Page 2 of 14
FM2.{3,7-8} | Death: Definition, Types & Modes — SDL Guide (Part 2)
Suspended Animation: Recognition and Medicolegal Significance
Suspended animation (Latin: mors apparens, apparent death) is a condition in which the vital signs — pulse, respiration, reflexes — are so profoundly depressed that they are imperceptible to clinical examination, yet the individual is actually alive. It is not a mode of death; it is a state of greatly diminished metabolism in which life is preserved but all signs of life are temporarily absent or undetectable. Suspended animation is critically important in forensic medicine because premature certification of death in a person with suspended animation constitutes a grave professional error and potentially criminal negligence.
The conditions most commonly producing suspended animation are:
- Hypothermia: profound lowering of core body temperature (below ~28°C and especially below 20°C) slows metabolic rate to such a degree that pulse and breathing become imperceptible. There is a well-documented principle in resuscitation medicine: 'a patient is not dead until they are warm and dead' — this reflects the reversibility of hypothermia-induced apparent death
- Drug overdose: barbiturates, opioids, and other CNS depressants can suppress vital signs to an undetectable level; this has historically caused erroneous burial
- Electrocution: a non-lethal electric shock can cause cardiac arrest and apnoea followed by spontaneous recovery; the window between apparent death and resuscitation is brief
- Drowning (submersion): the diving reflex (especially in cold water) can dramatically suppress heart rate and reduce oxygen consumption; infants have been resuscitated after prolonged submersion in cold water
- Catalepsy: a state of rigid immobility with reduced vital signs seen in severe hysteria or certain neurological conditions
- Neonatal apparent death: at birth, some neonates show no respiratory effort and apparent lifelessness that responds to stimulation
The medicolegal significance is profound. Historically, premature burial was a recognised danger (Blundell and other early forensic physicians documented cases). Modern forensic medicine requires that before issuing a death certificate, the certifying doctor must actively exclude suspended animation by:
1. Attempting resuscitation (or confirming it is clearly futile — e.g. decapitation, decomposition)
2. Observing for true signs of death: early signs include cessation of heartbeat and respiration; confirmatory signs include post-mortem lividity, rigor mortis, and temperature changes (covered in fp3)
3. In cases of doubt, observation over time is mandatory — no certificate should be issued until signs of actual death are unambiguous
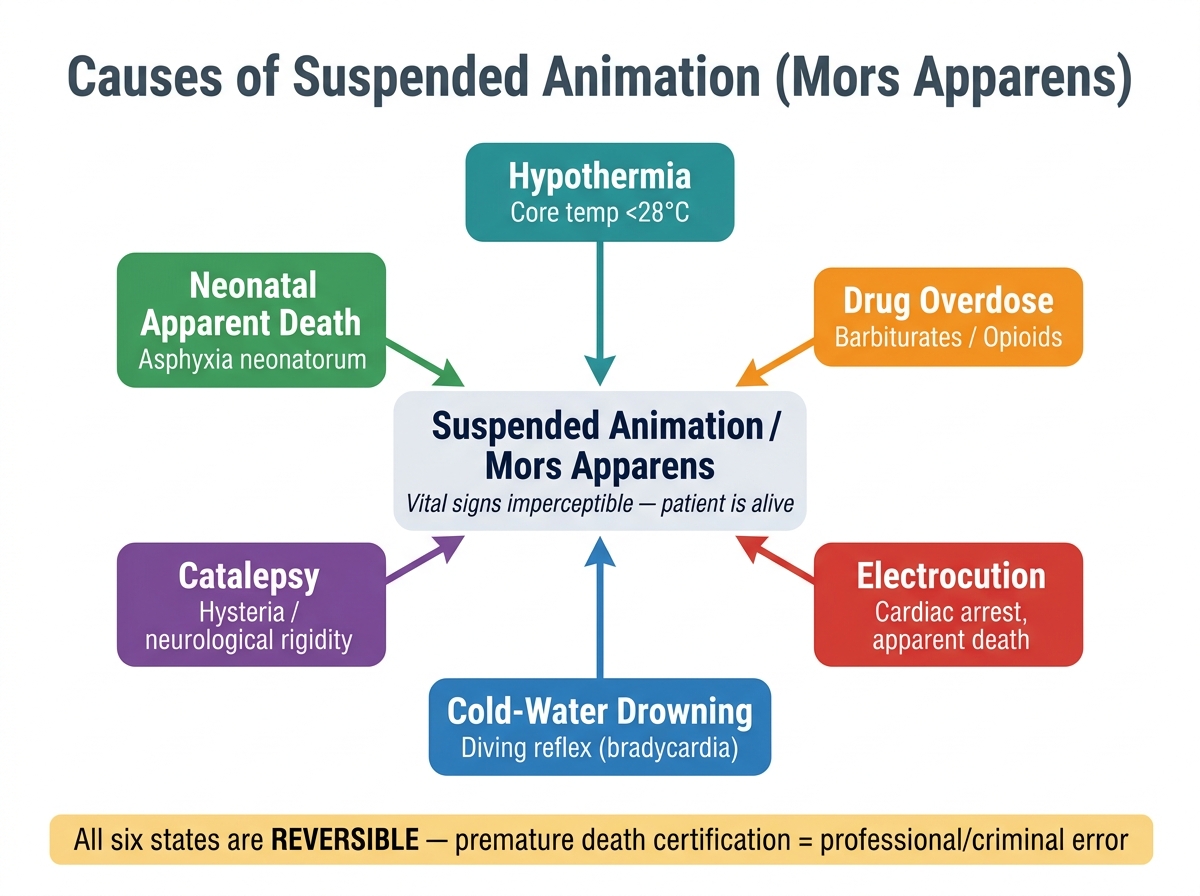
Causes of Suspended Animation (Mors Apparens)
- Suspended animation ≠ mode of death; it is a state that must be excluded before certifying death
- Key causes: hypothermia, drug overdose, electrocution, cold-water drowning, catalepsy
- The forensic rule: issue the death certificate only when post-mortem changes confirm irreversible death
CLINICAL PEARL
The 'warm and dead' rule: A patient with severe hypothermia may have an undetectable pulse and appear dead, yet be fully resuscitable once warmed. Core body temperature must be measured in all apparent deaths found in cold environments. Never certify death in a hypothermic patient until warming has been attempted and the patient remains pulseless at a core temperature above 32-35°C. This rule has saved lives — including documented cases of children submerged in icy water for over 30 minutes who survived neurologically intact. Conversely, attempting resuscitation in a patient with clear post-mortem changes (rigor, lividity, decomposition) is inappropriate and distressing. The forensic physician's task is to distinguish these two states with certainty.
Medicolegal Framework: Death Certification and Brain-Death Legislation
The legal recognition of death in India is governed by a combination of statutory provisions and case law that has evolved to address the realities of modern medicine. The central challenge has been integrating the concept of brain death into a legal system originally built around cardiorespiratory death, because brain death enables organ procurement from ventilated patients — an activity of immense therapeutic significance.
The Transplantation of Human Organs and Tissues Act 1994 (THOTA), as amended in 2011, formally defines brain death for legal purposes in India. Under THOTA (Section 2(c)), a person is deemed dead if either: (a) the cardiorespiratory criteria are met (permanent cessation of circulation and respiration), OR (b) brain death criteria are met — specifically, permanent and irreversible cessation of all functions of the brain, including the brainstem. Crucially, under THOTA, brain death can only be certified by a board of four doctors: the doctor in charge of the hospital or their nominee, a registered medical practitioner in charge of the patient, a neurologist or neurosurgeon, and a government-appointed doctor. This four-member board requirement is specific to the organ-transplantation context.
For routine clinical practice (certifying death in a patient who has not been declared brain-dead on a ventilator), the cardiorespiratory definition remains primary. The doctor signing the death certificate (Form 4A in India) certifies the cessation of vital functions on clinical grounds. The MCCD (Medical Certificate of Cause of Death) issued under the Registration of Births and Deaths Act must be completed by the attending physician.
Key medicolegal rules for death certification:
- A death certificate can be signed only by a registered medical practitioner who attended the deceased during the last illness OR examined the body after death
- In cases of sudden, unexpected, or unnatural death, the body must be referred to the police/magistrate and a forensic autopsy may be ordered
- Premature certification is an offence under the IPC (section 304A — causing death by negligence, or potentially sections related to forgery/false documentation)
- Once a death certificate is issued, the body may be disposed of — making the responsibility of the certifying physician absolute
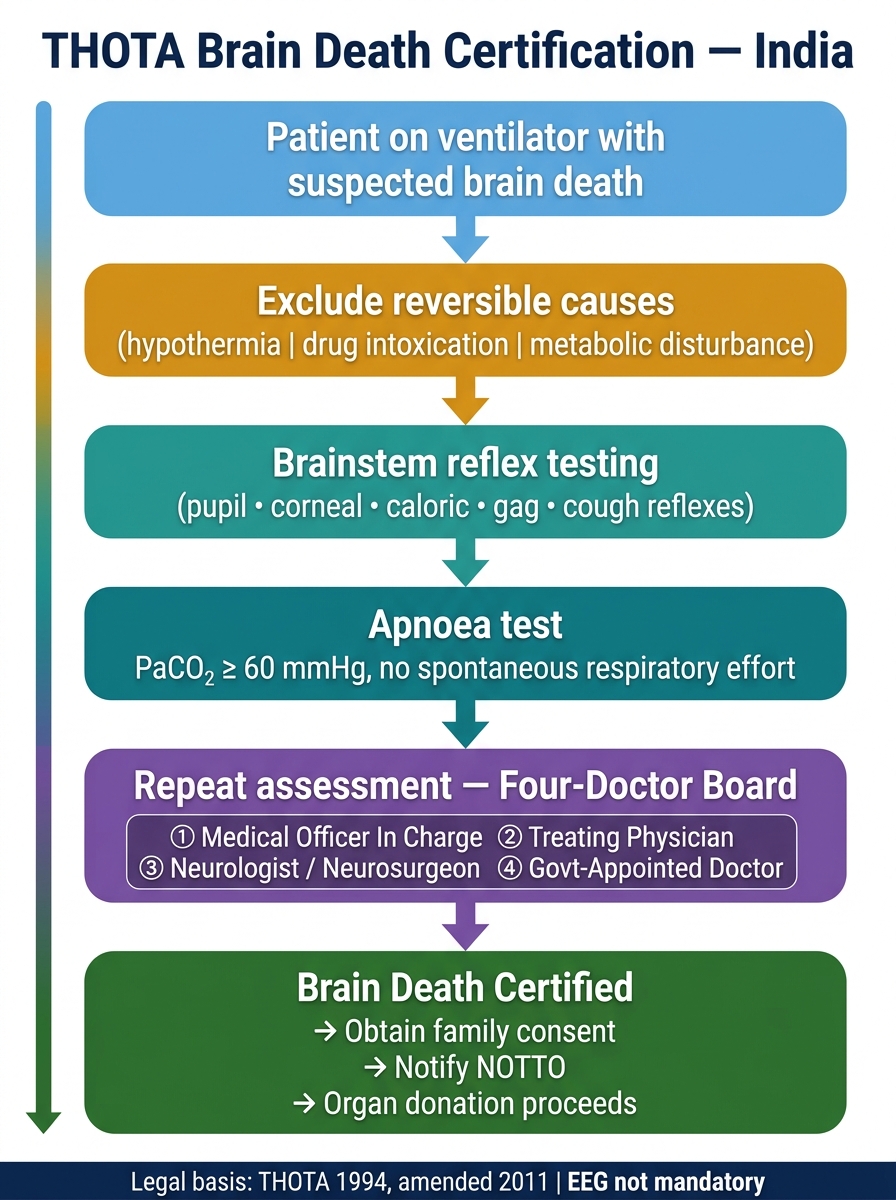
THOTA Brain Death Certification Flowchart (India)
- Brain death definition in India: per THOTA 1994 (amended 2011) — four-doctor board for organ-donation context
- Routine death certification: cardiorespiratory criteria, attended physician signs MCCD
- Suspended animation must be excluded before any certificate is issued
SELF-CHECK
Under the Transplantation of Human Organs and Tissues Act (THOTA) 1994 as amended in 2011, which of the following is correct regarding brain death certification for organ donation purposes?
A. One neurologist alone can certify brain death
B. Brain death requires certification by a board of four doctors including a neurologist or neurosurgeon
C. Brain death can only be certified 24 hours after the initiating event
D. EEG showing isoelectric tracing is mandatory before brain death certification in India
Reveal Answer
Answer: B. Brain death requires certification by a board of four doctors including a neurologist or neurosurgeon
Under THOTA 1994 (as amended 2011), brain death for the purpose of organ donation must be certified by a board of four doctors: the medical officer in charge of the hospital (or their nominee), the doctor in charge of the case, a neurologist or neurosurgeon, and a government-appointed doctor. One doctor alone cannot certify brain death. There is no mandatory 24-hour waiting period specified in the Act, though repeated testing at an appropriate interval is required. EEG is NOT mandatory for brainstem death diagnosis in India — the clinical criteria (brainstem reflex testing + apnoea test) are the standard.