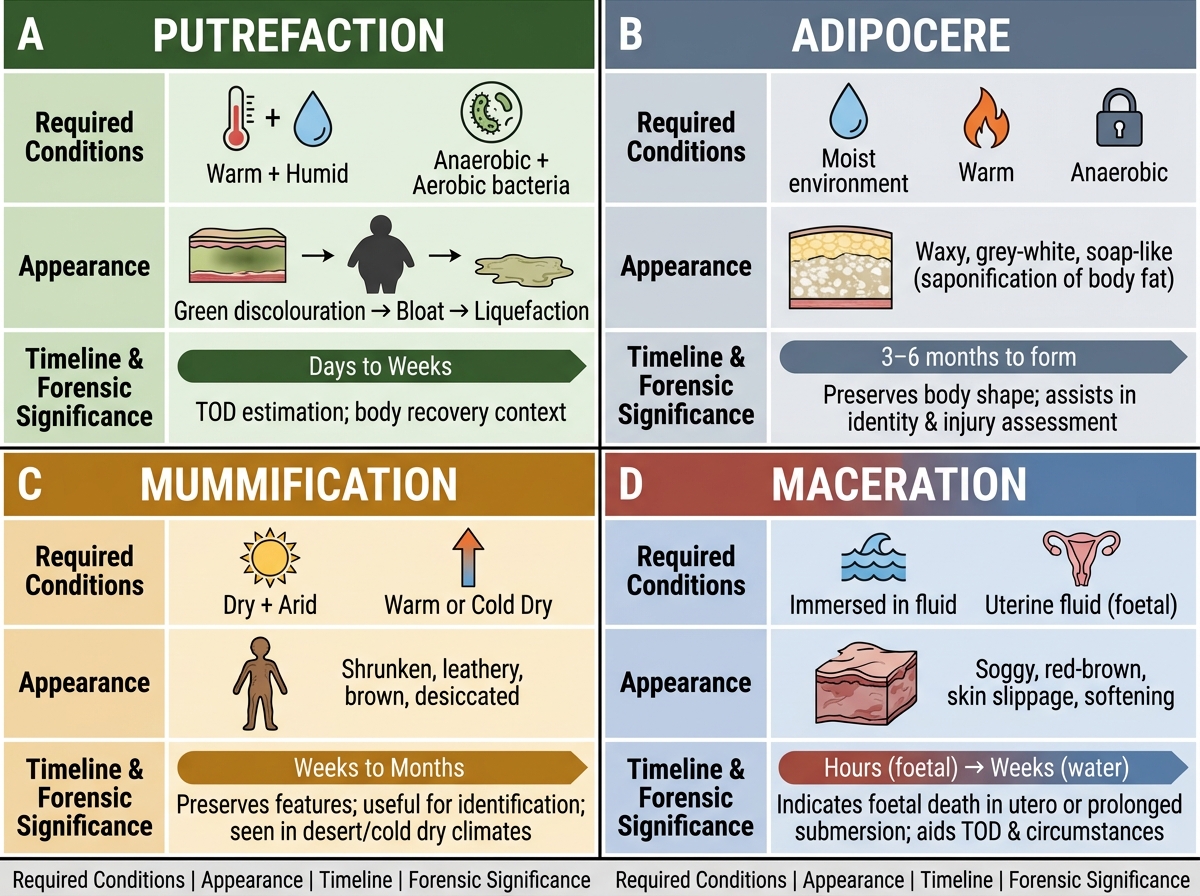
Late Post-Mortem Changes: Comparative Overview
| Change | Key Requirement | Appearance | Timeline |
|---|---|---|---|
| Putrefaction | Warm + humid + bacteria | Green → bloat → liquefaction | Days to weeks |
| Adipocere | Warm + moist + anaerobic | Waxy, grey-white, soap-like | 3-6 months to form |
| Mummification | Dry + warm + arid | Shrunken, leathery, brown | Weeks to months |
| Maceration | Fluid (water/uterine fluid) | Soggy, red-brown, skin slip | Hours (foetal) to weeks |
SELF-CHECK
A body is recovered from a well in a tropical region 6 months after the individual was reported missing. The body has a waxy, grey-white appearance with a rancid soap-like odour. Which late post-mortem change is most likely?
A. Putrefaction at an advanced stage
B. Mummification
C. Adipocere formation
D. Maceration
Reveal Answer
Answer: C. Adipocere formation
Adipocere forms when body fat is saponified into fatty acid salts in warm, moist, anaerobic conditions — exactly what is provided by submersion in a well in a tropical climate over 6 months. The characteristic appearance is waxy, grey-white, with a rancid/cheesy/soapy odour. Putrefaction would result in tissue liquefaction and eventual skeletonisation, not a waxy preserved state. Mummification requires dry conditions and produces a dark, leathery, shrunken body. Maceration produces a soggy, red-brown, skin-slipping appearance, typically in a shorter timeframe and without the waxy transformation.
Estimation of Time Since Death: Methods and Integration
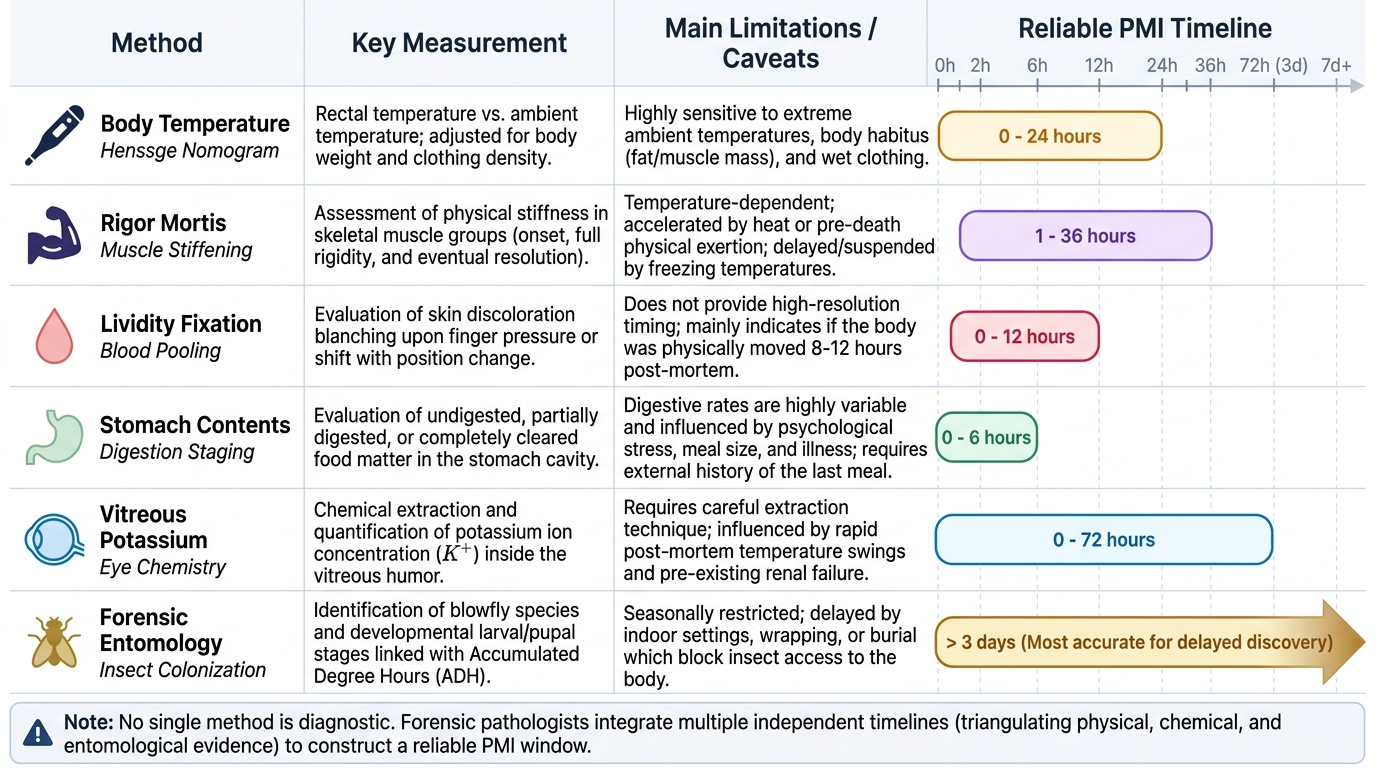
Post-mortem interval (PMI) estimation is one of the most practically important skills in forensic medicine. No single method is perfect; the forensic physician integrates multiple independent lines of evidence to arrive at a range rather than a precise time. Each method has a different optimal window of reliability, and discordant results require explanation.
Body temperature (algor mortis) — most reliable in the first 24 hours. Using the Henssge nomogram (or the simplified formula) with rectal temperature and ambient temperature, a PMI can be estimated with reasonable accuracy in the early post-mortem period. Important caveats: the measurement must be rectal (axillary temperature is unreliable post-mortem); the ambient temperature at the time of death (not just at the time of examination) must be known or estimated; the body habitus and clothing affect the corrective factor.
Rigor mortis staging. Using the temperature-dependent timings as a guide (onset 1-2h, fully established 6-12h, resolution beginning 24-36h at ~25-30°C), the forensic physician can place the PMI within one of three windows. Critically, the staging must account for ambient temperature — a body found in a cold storage room with no rigor does NOT mean the PMI is <1h; rigor may have been suppressed by cold.
Post-mortem lividity fixation. Mobile lividity (blanches and shifts on pressure) = <8-12h. Fixed lividity = >8-12h. Fixed lividity in the 'wrong' position (inconsistent with the body's final position) = body moved >8-12h after death.
Stomach contents. The state of digestion of the last meal provides a rough guide: undigested food in the stomach = death within ~2 hours of eating; partially digested food = 2-4 hours; empty stomach = ≥4-6 hours after last meal. This is an imprecise method but useful when combined with witness information about the last meal.
Forensic entomology. Blow flies (Calliphora, Lucilia, and Sarcophaga species) arrive at a body within minutes of death and lay eggs on moist orifices (eyes, nose, mouth, wounds). The developmental stages of insect larvae (eggs → 1st instar → 2nd instar → 3rd instar → pupa → adult) have known time schedules dependent on ambient temperature. In cases of delayed discovery (days to months), the accumulated degree hours (ADH) method using temperature-corrected larval development data provides a PMI estimate accurate to within hours in favourable conditions. Forensic entomology is the most accurate method for estimating PMI beyond 3 days.
Vitreous (ocular) chemistry. Potassium ions are released from retinal cells in a predictable linear fashion after death; vitreous potassium concentration rises at approximately 0.14-0.17 mmol/L per hour after death. While individual variation limits precision, it provides a useful check when body temperature and rigor mortis staging are compromised. Other vitreous analytes (glucose, urea, chloride) provide supporting biochemical context.
Putrefaction staging. In decomposed remains, the stage of putrefaction provides a rough lower bound for the PMI. The presence of insect casts/puparia (indicating completed insect generations) can extend the entomological estimate into months.
Provided image
Practical approach to PMI estimation:
1. Note ambient conditions (temperature, humidity, exposure) BEFORE moving the body
2. Measure rectal temperature and ambient temperature — apply Henssge nomogram
3. Assess rigor mortis stage (jaw, neck, trunk, limbs) and account for ambient temperature
4. Assess lividity (distribution, colour, fixation)
5. Document stomach contents if accessible
6. Collect insect evidence (larvae stages, puparia) with temperature data
7. Examine vitreous for potassium if body temperature method is unreliable
8. Report a range, not a single time — every method has uncertainty; the integrated range is more reliable and more honest than a false precise estimate
CLINICAL PEARL
Cherry-red lividity: the first clue to CO poisoning. When post-mortem lividity is cherry-red or bright-red instead of the usual blue-purple, carbon monoxide poisoning must be the primary diagnosis until proven otherwise. Carboxyhaemoglobin (COHb) is a stable, bright-red compound that gives the classic lividity colour and also imparts a pink flush to the skin, mucous membranes, and internal organs. The forensic physician must note this finding immediately and initiate full scene investigation for CO sources (faulty heating, blocked chimneys, running vehicle in closed garage). A secondary cause of cherry-red lividity is severe hypothermia, where preserved oxyhaemoglobin gives a similar appearance. The toxicology result (COHb %) is the confirmatory test, but the cherry-red lividity is the flag that triggers the investigation — and it should be the first thing checked at every body examination.
Medicolegal Application of Post-mortem Changes
Post-mortem changes do not merely indicate when a person died — they carry evidentiary information that can reconstruct the events surrounding death, identify causes, and challenge or confirm alibis and crime narratives.
PMI in criminal investigation. The PMI range establishes the window within which the death must have occurred, against which witness accounts, phone records, and CCTV footage are tested. A PMI estimate of 'death occurred between 10 PM Friday and 2 AM Saturday' directly tests whether an alibi holds. Courts treat PMI estimates as expert opinion, with the range (not a single time) representing the honest scientific position.
Fixed lividity and body movement. If post-mortem lividity is fixed posteriorly (back/buttocks) but the body is found face-down, the body was moved — face-down — more than 8-12 hours after death. This is direct physical evidence that the body was repositioned after death. Conversely, lividity consistent with the body's final position argues against post-mortem movement.
Cadaveric spasm and manner of death. In apparent suicide by self-inflicted firearm wound, finding the weapon in a cadaveric-spasm grip is strong evidence the person was holding the gun at the moment of death. In drowning, cadaveric spasm of the hands clutching weeds or sand supports a genuine drowning in that location (difficult for a perpetrator to fabricate). The forensic pathologist must specifically look for and document cadaveric spasm.
Adipocere and long-delayed discovery cases. When a body is found years after death (in a damp well, flooded basement, or buried in wet soil), adipocere preservation may allow wound identification and identity confirmation that would be impossible in a fully skeletonised body. It may also confound PMI estimation if mistaken for putrefaction.
Foetal maceration and time of foetal death. In medico-legal cases involving stillbirth or maternal concealment of pregnancy, the degree of foetal maceration at birth (mild = few hours, moderate = 1-3 days, severe = >3 days) helps estimate when foetal death occurred and whether the neonate survived birth — a critical distinction for IPC Section 304 (infanticide vs stillbirth).
Provided image
Key medicolegal rules from post-mortem changes:
- Cherry-red lividity → investigate for CO/cyanide poisoning immediately
- Fixed lividity inconsistent with body position → body was moved post-mortem
- Cadaveric spasm → preserve and photograph before moving the body; document object in grip
- All PMI estimates should be given as ranges with stated assumptions (temperature, conditions)
- Post-mortem changes should be documented on arrival at the scene, before the body is moved
SELF-CHECK
At a homicide scene, a body is found lying face-up. Post-mortem lividity is fixed and dark purple on the anterior surface (chest, face, front of thighs). Rigor mortis is fully established. Ambient temperature is 26°C. What conclusion can be drawn?
A. The body has been in this position since death, approximately 12-18 hours ago
B. The body was face-down for at least 8-12 hours after death, then turned face-up
C. The lividity pattern indicates cyanide poisoning
D. Rigor mortis is inconsistent with lividity and an error has been made
Reveal Answer
Answer: B. The body was face-down for at least 8-12 hours after death, then turned face-up
Fixed lividity on the anterior surface (face, chest, front of limbs) while the body is face-up means the blood pooled anteriorly (as it would if the body was face-down) and then fixed before the body was turned. Lividity fixes at 8-12h after death. Since the lividity is now fixed on the anterior surface but the body is found face-up, the body must have been face-down for at least 8-12 hours post-mortem, then rolled face-up. This is direct physical evidence the body was moved. Fully established rigor (6-12h to fully establish) and ambient 26°C are consistent with approximately 12-24h post-mortem. Cyanide/CO poisoning would produce cherry-red or dark lividity — not simply anterior distribution. Rigor and lividity are independent processes and give complementary, not contradictory, information.
KEY TAKEAWAYS
Post-mortem changes are the body's biological clock, offering a multi-layered record of time and environment after death. Early changes (first 24-48h) include: algor mortis (body cooling, ~1.5°C/h, Henssge nomogram); post-mortem lividity (gravitational blood pooling, fixed at ~8-12h, cherry-red in CO poisoning, brown in methaemoglobinaemia); and rigor mortis (ATP-depletion stiffening, onset 1-2h, fully established 6-12h, resolving 24-36h — all at ambient ~25-30°C and temperature-dependent). Cadaveric spasm (instantaneous, no flaccid interval, preserved grip), cold stiffening, and heat stiffening are distinct from rigor mortis. Late changes include: putrefaction (bacterial decomposition, green → bloat → liquefaction); adipocere (saponification of fat in warm moist anaerobic conditions); mummification (desiccation in dry warm conditions); and maceration (sterile autolysis in fluid, intrauterine or aquatic). PMI estimation integrates body temperature (Henssge), rigor staging, lividity fixation, stomach contents, forensic entomology, and vitreous potassium — always expressed as a range with stated temperature assumptions.
REFLECT
You are dispatched to examine a body found in a closed room in Chennai in May (ambient temperature estimated at 32-35°C). The body is a 50-year-old man found by neighbours who had not seen him for approximately 3 days. You observe: significant bloating and green discolouration of the abdomen; skin slippage on the hands; fixed purple lividity on the back; rigor mortis absent (the body is flaccid); and a faint smell of decomposition. What are the specific post-mortem changes present? In what order did they develop? What does the absence of rigor mortis indicate — and why must you account for the high ambient temperature in your interpretation? What methods would you use to arrive at a PMI estimate, and what range would you suggest based on the available evidence? What additional scene evidence would you look for?