Page 4 of 14
FM2.5-6 | Natural, Unnatural & Sudden Death — SDL Guide
Learning Objectives
- Define natural and unnatural death and classify deaths by manner
- Describe the cardiovascular and non-cardiovascular causes of sudden natural death, including causes specific to young adults and athletes
- Define sudden unexplained death syndrome (SUDS/SIDS) and outline the systematic investigation protocol
- Outline the legal obligations of a physician encountering sudden or unnatural death, including police notification and autopsy referral under the Cr.PC
INSTRUCTIONS
Every unexpected death creates a medicolegal problem: is this a natural death from disease, or an unnatural death requiring police investigation? The doctor who first sees the body — whether a GP in the community or a casualty officer — must make this initial classification correctly. A natural death incorrectly certified as unnatural triggers unnecessary police action and distresses families; an unnatural death certified as natural can conceal a murder. This module builds the classification framework for natural and unnatural death, explores the common causes of sudden natural death (with particular focus on young adults), and clarifies the doctor's legal duties under Indian law.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old professional footballer collapses during a practice session and is found unresponsive with no palpable pulse. He is brought to the emergency department but cannot be resuscitated. There is no history of prior illness, no injury, and no witnesses to any foul play. The police arrive at the hospital requesting the death certificate. The junior resident is faced with an immediate dilemma: is this a natural death (which she can certify herself) or an unnatural death (which must be referred to the police and may require forensic autopsy)? The answer hinges on a classification that every practising doctor must understand.
WHY THIS MATTERS
The classification of a death as natural or unnatural is not an academic exercise — it determines the entire subsequent legal and investigative pathway. A natural death can be certified by the attending physician on a standard MCCD, and the body can be released for disposal. An unnatural death must be reported to the police, and the body referred to a forensic pathologist for autopsy; the police then conduct an inquest under the Code of Criminal Procedure (Cr.PC). Failure to report an unnatural death — even in good faith — may expose the physician to criminal liability under Section 176 (Cr.PC: informing magistrate of certain deaths) and IPC Section 304A (causing death by negligence if the death was due to medical error). Understanding sudden death is equally urgent: the sudden unexpected death of a young person is always a medicolegal event until proven otherwise, and the forensic pathologist's report may be the only evidence establishing whether the death was natural, accidental, or homicidal.
RECALL
Recall from your Year 1 physiology and pathology foundations: the cardiovascular system maintains perfusion through a rhythmically contracting heart, patent coronary arteries, and intact electrical conduction. Ischaemic heart disease results from atherosclerotic narrowing of coronary arteries, leading to myocardial infarction or fatal arrhythmia. Recall also from fp1: the syncope mode of death represents primary cardiac failure — this is the final common pathway in most cases of sudden cardiac death. The brain's vulnerability to ischaemia (neurons die in 4-6 min) explains why sudden cardiac failure produces rapid death without warning. From the prior module on death types, you know that the manner of death (natural, accident, homicide, suicide) is distinct from the cause and mode — that tripartite distinction is the scaffold for this module.
Natural vs Unnatural Death: Definitions and Medicolegal Classification
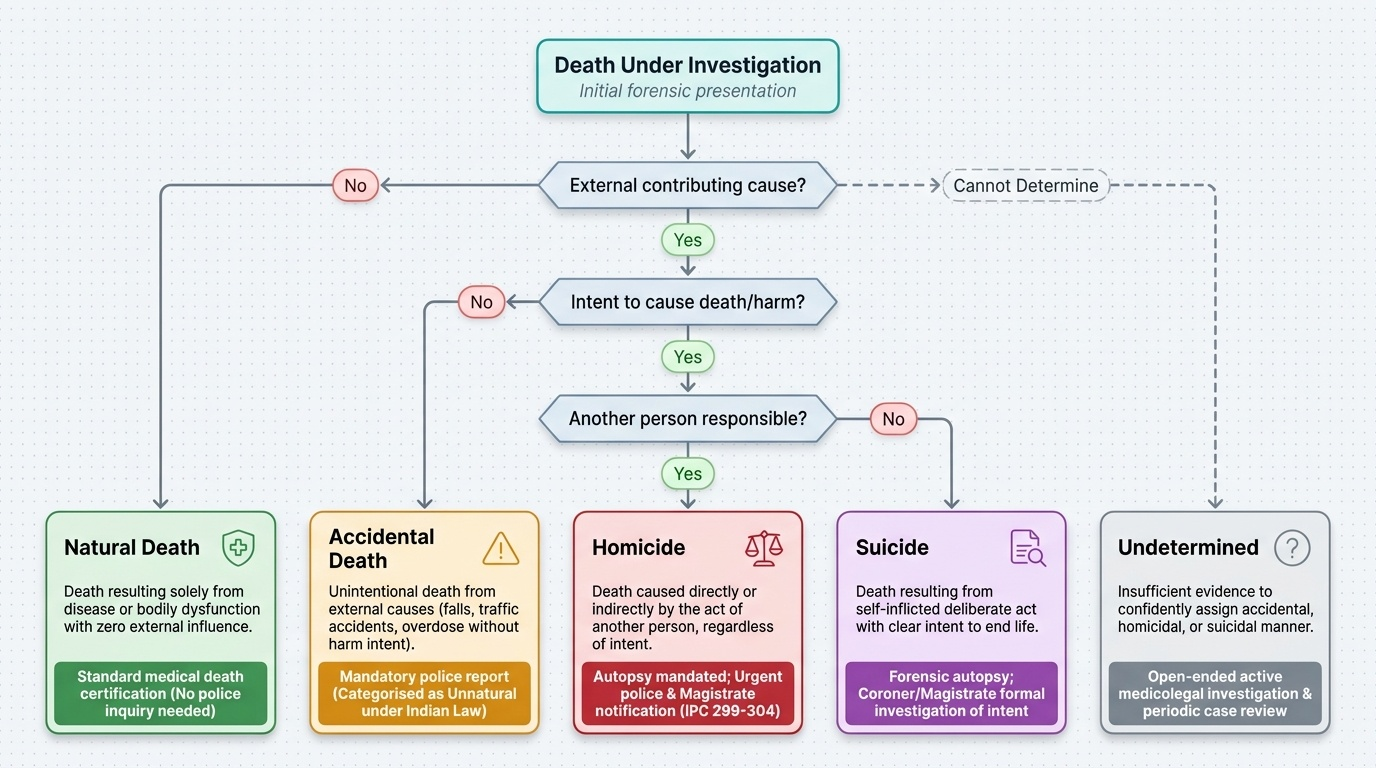
The classification of death by manner is the forensic pathologist's most fundamental determination. Manner answers the question: Why did this death occur in a social sense? — not the biological cause, but the circumstance. The four recognised manners of death, used in all forensic and death registration systems, are:
- Natural death: death resulting solely from disease or natural bodily dysfunction, with no external contributing cause. For a death to be certified as natural, the certifying physician must be satisfied that no trauma, poisoning, negligence, or external intervention played any causal role. Natural deaths include all deaths from infections, cardiovascular disease, neoplasia, organ failure, and congenital abnormalities — provided these were not triggered or exacerbated by external causes.
- Accidental death: death resulting from an unintentional external cause — a fall, a road traffic accident, drowning, a workplace injury, a drug overdose in a person who did not intend to harm themselves. The key element is absence of intent to cause death or injury. In Indian law, accidental deaths are medico-legally categorised as unnatural and must be reported to the police.
- Homicide: death caused by the act of another person, regardless of intent. Forensic homicide (in the medicolegal sense) is broader than murder; it includes manslaughter, culpable homicide, and any death where another person's action was causally responsible. The IPC distinctions (IPC 299-304: culpable homicide, murder) are determined by the court after the forensic pathologist establishes that the death was not natural.
- Suicide: death resulting from a self-inflicted deliberate act with intent to end one's own life. Establishing suicide requires evidence of intent — the forensic pathologist documents the physical findings (entry wound characteristics, note, circumstances), but the manner determination involves coroner/magistrate investigation beyond the autopsy alone.
A fifth category, undetermined, is used when investigation cannot establish the manner with reasonable confidence — typically when the evidence supports both accidental and suicidal (or accidental and homicidal) interpretations.
The medicolegal boundary between natural and unnatural death hinges on two questions:
- Was there any external contributing cause?
- Was the disease the sole cause, or did it occur in a context of potential foul play?
For example, a person with severe atherosclerosis who dies after a minor road traffic accident may have a 'natural' cardiac death precipitated by the stress of the collision — in which case the manner may be accidental (unnatural), not natural, because the external cause contributed.
Provided image
| Manner | Key Feature | Medicolegal Action |
|---|---|---|
| Natural | Disease alone; no external cause | MCCD by attending physician; no police referral required |
| Accidental | Unintentional external cause | Police report; forensic autopsy |
| Homicide | Act of another person | Police report; forensic autopsy; criminal investigation |
| Suicide | Deliberate self-infliction | Police report; inquest; forensic autopsy |
| Undetermined | Cannot classify | Police report; full forensic investigation |
SELF-CHECK
A 65-year-old man with known hypertension slips on a wet floor, sustains a minor head injury, and dies 6 hours later from a hypertensive intracerebral haemorrhage. Which manner of death is most appropriate?
A. Natural — because the immediate cause of death (ICH) is a natural disease
B. Accidental — because the fall (external cause) precipitated the fatal event
C. Undetermined — because the contribution of the fall cannot be quantified
D. Homicide — because someone left the floor wet
Reveal Answer
Answer: B. Accidental — because the fall (external cause) precipitated the fatal event
Although the immediate mechanism of death (intracerebral haemorrhage) is a disease process, the manner of death is accidental because the fall (an external unintentional cause) precipitated the haemorrhage. A death from natural disease can still be classified as unnatural/accidental if an external event was causally connected to it. This distinction is critical: the doctor must refer this case to the police even if the patient had a known history of hypertension. Option C (undetermined) would apply only if the causal link between the fall and the haemorrhage could not be established at all. Option D (homicide) requires intent by another person — leaving a floor wet is negligent but requires a separate negligence assessment.
Sudden Natural Death: Cardiovascular and Non-Cardiovascular Causes
Sudden death is defined as an unexpected, rapid death occurring within 1 hour of the onset of symptoms in a witnessed case, or within 24 hours of the person being last seen alive in an unwitnessed case, and arising from an internal (natural) cause. The sudden and unexpected nature of the death is what triggers medicolegal concern — a person apparently in good health who is found dead always raises the question of foul play, and a systematic approach to the underlying cause is essential.
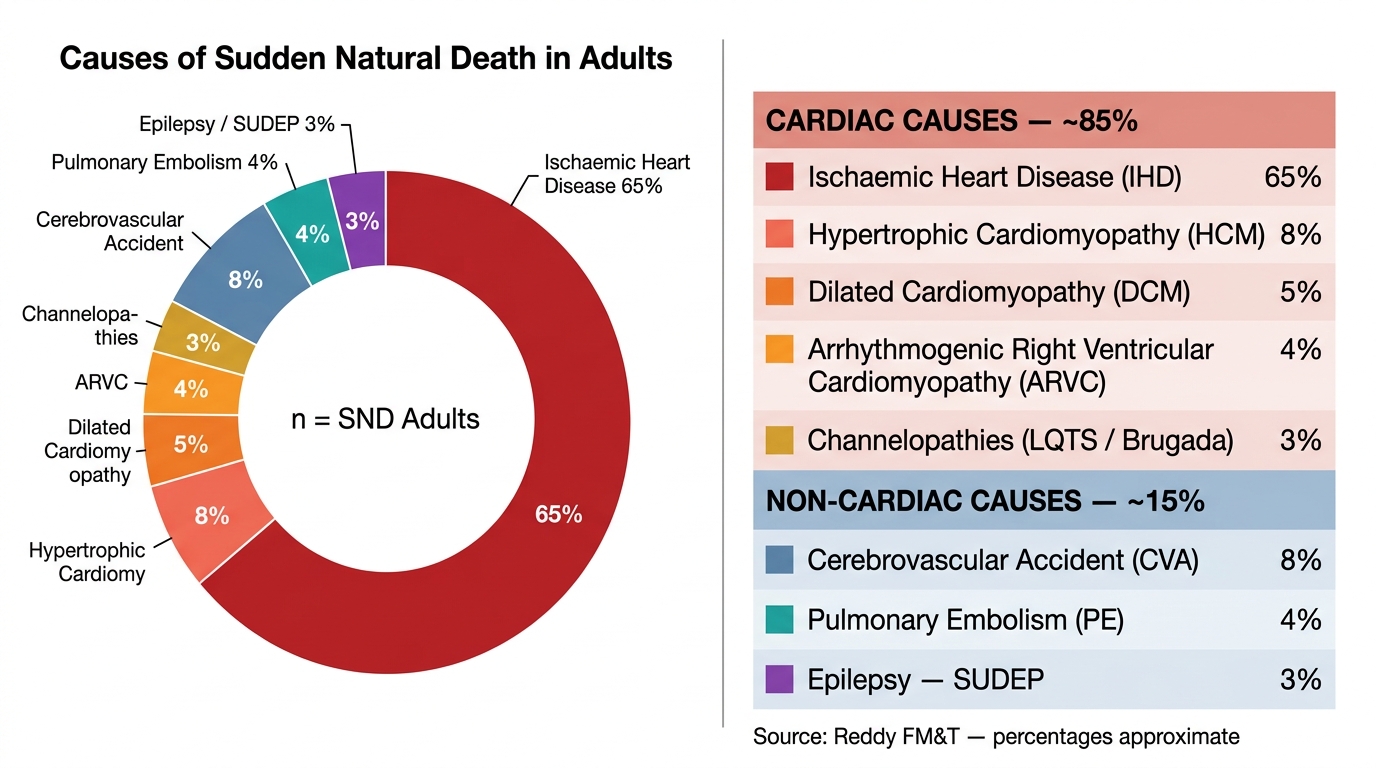
Among adults, approximately 70-80% of sudden unexpected natural deaths are cardiovascular in origin (per Reddy's FM&T). The leading causes are:
Cardiovascular causes of sudden natural death:
- Ischaemic heart disease (IHD): the single most common cause overall — coronary artery atherosclerosis leading to acute myocardial infarction or a fatal ventricular arrhythmia (ventricular fibrillation or pulseless ventricular tachycardia). Many victims have no prior symptoms. At autopsy, fresh coronary artery occlusion (thrombosis on a ruptured plaque) and areas of early myocardial necrosis are the hallmarks
- Hypertrophic cardiomyopathy (HCM): the leading cause of sudden death in young athletes — a genetic disorder (autosomal dominant in most cases, mutations in sarcomeric proteins such as β-myosin heavy chain) causing asymmetric ventricular hypertrophy. Sudden death results from outflow tract obstruction or fatal arrhythmia during physical exertion. Autopsy shows marked ventricular hypertrophy (often >500g heart weight) with myocyte disarray
- Dilated cardiomyopathy: the heart is enlarged and hypokinetic; sudden death occurs from ventricular arrhythmia. May be idiopathic, post-viral (especially Coxsackievirus B), or peripartum
- Arrhythmogenic right ventricular cardiomyopathy (ARVC): replacement of right ventricular myocardium with fibro-fatty tissue; a significant cause of sudden death in young adults, especially during exercise; autosomal dominant (desmoplakin, plakophilin mutations)
- Channelopathies (ion channel diseases): Long QT syndrome, Brugada syndrome, short QT syndrome, and catecholaminergic polymorphic ventricular tachycardia (CPVT) — structurally normal hearts with inherited electrical dysfunction; may leave NO macroscopic findings at autopsy, requiring genetic/molecular testing ('molecular autopsy')
Non-cardiovascular causes of sudden natural death:
- Cerebrovascular accidents: rupture of a berry (saccular) aneurysm at the circle of Willis → subarachnoid haemorrhage; hypertensive intracerebral haemorrhage; massive ischaemic stroke. Berry aneurysm rupture classically presents as 'thunderclap headache' and can cause instantaneous death
- Pulmonary embolism: massive PE causing acute right heart failure and cardiac arrest; often following deep vein thrombosis (DVT) in immobile, post-surgical, or pregnant patients
- Epilepsy — SUDEP (Sudden Unexpected Death in Epilepsy): poorly understood mechanism; most common in young adults with uncontrolled generalised tonic-clonic seizures
- Aortic dissection/rupture: acute Stanford Type A dissection can cause instantaneous death from cardiac tamponade or aortic valve disruption
Leading Causes of Sudden Natural Death in Adults (Reddy FM&T)
- IHD = most common cause overall (any age, predominantly older adults)
- HCM = most common cause in young athletes (under 35)
- Berry aneurysm rupture = important cause in young adults (20-40) with no cardiac history
- Channelopathies = autopsy-negative sudden death → molecular autopsy required
SELF-CHECK
A 19-year-old male cricket player collapses and dies during a match. Autopsy shows a markedly enlarged heart (weight 620g) with asymmetric septal hypertrophy and histological myocyte disarray. No coronary artery disease is found. What is the most likely diagnosis?
A. Ischaemic heart disease
B. Hypertrophic cardiomyopathy (HCM)
C. Arrhythmogenic right ventricular cardiomyopathy (ARVC)
D. Long QT syndrome
Reveal Answer
Answer: B. Hypertrophic cardiomyopathy (HCM)
The combination of a young athlete, marked ventricular hypertrophy (>500g heart weight), asymmetric septal thickening, and myocyte disarray on histology is pathognomonic of hypertrophic cardiomyopathy (HCM). HCM is the leading cause of sudden cardiac death in young athletes in India. IHD would show coronary artery disease and myocardial infarction on autopsy, not hypertrophy and disarray. ARVC characteristically involves the right ventricle with fibro-fatty replacement. Long QT syndrome produces a structurally normal heart — there would be no hypertrophy or histological changes at autopsy.
Sudden Unexplained Death: SIDS, SUDS, and the Autopsy Protocol
Despite thorough clinical history review, scene investigation, and complete autopsy, a proportion of sudden deaths remain unexplained. These are categorised as sudden unexplained death syndromes, and require a systematic, protocol-driven investigation to avoid both false-positive attributions (certifying a natural cause that wasn't there) and false negatives (missing a subtle cause or an injury).
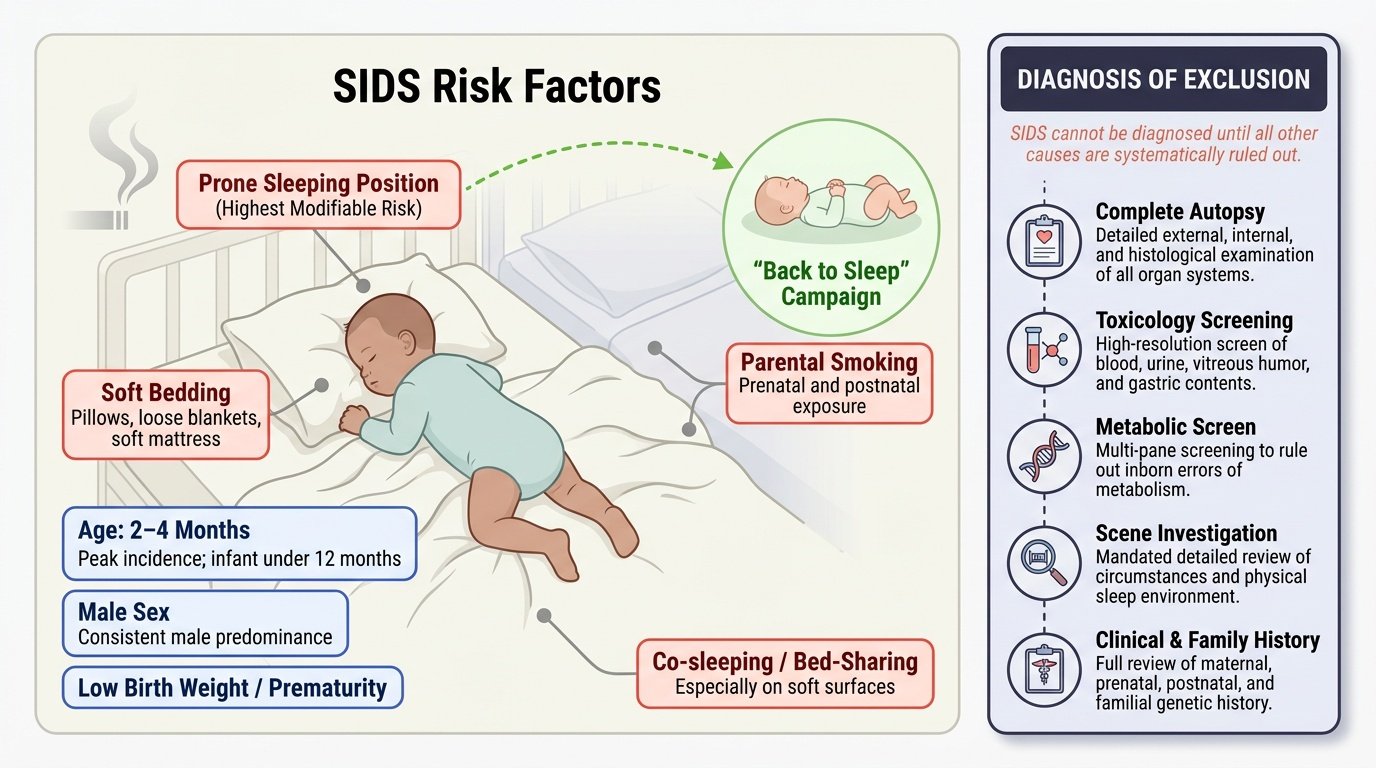
Sudden Infant Death Syndrome (SIDS) is defined as the sudden unexpected death of an infant under 12 months of age (peak age 2-4 months; male predominance) that remains unexplained after a thorough investigation comprising a complete autopsy, review of the medical history, and investigation of the death scene. It is a diagnosis of exclusion — SIDS cannot be diagnosed until all other causes have been systematically ruled out. Risk factors include: prone sleeping position (the most modifiable risk factor — the 'Back to Sleep' campaign reduced SIDS rates substantially), soft bedding, parental smoking, low birth weight, and co-sleeping. SIDS is NOT caused by vaccination, and it is NOT smothering (though the two are forensically challenging to distinguish in some cases, which is why scene investigation is mandatory).
Sudden Unexplained Death Syndrome in adults (SUDS) — also called sudden unexpected nocturnal death syndrome (SUNDS) in some populations (notably reported in young Southeast Asian and Filipino men during sleep) — describes sudden death in an adult with no identified structural or toxicological cause despite full investigation. Molecular autopsy (genetic testing for channelopathies) has revealed Brugada syndrome as a cause in many SUNDS cases.
The forensic autopsy protocol for sudden unexplained death must be systematic:
1. Thorough external examination: any signs of injury, petechiae, cyanosis, needle marks
2. Complete internal examination: all organs; heart weight and dimensions; coronary artery dissection and cross-sectioning at 3mm intervals; valvular inspection; histological sampling of myocardium, brain, and lung
3. Neuropathological examination: in adults — brain weight, slice sections, histology for subtle haemorrhage or encephalitis; in infants — full brain examination
4. Toxicological screening: blood, urine, vitreous humour, gastric contents; screens for alcohol, therapeutic drugs, illicit drugs, carbon monoxide
5. Microbiological samples: in infants especially — nasal swabs, blood culture, lung swabs to identify occult sepsis
6. Metabolic screening: in infants — blood spots for inherited metabolic disorders (e.g. MCAD deficiency — medium-chain acyl-CoA dehydrogenase deficiency — is an important mimic of SIDS)
7. Genetic/molecular autopsy: if no structural cause is found — targeted genetic panel for channelopathies (LQTS, Brugada, CPVT)
Provided image
- SIDS: age <1 year; peak 2-4 months; diagnosis of exclusion; prone position is the key modifiable risk
- SUNDS: adult, often during sleep; linked to Brugada syndrome in many cases
- A complete autopsy protocol including toxicology + histology is mandatory before a 'sudden unexplained death' label is applied
CLINICAL PEARL
The SIDS-smothering dilemma: The autopsy findings in SIDS and in deliberate smothering (infanticide by overlaying or suffocation) are often identical — both may show petechiae in the lungs and thymus, pulmonary congestion, and no specific cause. The forensic distinction requires: complete scene investigation, family history review (prior unexplained infant deaths in the family are a significant red flag — recurrent SIDS in one family is statistically unusual and raises concern for non-accidental injury), and multidisciplinary case review. A forensic pathologist who certifies SIDS without scene investigation has not met the diagnostic standard. Equally, a pathologist who labels all sudden infant deaths as infanticide without evidence is making a serious error. The correct position is: thorough investigation, honest uncertainty where it exists, and the diagnosis of exclusion documented carefully.
Medicolegal Issues in Sudden and Unnatural Death
Every physician practising in India must know the legal obligations that attach to different categories of death. The Code of Criminal Procedure (Cr.PC) and the Registration of Births and Deaths Act (RBD Act) together govern what must be done when a person dies.
Reportable deaths — deaths that MUST be reported to the police and/or magistrate — include:
- All unnatural deaths: accidental, homicidal, suicidal
- All sudden, unexpected, and unexplained deaths (until natural cause is established)
- Death of a person admitted for less than 24 hours without an established diagnosis
- Death in police custody, judicial custody, or any institution
- Death under suspicious circumstances
- Death associated with medical procedure (anaesthesia death, post-operative death in suspicious circumstances)
Under Section 174 of the Cr.PC, a police officer is required to investigate sudden, suspected unnatural, or unknown-cause deaths and may order an inquest. Under Section 176 Cr.PC, a magistrate's inquest may be ordered in deaths in custody or other specified circumstances. The forensic autopsy (medico-legal autopsy, post-mortem examination) is performed under police/magistrate requisition; the report is a legal document and the forensic pathologist may be called to testify.
The attending doctor's duties:
1. Do not issue a death certificate for a death that falls into a reportable category — report to the police first
2. Do not interfere with the body (cleaning, repositioning) before the police have been notified and a decision made regarding autopsy
3. Preserve any samples (blood, urine, gastric aspirate) if poisoning is suspected
4. Document all findings contemporaneously — notes made at the time carry far greater evidential weight than retrospective accounts
5. If in doubt about the category, err on the side of reporting — you can never be prosecuted for reporting a death that turns out to be natural; you can be prosecuted for failing to report one that turns out to be unnatural
Sudden death in the community:
When a general practitioner or community health worker encounters a sudden death outside the hospital, the standard is: if the person was under your regular care with a known life-limiting illness and the death is consistent with the natural progression of that illness, a natural-death certificate can be issued. In all other cases — unknown person, no known diagnosis, unexpected death — the body must be referred to police before any certificate is issued.
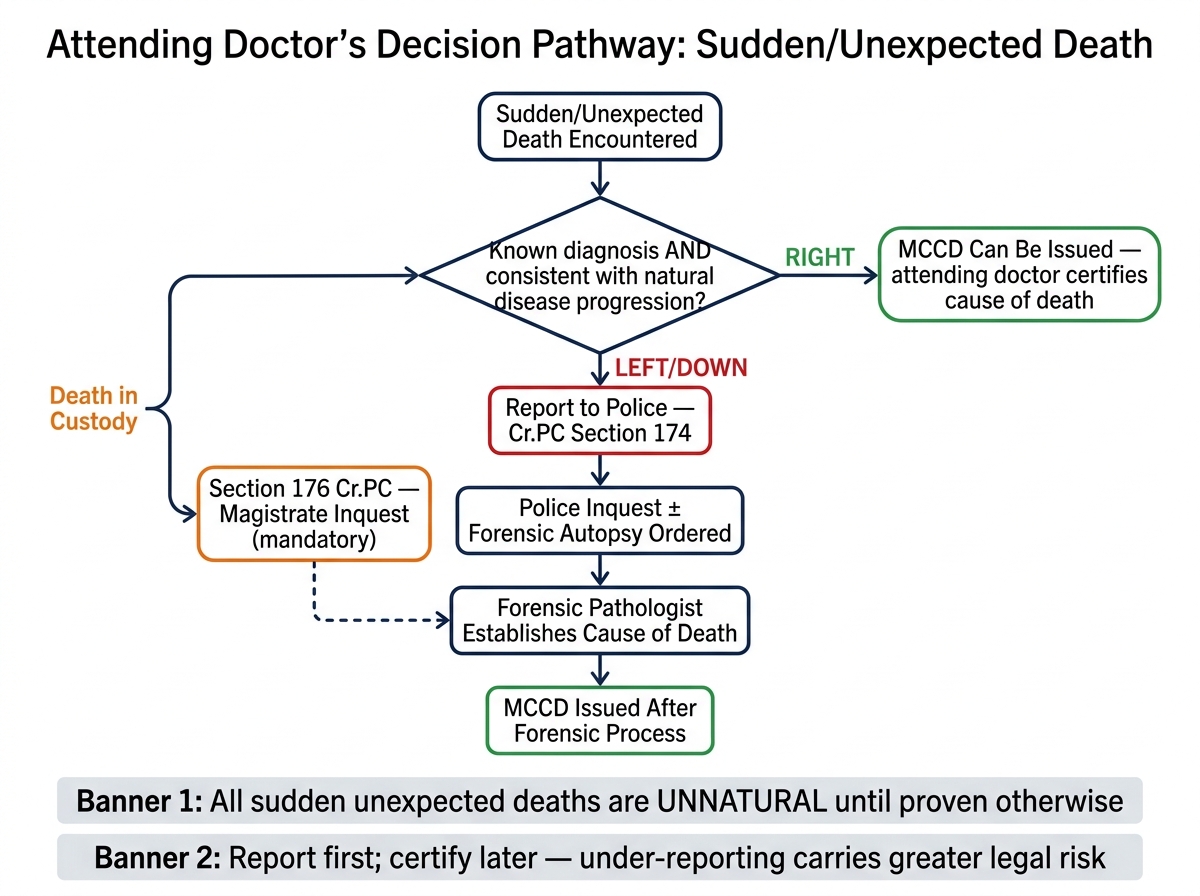
Decision Pathway for Sudden/Unexpected Death: MCCD vs. Medico-Legal Reporting
- All sudden unexpected deaths are unnatural until proven otherwise
- Report first; certify later — the physician faces greater legal risk from under-reporting than over-reporting
- Preserve physical evidence, document contemporaneously
SELF-CHECK
A 35-year-old woman is brought to casualty after being found unresponsive at home. Resuscitation fails. Her family states she was 'perfectly healthy'. There is no known diagnosis, no evidence of injury, and no suspicious circumstances. What is the MOST appropriate immediate action for the casualty physician?
A. Issue a death certificate noting 'cardiac arrest — natural cause' since there is no evidence of foul play
B. Report the death to the police before issuing any certificate, as this is a sudden unexpected death
C. Wait 24 hours and then issue the certificate if no investigation is requested
D. Refer the family to the civil surgeon's office to issue the certificate
Reveal Answer
Answer: B. Report the death to the police before issuing any certificate, as this is a sudden unexpected death
A sudden, unexpected death in an apparently healthy 35-year-old without a known diagnosis is a reportable death under Cr.PC Section 174. The doctor MUST report to the police before issuing any certificate. Issuing a natural-cause certificate without investigation exposes the doctor to criminal liability if the death subsequently proves to be unnatural. There is no 24-hour waiting period — the obligation to report is immediate. The civil surgeon referral alone is not the correct primary action; police notification is the first step.
KEY TAKEAWAYS
Deaths are classified by manner: natural (disease alone) vs unnatural (accident, homicide, suicide, undetermined). This classification drives the medicolegal pathway — natural deaths are certified by the attending physician on an MCCD; unnatural deaths must be reported to police and may require forensic autopsy. Sudden natural death is an unexpected rapid death from natural disease, most commonly cardiovascular; ischaemic heart disease leads overall, while hypertrophic cardiomyopathy is the leading cause in young athletes. Non-cardiac causes include berry aneurysm rupture, pulmonary embolism, and SUDEP. When no cause is found after full autopsy and toxicology, the death is classified as sudden unexplained. SIDS (Sudden Infant Death Syndrome) is a diagnosis of exclusion for deaths in infants under 12 months, requiring complete autopsy, toxicology, metabolic screening, scene investigation, and — when warranted — molecular autopsy. The physician's legal duty is clear: all sudden unexpected deaths must be reported to police before any certificate is issued; failure to report is a criminal offence under the Cr.PC.
REFLECT
You are a general practitioner in a semi-urban practice. A family calls you urgently to the home of a 45-year-old man who was found collapsed and unresponsive in his bed in the morning. He had no known illness and had been seen at dinner the previous evening in apparent good health. No drugs, no alcohol, no signs of trauma. His wife is devastated and asking you to 'just sign the certificate so we can proceed with the funeral'. Consider: What category does this death fall into — natural, unnatural, or undetermined at this point? What are your legal obligations? What forensic findings at a subsequent autopsy might change your initial categorisation? If you later learn he had a prescription for propranolol (for 'hypertension') that his wife was unaware of, what new considerations arise? Write a brief medicolegal assessment of the situation.