Page 1 of 16
FM11.1-2 | Mental Illness: Classification & Symptomatology — SDL Guide
Learning Objectives
- Classify common mental illnesses including PTSD using ICD-11 categories
- Define and distinguish hallucinations, illusions, delusions, obsessions, and lucid interval with clinical examples
- Explain the medicolegal significance of mental illness classification and lucid interval in forensic practice
INSTRUCTIONS
Forensic medicine demands a working knowledge of mental illness beyond basic clinical psychiatry. In courts, jails, and medicolegal examinations, a forensic physician must be able to classify a patient's mental state, document specific symptoms with forensic precision, and translate that assessment into legally meaningful language. This module builds the classification and symptom vocabulary that underpins every forensic psychiatric evaluation — from will contests to criminal responsibility determinations.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old man is produced before a Sessions Court charged with theft. His lawyer files an application claiming the accused suffers from a mental illness and requests a medical board examination to determine fitness to stand trial. The magistrate orders you — as the court-appointed forensic physician — to conduct a psychiatric examination and submit a written opinion. As you begin your evaluation, the accused stares at the ceiling, laughs without cause, and mutters responses to voices you cannot hear. How do you systematically classify what you are observing, and what specific symptoms must you document to make your medicolegal opinion court-admissible?
WHY THIS MATTERS
Mental illness is encountered in every domain of forensic practice: criminal responsibility, testamentary capacity, fitness to plead, civil competency, and custody disputes. A forensic physician who cannot distinguish a hallucination from an illusion, or a delusion from an obsession, risks producing an opinion that is scientifically indefensible and legally unusable. Understanding the international classification systems and the precise symptomatological vocabulary is therefore not academic — it is the foundation of every court-admissible psychiatric opinion you will ever write. The terms you learn in this module will appear in police interrogation reports, court orders, and legal textbooks throughout your career.
RECALL
Before proceeding, recall from your Year-1 Physiology that the cerebral cortex mediates perception and higher cognitive functions. Psychotic symptoms arise when normal filtering and integration of sensory inputs breaks down — the brain generates percepts without genuine external stimuli or forms beliefs that cannot be corrected by evidence. From Year-1 Psychology/Psychiatry basics, recall that the mental status examination (MSE) is the structured clinical tool for documenting a patient's appearance, behaviour, speech, mood, affect, thought content, thought form, perceptions, cognition, insight, and judgment. This SDL focuses on the classification of illnesses (the big-picture diagnostic categories) and the specific symptom terms within them.
Overview of Mental Illness Classification Systems
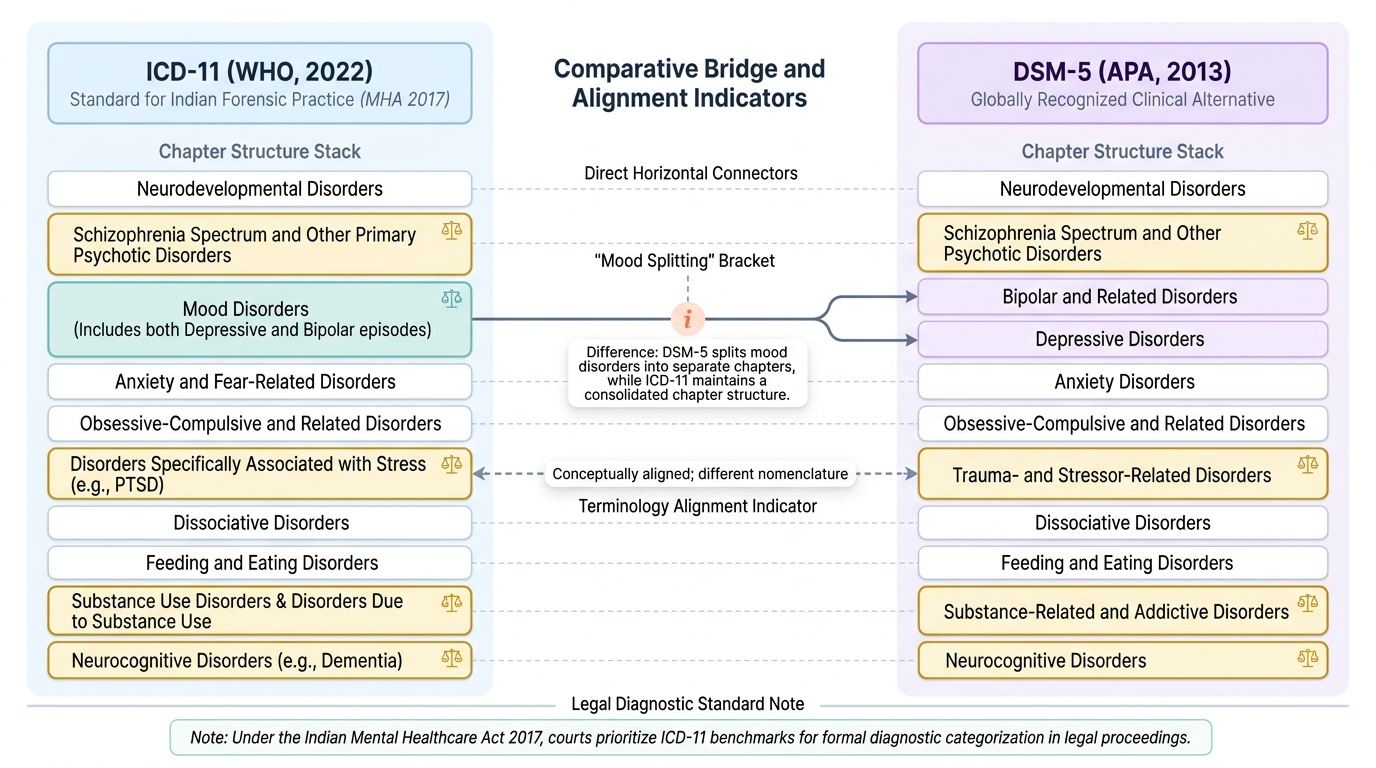
When a forensic physician is asked to provide an opinion on the mental state of an accused or a testator, the opinion must be grounded in a recognised international classification system — not informal or colloquial language. Two systems dominate global and Indian forensic psychiatric practice: the International Classification of Diseases, 11th revision (ICD-11), published by the World Health Organization in 2022, and the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), published by the American Psychiatric Association in 2013. Indian courts and the Mental Healthcare Act 2017 (the operative Indian statute) reference international classification systems, and most Indian forensic reports use ICD-11 terminology. These systems provide operationally defined diagnostic criteria: specific symptom types, minimum duration requirements, and exclusion criteria that ensure two clinicians examining the same patient reach the same diagnostic category.
The value of using a standardised classification system in forensic work extends beyond clinical accuracy. A court-admissible psychiatric opinion must withstand cross-examination by opposing counsel. When your report states that the accused "meets ICD-11 criteria for a schizophrenia spectrum disorder," you are anchoring your opinion to an internationally recognised, peer-reviewed standard — not personal clinical intuition. This transforms the opinion from an individual assertion into a reproducible, verifiable finding, exactly what courts require from expert witnesses.
The two systems are broadly compatible but use different chapter structures. ICD-11 organises mental disorders into blocks such as Neurodevelopmental Disorders, Schizophrenia Spectrum and Other Primary Psychotic Disorders, Mood Disorders, Anxiety and Fear-Related Disorders, Obsessive-Compulsive and Related Disorders, Disorders Specifically Associated with Stress (where PTSD lives), Dissociative Disorders, Feeding and Eating Disorders, Substance Use Disorders, Disorders Due to Substance Use, and Neurocognitive Disorders. DSM-5 uses similar but non-identical chapter boundaries. For routine Indian forensic practice, familiarity with the ICD-11 block names and their key forensically relevant disorders is the minimum required standard.
Provided image
Common Mental Illnesses — ICD-11 Categories and PTSD
The scientific basis for classifying mental illness rests on clusters of symptoms that have predictable onset patterns, family aggregation, neurobiological correlates, and — critically for forensic purposes — distinct behavioural implications. Understanding the major ICD-11 categories equips the forensic physician to recognise which diagnosis is most likely and what legal consequences flow from it.
Provided image
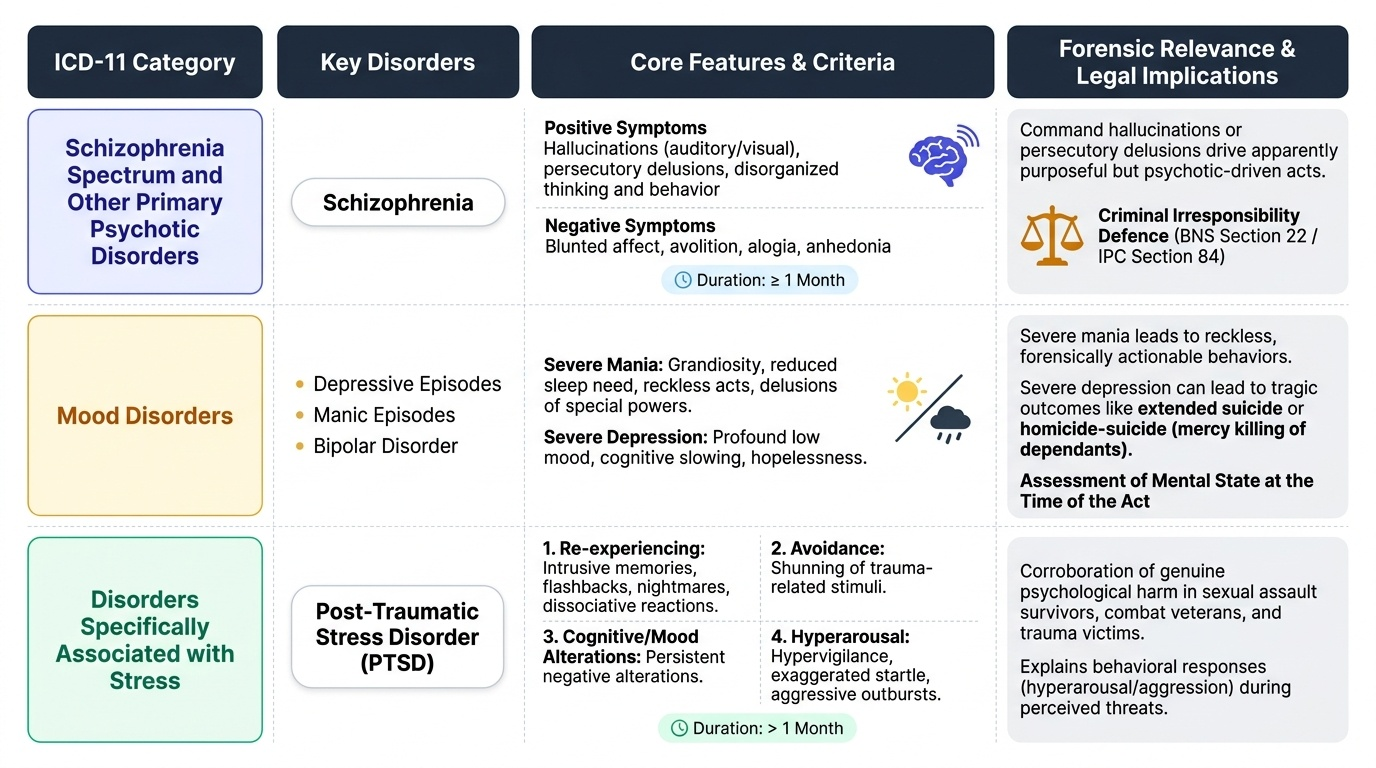
Schizophrenia Spectrum and Other Primary Psychotic Disorders is the category most frequently encountered in criminal responsibility assessments. Schizophrenia itself is characterised by positive symptoms (hallucinations, delusions, disorganised thinking and behaviour) and negative symptoms (blunted affect, avolition, alogia, anhedonia). ICD-11 requires that symptoms are present for at least one month. The forensic significance is profound: a person experiencing command auditory hallucinations or persecutory delusions may commit acts that appear purposeful to observers but are driven entirely by psychotic experience, creating a genuine basis for the criminal irresponsibility defence (BNS Section 22, formerly IPC Section 84).
Mood Disorders encompass depressive episodes, manic episodes, and bipolar disorder. Severe mania with psychotic features — grandiosity, reduced need for sleep, reckless acts, sometimes with delusions of special powers — is directly forensically relevant. Severe depression can lead to extended suicide or homicide-suicide ("mercy killing" of dependants), raising medicolegal questions about mental state at the time of the act.
Disorders Specifically Associated with Stress is the ICD-11 block that includes Post-Traumatic Stress Disorder (PTSD), a diagnosis of enormous forensic importance. PTSD follows exposure to a traumatic event and is characterised by: (1) re-experiencing symptoms (intrusive memories, nightmares, flashbacks, dissociative reactions — the person acts or feels as if the traumatic event is recurring), (2) avoidance of trauma-related stimuli, (3) persistent negative alterations in cognition and mood, and (4) marked alterations in arousal and reactivity (hypervigilance, exaggerated startle, aggressive outbursts). Symptoms must persist for more than one month. Forensically, PTSD is relevant in sexual assault survivors (it corroborates the genuineness of psychological harm), combat veterans charged with violent offences (diminished responsibility), and as a cause of functional disability in injury compensation claims. Notably, ICD-11 has moved PTSD OUT of the Anxiety Disorders chapter (its old ICD-10 location) into a distinct stress-related block — a nuance that matters when citing classification in court.
Obsessive-Compulsive and Related Disorders includes OCD and body dysmorphic disorder. Anxiety and Fear-Related Disorders includes panic disorder, generalised anxiety disorder, and phobias. Neurocognitive Disorders (dementia, delirium, traumatic brain injury sequelae) are highly relevant in testamentary capacity assessments. Substance Use Disorders and substance-induced disorders (intoxication, withdrawal, including Delirium Tremens — covered in SDL fpsy3) are critical in toxicology-related forensic cases.
SELF-CHECK
Under ICD-11, which chapter block contains Post-Traumatic Stress Disorder (PTSD)?
A. Anxiety and Fear-Related Disorders
B. Disorders Specifically Associated with Stress
C. Schizophrenia Spectrum and Other Primary Psychotic Disorders
D. Dissociative Disorders
Reveal Answer
Answer: B. Disorders Specifically Associated with Stress
ICD-11 moved PTSD from the Anxiety Disorders chapter (its ICD-10 position) into a distinct block called 'Disorders Specifically Associated with Stress,' which also includes Acute Stress Reaction and Adjustment Disorder. This is forensically significant because citing the correct ICD-11 chapter demonstrates up-to-date classification knowledge under cross-examination.
Perceptual Disturbances: Hallucinations and Illusions
Perceptual disturbances are among the most dramatic and forensically significant symptoms in psychiatric practice. The forensic physician documenting perceptual disturbances must capture not merely their presence but their sensory modality, content, and the patient's attribution and response to them — because these details directly inform the legal assessment of the patient's mental state at the time of the alleged act.
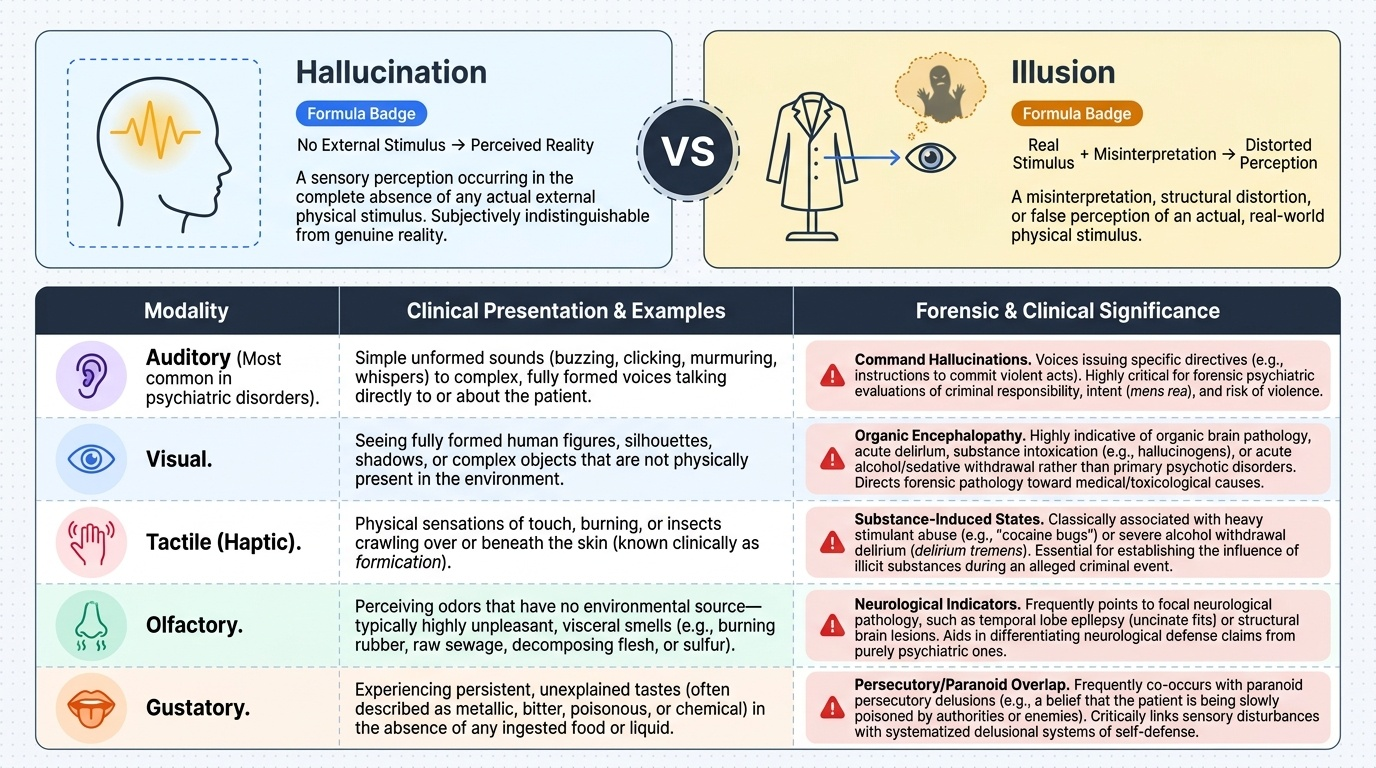
A hallucination is a perception that occurs in the absence of any real external stimulus. The defining feature is that the percept feels real to the patient — it has the full force and impact of a genuine sensory experience. Hallucinations are classified by sensory modality:
- Auditory hallucinations are the most common in psychotic disorders. They range from simple sounds (buzzing, clicking) to formed voices. Particularly important forensically are command auditory hallucinations — voices instructing the patient to perform specific acts, including acts of violence. If a patient reports that a voice commanded them to attack a person, this is directly relevant to criminal responsibility.
- Visual hallucinations — seeing formed figures, shadows, or objects that are not present — are more common in organic conditions (delirium, substance intoxication, withdrawal) than in primary psychotic disorders, where they are less prevalent than auditory hallucinations.
- Tactile (haptic) hallucinations — sensations of being touched, insects crawling on the skin (formication, common in cocaine and alcohol withdrawal) — are seen in substance use disorders and delirium.
- Olfactory and gustatory hallucinations — smells and tastes without stimulus — may occur in temporal lobe epilepsy (olfactory aura), severe depression, or schizophrenia.
- Hypnagogic hallucinations (at the onset of sleep) and hypnopompic hallucinations (on waking) are physiological phenomena and do not in themselves indicate mental disorder.
An illusion is fundamentally different from a hallucination: an illusion is a misperception or misinterpretation of a real, existing external stimulus. The stimulus is genuinely present, but the brain processes it incorrectly. A classic example: a grieving person sees a coat hanging on a door and perceives it as a human figure. Illusions are common in states of low lighting, fatigue, heightened arousal, or intoxication, and they are not in themselves indicative of serious mental illness. The medicolegal significance of distinguishing hallucinations from illusions is that hallucinations (especially in the context of a psychotic disorder) can support a mental illness diagnosis and the consequent legal defence, whereas isolated illusions typically do not.
For forensic documentation, the physician must record: which modality, the specific content of the hallucination, whether it is ego-syntonic (the patient accepts and acts on it) or ego-dystonic (the patient resists or is distressed by it), and whether the patient has any insight into the unreality of the experience.
Provided image