Page 1 of 14
FM2.{3,7-8} | Death: Definition, Types & Modes — SDL Guide
Learning Objectives
- Define somatic (clinical) death and cellular (molecular) death, and explain the reversibility window
- Distinguish cortical death (persistent vegetative state) from brainstem death and describe the criteria for brain death certification
- Describe the three classical modes of death — coma, asphyxia, and syncope — and their pathophysiological basis
- Define suspended animation, list its causes, and explain its medicolegal significance
- Outline the statutory framework for brain death certification and its link to organ transplantation
INSTRUCTIONS
Death is not a single moment — it is a biological process and a legal event. For a forensic physician, understanding the precise definition and classification of death is foundational to every certification, every organ transplant decision, and every medicolegal inquiry. This module establishes the conceptual framework: the difference between whole-organism failure and cellular extinction, the critical distinction between cortical and brainstem death, the three classical modes of dying, and the danger of misidentifying suspended animation as death. These concepts underpin every subsequent topic in forensic pathology.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old construction worker is brought to the casualty department after being pulled from a collapsed foundation trench. He had been buried for approximately 20 minutes. On arrival, there is no palpable pulse, no spontaneous respiration, and the pupils are fixed and dilated. The attending physician is uncertain: has death occurred, or is this a rescuable state? The casualty officer knows that cerebral neurons begin to die within minutes of circulatory arrest, but the police are already on their way to collect a death report. How does the doctor decide — and what does the law require before that certificate is signed?
WHY THIS MATTERS
The definition of death has direct consequences that extend far beyond the clinical setting. A premature death certificate can result in burial of a living person, constituting a serious criminal offence and a professional catastrophe for the certifying doctor. Conversely, delayed certification blocks organ procurement from a brain-dead donor, denying a recipient their only chance of survival. The medicolegal boundaries between somatic death, cellular death, brain death, and suspended animation are not academic subtleties — they govern the legality of resuscitation withdrawal, the validity of a death certificate, the permissibility of organ transplantation, and the doctor's liability under the Indian Penal Code. Every doctor who certifies a death must understand exactly what they are certifying.
RECALL
Before exploring the forensic classification of death, recall the physiology of vital functions from Year 1. The three pillars of life are cardiac function (maintaining perfusion), respiratory function (oxygenation), and central nervous system function (regulation and consciousness). Cardiac output depends on electrical conduction through the SA node, AV node, and His-Purkinje system; circulatory arrest leads to loss of perfusion within seconds. Respiratory function requires intact brainstem respiratory centres (medulla oblongata); apnoea from brainstem failure is irreversible without mechanical support. At the cellular level, ATP generation via oxidative phosphorylation ceases when oxygen supply ends; neurons are most vulnerable because they cannot tolerate anaerobic metabolism for more than 4-6 minutes. These physiological anchors are the scaffold on which the forensic classification of death is built.
Somatic (Clinical) Death and Cellular (Molecular) Death
Somatic death (also called clinical death) is defined as the irreversible cessation of the integrated vital functions of the organism as a whole — specifically, permanent stoppage of the heartbeat, respiration, and central nervous system activity. Critically, the word 'irreversible' is key: in the first few minutes following apparent cardiorespiratory arrest, resuscitation can restore cardiac and respiratory function, and somatic death has not truly occurred until the window of reversibility has closed. This reversibility window is the clinical basis for cardiopulmonary resuscitation (CPR), defibrillation, and therapeutic hypothermia — all interventions that exploit the brief gap between functional cessation and irreversible cellular extinction.
Following somatic death, individual cells throughout the body continue to survive for varying periods depending on their metabolic requirements and oxygen reserves. Cellular death (also called molecular death) is the irreversible cessation of cellular metabolism — the point at which individual cells can no longer sustain life even with restored perfusion. Neurons in the cerebral cortex are the most vulnerable: in normothermic conditions (approximately 37°C), irreversible neuronal injury begins within 4-6 minutes of circulatory arrest. Cardiac myocytes survive for 20-30 minutes; renal tubular cells for up to 2 hours; skeletal muscle and connective tissue can remain viable for several hours. This staggered cellular death profile has immense practical implications: it is why kidneys, corneas, and heart valves can be harvested from a recently deceased donor within defined time windows, while the brain — the first to die — cannot be restored.
The forensic significance of distinguishing somatic from cellular death is that the law requires certification of somatic death; no doctor is expected to await complete molecular extinction before issuing a death certificate. However, the certifying doctor must be certain that the state is truly somatic death and not a reversible condition such as deep anaesthesia or suspended animation (addressed below).
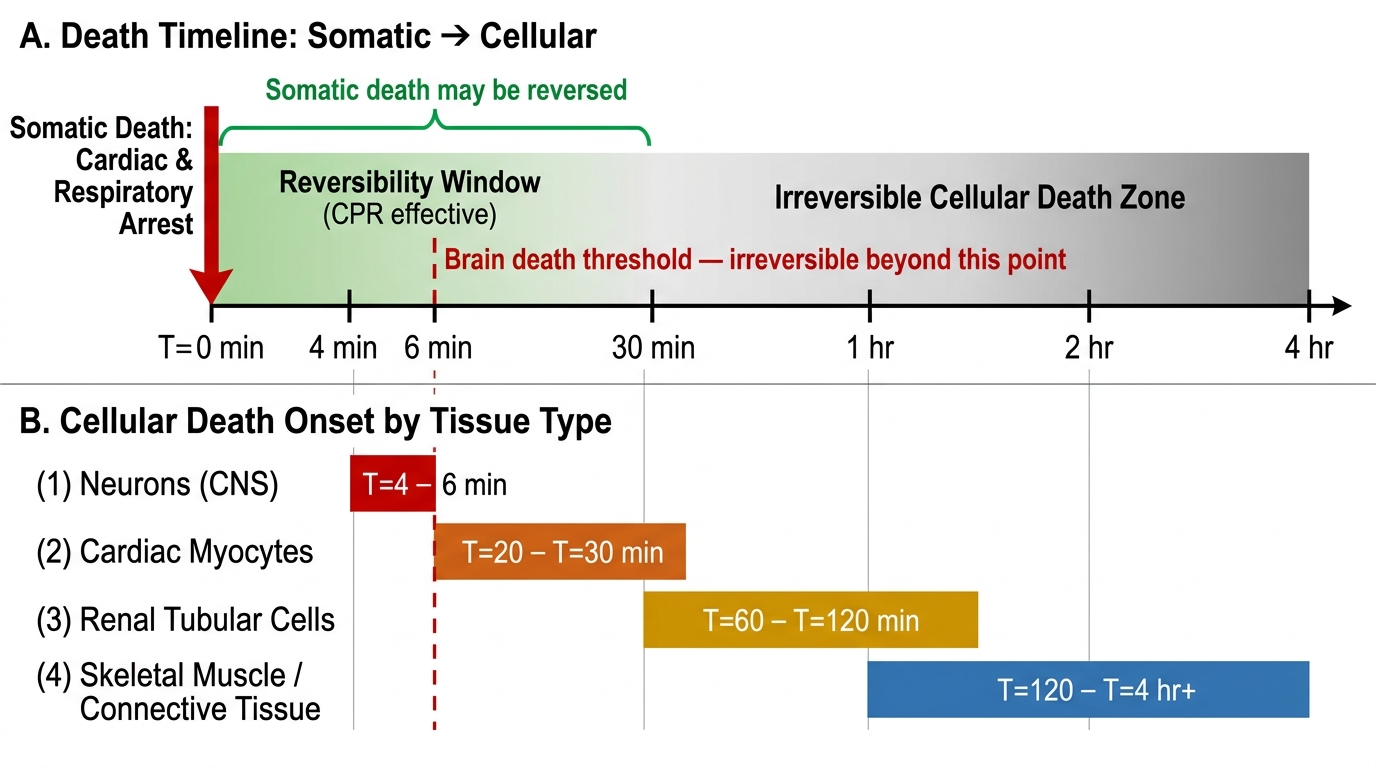
Figure: Somatic to Cellular Death — Timeline and Tissue-Specific Progression
- Somatic death hallmarks: no pulse, no respiration, no response to stimulation, fixed dilated pupils
- Cellular death progression (at ~37°C): neurons 4-6 min → cardiac myocytes 20-30 min → renal cells ~2 h → skeletal muscle/connective tissue several hours
- Reversibility window: somatic death may be reversed by CPR within 4-6 min (brain limit); restoration of circulation after this window results in return of cardiac/respiratory function but irreversible brain damage
SELF-CHECK
A patient is successfully resuscitated after 3 minutes of cardiac arrest with CPR. Which of the following best describes the stage of death that was present and then reversed?
A. Cellular (molecular) death
B. Somatic (clinical) death — reversibility window still open
C. Brain death
D. Suspended animation
Reveal Answer
Answer: B. Somatic (clinical) death — reversibility window still open
Somatic (clinical) death refers to the cessation of integrated vital functions — it is defined as irreversible, but in the early minutes the 'irreversibility' has not yet been confirmed and resuscitation is attempted. When CPR within 3 minutes successfully restores circulation before cellular death is complete, we say the patient was in the reversible phase of somatic death (or apparent death). Cellular death would have been irreversible and not rescued. Brain death requires formal certification criteria and is not consistent with successful resuscitation. Suspended animation applies to conditions where vital signs are imperceptible due to extreme metabolic depression (e.g. hypothermia), not cardiac arrest amenable to CPR.
Brain Death: Cortical Death vs Brainstem Death
Provided image
With the advent of mechanical ventilation in the 1950s and 1960s, medicine confronted a new category of death: patients whose hearts continued to beat and whose lungs were being ventilated by a machine, but whose brains had been irreversibly destroyed. This clinical reality required a new legal and medical definition. Brain death is defined as the irreversible cessation of all functions of the entire brain, including the brainstem. It is now recognised as legal death in most countries, including India (under The Transplantation of Human Organs Act 1994 and its 2011 amendment, THOTA — see fp5).
A critical distinction — one that is frequently confused and has profound legal consequences — is between cortical death and brainstem death. Understanding this difference is essential because the two conditions have completely different prognoses, clinical presentations, and legal statuses.
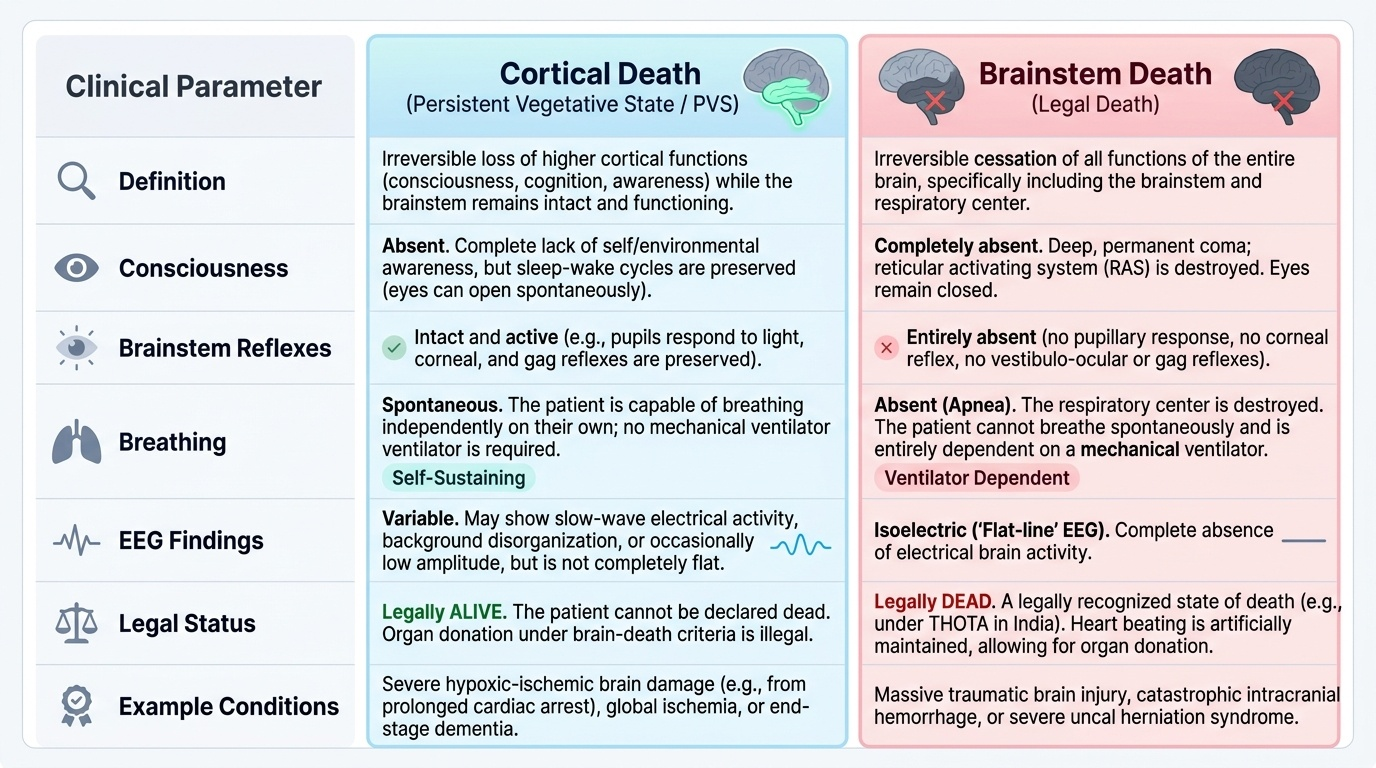
Cortical death (also called persistent vegetative state, PVS) describes the permanent loss of higher cortical functions — consciousness, cognition, purposeful movement, and awareness — while the brainstem remains intact. The brainstem continues to regulate breathing, heart rate, sleep-wake cycles, and reflexes. A patient in PVS can breathe spontaneously, may open their eyes spontaneously (but without awareness), and will maintain a regular heartbeat. They are alive — they are NOT brain-dead. PVS is not a form of brain death, and a patient in PVS cannot be declared legally dead or considered for organ donation under brain-death criteria. (This distinction is life-or-death — a number of tragic misidentifications have occurred globally.)
Brainstem death, by contrast, is the irreversible cessation of all brainstem functions — including the respiratory centre, the reticular activating system (consciousness), and all brainstem reflexes. Without mechanical ventilation, the patient would have no respiratory effort whatsoever. The criteria for diagnosing brainstem death (per Reddy's FM&T and Indian THOTA guidelines) are:
1. Known irreversible structural cause of brain damage (e.g. severe head injury, intracranial haemorrhage)
2. Exclusion of reversible causes: hypothermia (core temp must be >35°C), drug effects (sedatives, neuromuscular blocking agents), metabolic derangements
3. Absent brainstem reflexes: pupillary light reflex (pupils fixed, dilated), corneal reflex, oculocephalic reflex (doll's eye), vestibulo-ocular reflex (caloric test), gag reflex, cough reflex
4. Apnoea test: disconnect from ventilator; pre-oxygenate; observe for 10 minutes. Brain death is confirmed if there is no respiratory effort when PaCO2 rises to ≥60 mmHg
5. Two independent doctors must certify (one must be a specialist — neurologist, neurosurgeon, or intensivist); tests are repeated after an appropriate interval
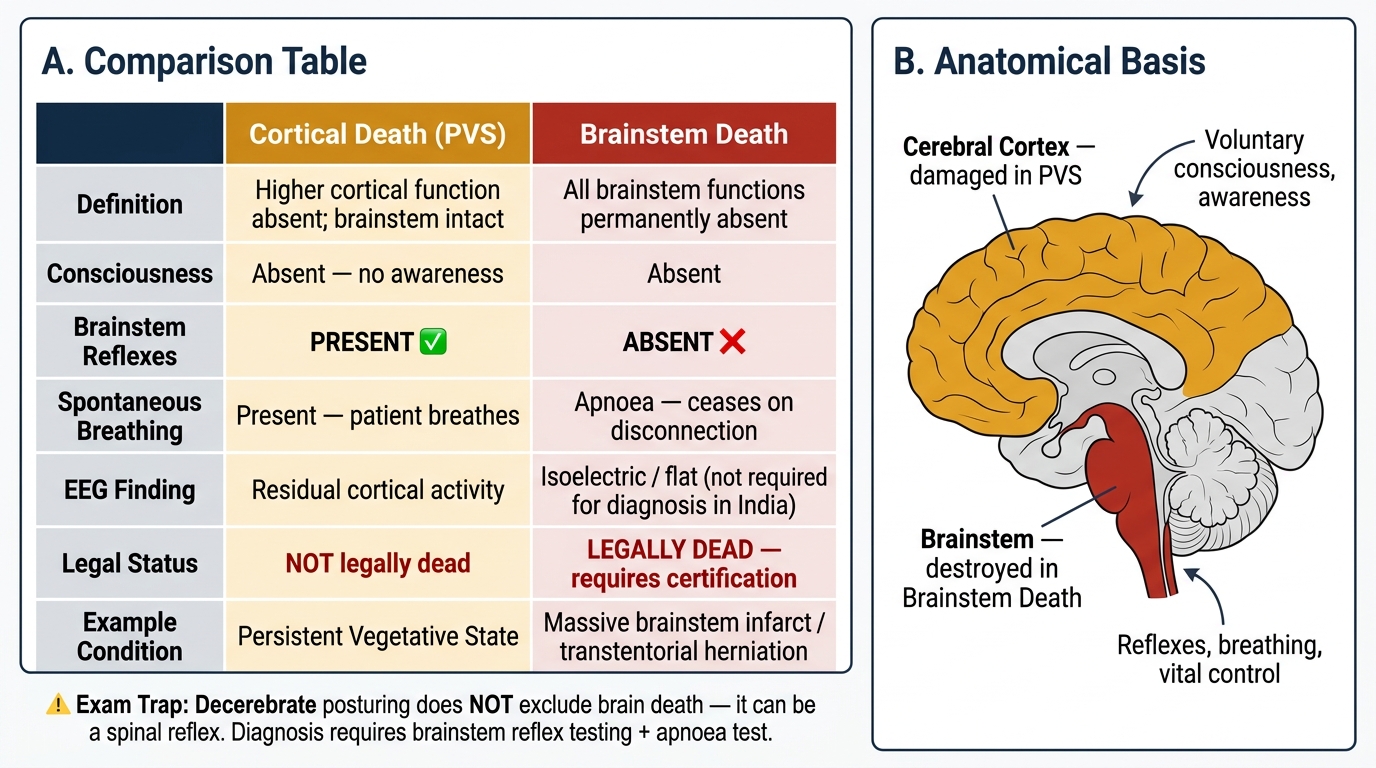
Cortical Death (PVS) vs Brainstem Death — Diagnostic Criteria and Legal Status
- Cortical death (PVS): intact brainstem, spontaneous breathing, NOT brain death, NOT legally dead
- Brainstem death: no brainstem reflexes, apnoea on disconnection, legally dead (with certification)
- EEG: in PVS shows residual cortical activity; in brainstem death may show isoelectric (flat) tracing — but EEG is NOT required for brainstem death diagnosis in India
- Common exam trap: 'decerebrate posturing' still present does NOT exclude brain death (it can be a spinal reflex); what matters is brainstem reflex testing and apnoea test
Modes of Death: Coma, Asphyxia, and Syncope
The modes of death describe the immediate physiological mechanism by which vital functions cease — the final common pathway through which the body transitions from life to death, regardless of the underlying cause. The classical three-mode classification was proposed by Marie François Xavier Bichat (1771-1802), who observed that all death ultimately proceeds through failure of one or more of three vital systems: the brain (nervous system), the respiratory system, or the cardiovascular system. Forensic pathologists use this framework to describe how a person died, distinct from why (the cause of death, which is what the MCCD addresses).
Coma as a mode of death refers to progressive, irreversible loss of consciousness due to failure of cerebral function, leading ultimately to failure of all other vital centres. The brain is the primary organ failing. Coma can result from head injury, intracranial haemorrhage, metabolic encephalopathy (uraemia, hepatic failure, hypoglycaemia), drug toxicity, or any other cause of diffuse cortical or brainstem suppression. In forensic practice, coma as a mode of death is documented when cerebral failure is the initiating event and the primary determinant of the terminal sequence, with respiratory and cardiac failure occurring secondarily as brainstem regulation is progressively lost.
Asphyxia as a mode of death refers to death resulting from oxygen deprivation to the tissues, with consequent accumulation of carbon dioxide. The respiratory system is the primary organ failing. Asphyxia can be mechanical (smothering, strangulation, drowning, aspiration) or non-mechanical (CO poisoning, altitude, respiratory failure from pneumonia or neuromuscular disease). The sequence in asphyxia follows a characteristic pattern: initial hypoxic stimulation of the respiratory centre → increased respiratory effort → progressive hypoxia → cerebral depression → convulsions → final apnoea → cardiac arrest. In forensic pathology, 'asphyxia' as a mode of death is distinct from 'asphyxiation' as a cause — a victim of manual strangulation died from asphyxia (mode) caused by strangulation (manner).
Syncope as a mode of death refers to sudden cardiac failure — the heart is the primary organ failing, leading to immediate cessation of cerebral perfusion and secondary respiratory failure. Syncope (from Greek: cutting short) as a mode of death occurs in ventricular fibrillation, massive pulmonary embolism, aortic rupture, or any other cause of sudden catastrophic fall in cardiac output. In forensic terms, syncope as a mode of death is the pathway in sudden cardiac death, which has important natural-death classification implications (see fp2).
The practical importance of mode-of-death classification is that it links the physical findings at autopsy to the functional sequence of dying. For example, petechial haemorrhages (Tardieu's spots) in asphyxia, or the absence of such findings in sudden cardiac death (syncope mode), can help the forensic pathologist reconstruct the terminal events.
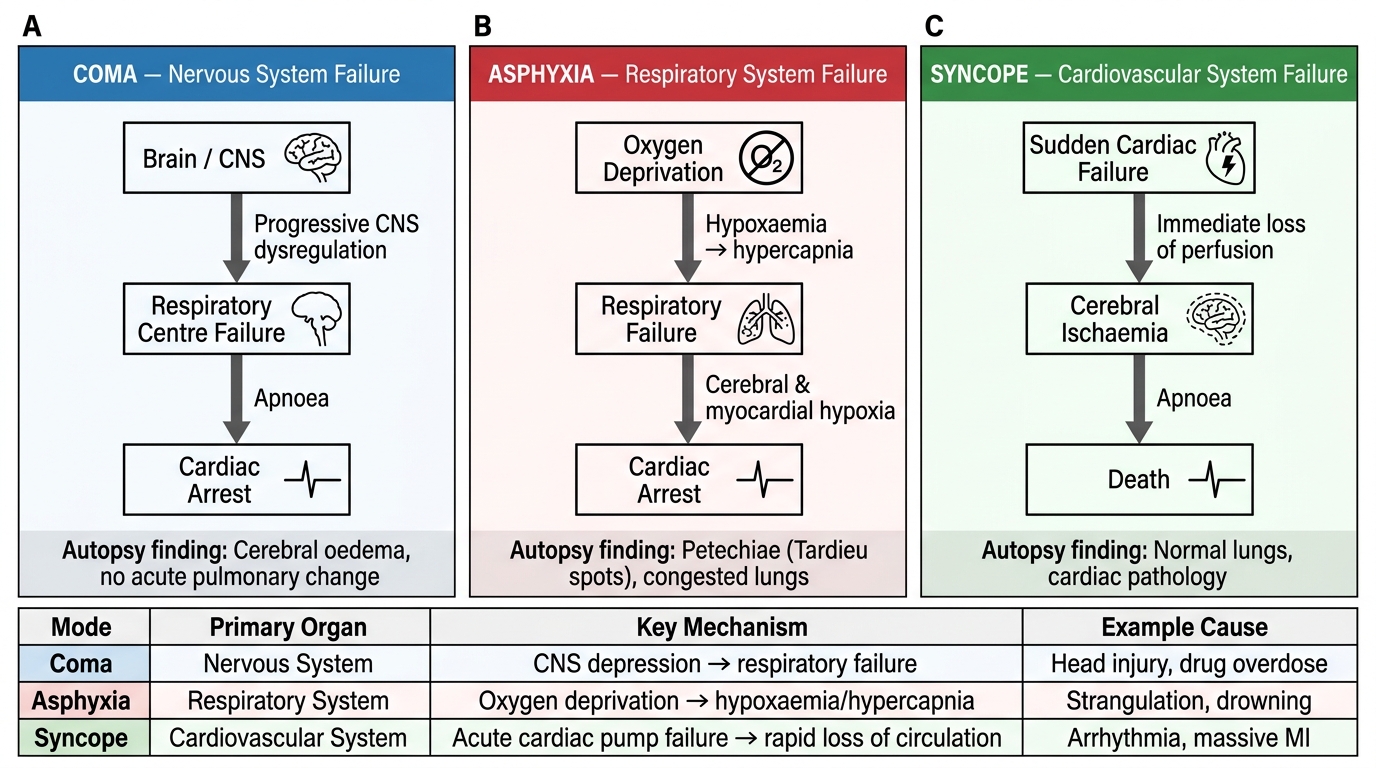
Bichat's Three Modes of Death: Parallel Pathways
| Mode of Death | Primary Organ Failing | Key Mechanism | Example Cause |
|---|---|---|---|
| Coma | Brain (nervous system) | Progressive loss of CNS regulation | Head injury, encephalitis |
| Asphyxia | Respiratory system | Oxygen deprivation, CO2 accumulation | Drowning, strangulation |
| Syncope | Heart (cardiovascular) | Sudden cardiac failure, loss of perfusion | VF, massive PE, aortic rupture |
SELF-CHECK
A 55-year-old man with known ischaemic heart disease is found dead in his chair with no signs of struggle or injury. Autopsy shows a fresh left anterior descending coronary artery occlusion. Which mode of death best describes this case?
A. Coma
B. Asphyxia
C. Syncope
D. Suspended animation
Reveal Answer
Answer: C. Syncope
This is a sudden cardiac death from acute myocardial infarction — the primary organ failing is the heart, leading to sudden cessation of cardiac output and secondary cessation of respiration and brain function. This is the syncope mode of death (primary cardiovascular failure). Coma would apply if the brain were the primary failing organ (e.g. stroke, encephalitis). Asphyxia would apply if the primary failure were respiratory oxygen deprivation. Suspended animation is not a mode of death but a condition resembling death.