Page 2 of 16
FM11.1-2 | Mental Illness: Classification & Symptomatology — SDL Guide (Part 2)
Thought Disturbances: Delusions and Obsessions
Thought disturbances represent disruptions in the content or form of thinking. In forensic psychiatry, disturbances of thought content — particularly delusions and obsessions — are of primary importance because they shape the patient's perception of reality and can directly drive violent or illegal behaviour.
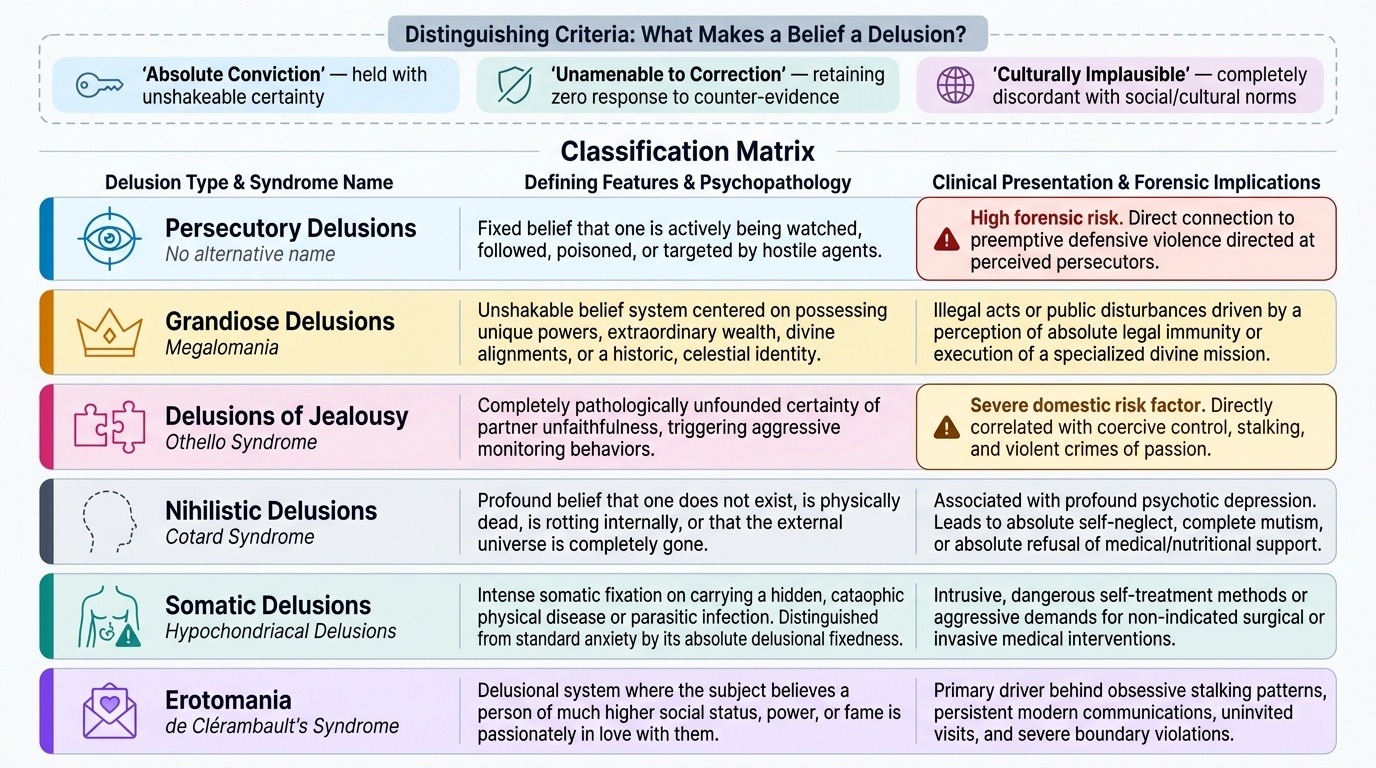
A delusion is a fixed, false, unshakeable belief that is out of keeping with the patient's cultural background, social background, and level of education, and that is maintained despite evidence to the contrary and despite reasonable attempts to reason with the patient. Three distinguishing features make a belief a delusion rather than merely an unusual opinion: it is (1) held with absolute conviction, (2) not amenable to correction by argument or evidence, and (3) culturally implausible. Delusions are classified by their content:
- Persecutory delusions (the most common type): belief that one is being watched, followed, poisoned, persecuted, or plotted against. Directly relevant to assaults on the alleged persecutor.
- Grandiose delusions: belief in special powers, identity (believing oneself to be a prophet, a historical figure, or to have a divine mission). Relevant to situations where the accused believed they had divine authority to perform an act.
- Delusions of jealousy (Othello syndrome): pathological jealousy — the fixed, false belief that one's partner is being unfaithful. A major forensic risk factor for intimate-partner violence and homicide.
- Nihilistic delusions (Cotard syndrome): belief that one is dead, that body parts are absent, or that the world does not exist. Associated with severe depression.
- Somatic/hypochondriacal delusions: belief of having a serious illness despite medical reassurance. Distinct from ordinary health anxiety by their fixed, unshakeable quality.
- Erotomania (de Clérambault's syndrome): fixed belief that a specific person — usually of higher social status — is in love with the patient. Relevant to stalking behaviour.
- Delusions of reference: belief that neutral events (news broadcasts, strangers' conversations) are specifically directed at or about the patient.
An overvalued idea must be distinguished from a delusion: it is a strongly held, abnormal belief that is not held with the absolute conviction of a delusion and is understandable in the context of the person's past experiences. It lies on a spectrum between a normal strongly-held belief and a true delusion.
An obsession is a repetitive, intrusive, unwanted thought, impulse, or mental image that enters the mind involuntarily and is recognised by the patient as their own (unlike a thought insertion in psychosis). The critical distinguishing feature is that the obsession is ego-dystonic — the patient recognises it as absurd or inappropriate, finds it repugnant, and attempts to suppress or neutralise it (often through compulsive acts). Common obsessional content includes themes of contamination, doubt ("did I lock the door?"), aggression, and sexual or religious content. The patient suffering from OCD does not want to act on the obsession and is distressed by it — this distinguishes obsessions from psychotic thought content where ego-syntonic beliefs drive behaviour.
Forensically, the distinction between obsession and delusion is important: a man who presents after an assault who describes persistent thoughts of harming his wife — which he finds repugnant and has never acted on — is describing an obsessional phenomenon, not a delusion. The forensic prognosis and legal implications are entirely different.
Provided image
SELF-CHECK
A patient describes a fixed belief that his neighbour is poisoning his food, which he maintains despite his wife showing him the unopened, factory-sealed food packets. He refuses to eat anything prepared at home. Which symptom best describes this?
A. Obsession
B. Overvalued idea
C. Persecutory delusion
D. Tactile hallucination
Reveal Answer
Answer: C. Persecutory delusion
This is a persecutory delusion — a fixed, false, unshakeable belief that he is being poisoned, maintained despite clear evidence to the contrary (sealed packets) and despite his wife's reasonable attempts to correct it. The key triad: absolute conviction + unamendable by evidence + culturally implausible. An obsession would be ego-dystonic (the patient would recognise it as irrational and resist it). An overvalued idea lacks absolute conviction.
Lucid Interval — Definition and Medicolegal Significance
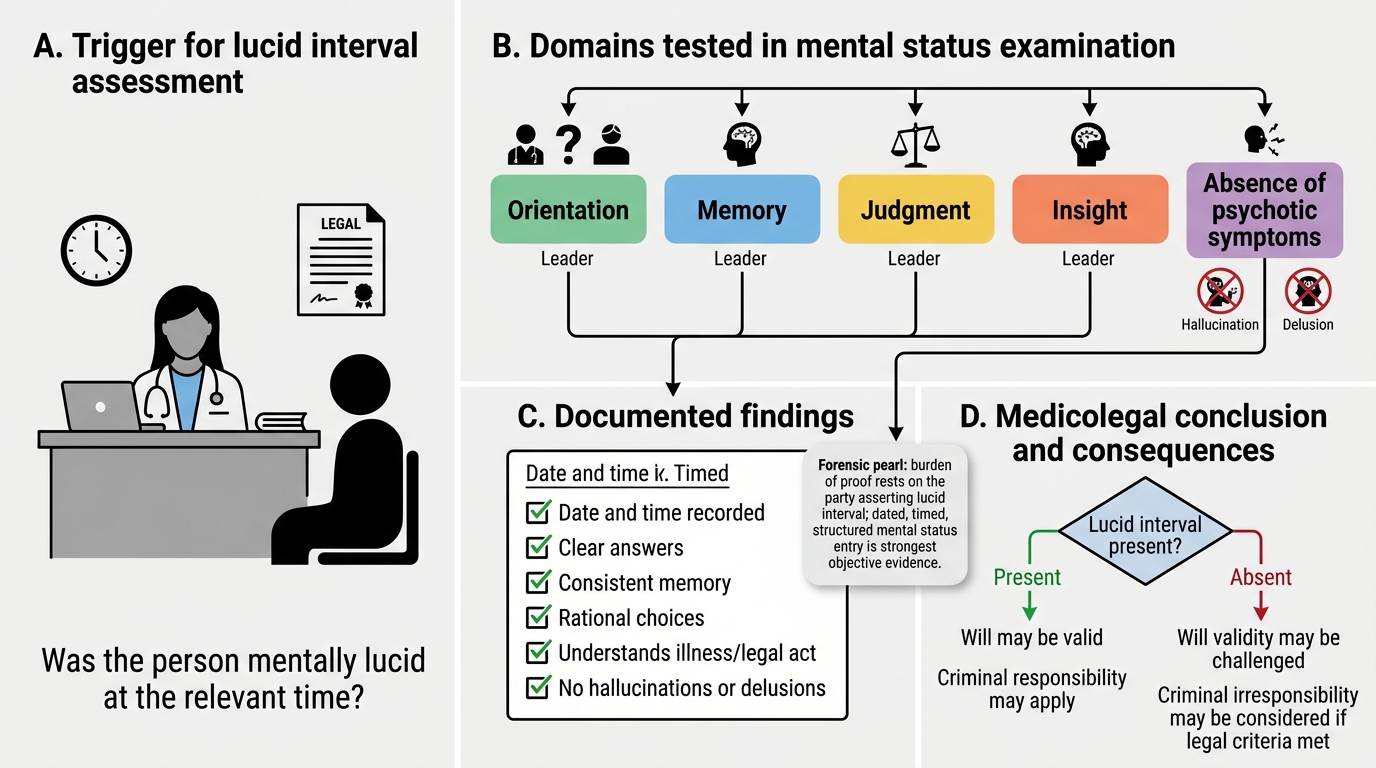
The lucid interval is a period during which a person, otherwise suffering from a mental disorder, temporarily regains their normal mental faculties and is of sound mind. During the lucid interval, the individual has full awareness of their actions, understands the nature and consequences of their decisions, and has intact judgment. The person is — for that period — legally and clinically sane, even though the underlying mental disorder persists.
The concept of the lucid interval is a cornerstone of forensic psychiatric documentation and must be assessed and recorded explicitly in any medicolegal psychiatric evaluation. The clinical examination for a lucid interval involves: testing orientation (person, place, time), assessing short- and long-term memory, evaluating judgment and insight, testing abstract reasoning, and determining whether the patient understands the nature and consequences of their actions at the specific time in question.
The medicolegal significance of the lucid interval operates across several domains:
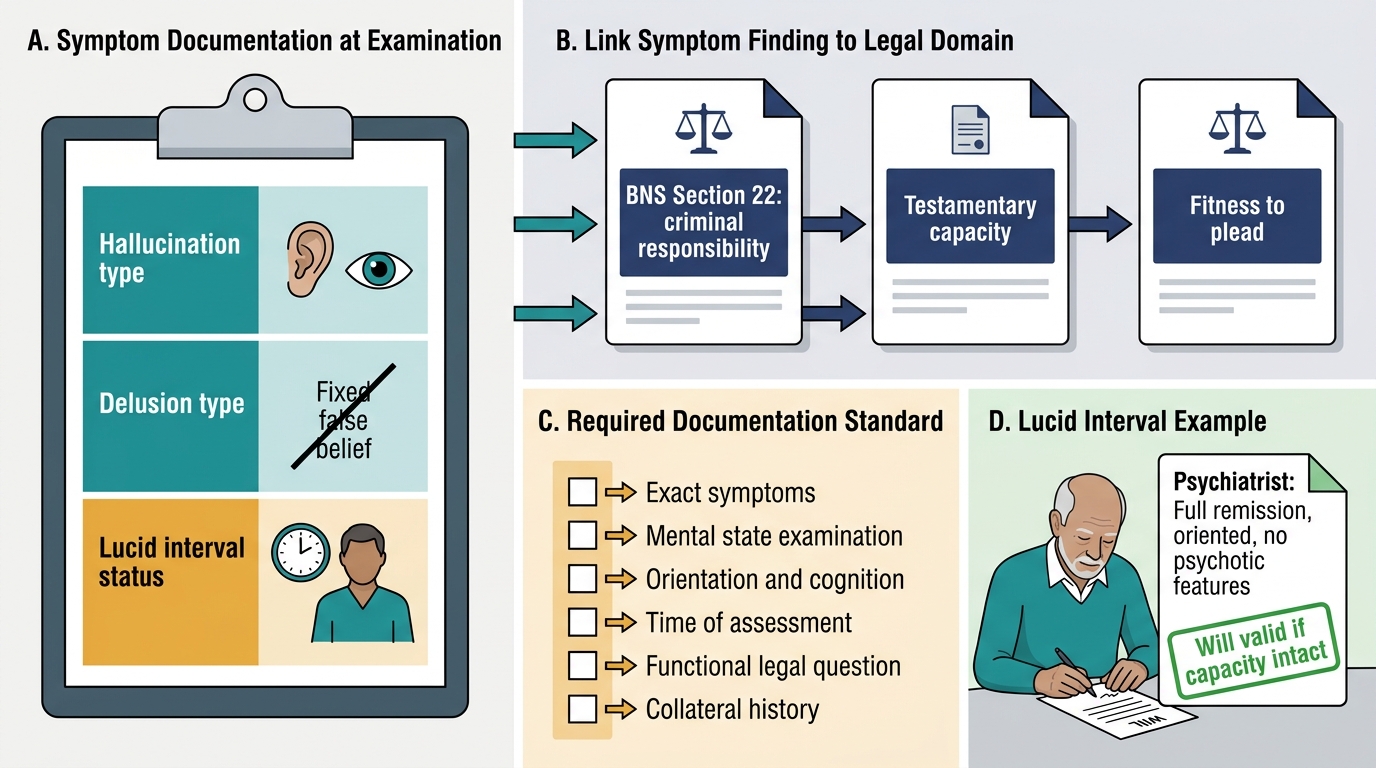
Testamentary capacity (will-making): A will made by a person with a mental disorder is valid if it was executed during a lucid interval. Under the Indian Succession Act, testamentary capacity requires that the testator understand the nature of the act of making a will, the extent of the property being disposed of, the claims of potential beneficiaries, and that no delusion influences the will. A will executed during an acute psychotic episode — when no lucid interval exists — may be challenged as void. The forensic physician asked to opine on will validity must reconstruct, from medical records, witness accounts, and available clinical data, whether the testator was in a lucid interval at the time of execution.
Criminal responsibility: An accused person who commits a criminal act during a lucid interval is fully criminally responsible, even if they have a mental illness. BNS Section 22 (formerly IPC Section 84) provides a complete defence only if the accused was, at the time of the act, by reason of unsoundness of mind, incapable of knowing the nature of the act or that it was wrong. If the act was committed during a lucid interval — when the accused had full cognitive capacity — the defence is not available.
Civil responsibility: Contracts entered into during a lucid interval by a person with a mental disorder are valid under Indian contract law. A person with intermittent mental illness can give valid evidence in court during a lucid interval.
Documenting a lucid interval in clinical notes requires recording the exact date, time, duration of observation, specific cognitive functions tested, and the examiner's assessment of the presence or absence of psychotic symptoms at that moment. Vague or undated entries are not useful in court.
Forensic Assessment of Lucid Interval
CLINICAL PEARL
Three forensically decisive distinctions to internalise:
- Hallucination vs illusion: A hallucination requires no real external stimulus — the percept arises entirely within the mind. An illusion requires a real stimulus that is misinterpreted. Only hallucinations in the context of an established mental illness reliably support criminal irresponsibility or mental illness certification.
- Delusion vs obsession: A delusion is ego-syntonic — the patient believes it wholeheartedly and may act on it. An obsession is ego-dystonic — the patient recognises it as alien to their rational mind, is distressed by it, and resists acting on it. A patient describing intrusive violent thoughts who is horrified by them and has never acted is likely obsessional, not psychotic — the prognosis and forensic risk are very different.
- Lucid interval documentation: The burden of proving a lucid interval rests on the party asserting it (e.g. the will's proponents). A forensic physician's dated, timed, structured mental status entry is the only objective evidence courts will accept. Retrospective reconstruction from nursing notes or visitor accounts is second-best. Always document explicitly when a patient appears to be in a lucid interval — it may become medicolegally critical years later.
Forensic Implications of Classification and Symptomatology
Classification and precise symptomatological documentation are not ends in themselves — they serve a specific function within the medicolegal inference chain. A forensic physician who correctly classifies a patient's disorder and documents its symptoms accurately has provided the court with a scientifically defensible foundation for legal determinations. Understanding how each piece connects to the applicable legal framework is essential for writing a court-admissible opinion.
Criminal responsibility under BNS Section 22: The key legal question is not whether the accused has a mental illness, but whether, AT THE TIME OF THE ACT, the mental illness rendered them incapable of knowing the nature of the act OR incapable of knowing that the act was wrong. This is the McNaughten standard (see SDL fpsy2 for detailed discussion). Classification evidence must therefore be linked to the specific symptom state at the time of the act. Documenting that the accused was experiencing command auditory hallucinations instructing him to attack the victim, or was in the grip of a paranoid delusion that the victim was about to kill him, directly supports the McNaughten criteria. A diagnosis alone — "the accused has schizophrenia" — without symptom documentation at the time of the act is legally insufficient.
Mental Healthcare Act 2017: Section 2(s) of the Mental Healthcare Act 2017 defines "mental illness" as a substantial disorder of thinking, mood, perception, orientation, or memory that grossly impairs judgment, behaviour, capacity to recognise reality, or ability to meet the ordinary demands of life. The use of ICD-11 classification terms in a forensic report aligns with this statutory definition, because the specified domains (thinking, mood, perception) correspond to the specific symptom categories defined above.
Expert witness obligations: As a forensic physician providing expert testimony on mental state, you are required under Indian Evidence Act principles to base your opinion on observed facts (symptoms documented during examination), recognised classification systems (ICD-11 or DSM-5), and established psychiatric principles. Opinions based on informal impressions or lay descriptions are inadmissible. The vocabulary of classification — schizophrenia spectrum disorder, PTSD, persecutory delusions, command auditory hallucinations, lucid interval — is the language of your expert opinion, and it must be used precisely.
IPC to BNS transition: The Bharatiya Nyaya Sanhita 2023 (BNS) replaced the Indian Penal Code from 01 July 2024. The insanity defence, previously at IPC Section 84, is now at BNS Section 22 with substantively identical wording. Forensic physicians must use the BNS section number in current opinions; citing IPC 84 for cases arising after 01 July 2024 is an error.
Forensic Psychiatry: Symptoms to Legal Outcomes
SELF-CHECK
A will was executed by a 70-year-old man with a known diagnosis of bipolar disorder. His treating psychiatrist confirms that he was in full remission, oriented, and without psychotic features at the time of signing. What is the most likely legal status of the will?
A. The will is void because the testator had a mental illness
B. The will is valid because it was executed during a lucid interval with intact testamentary capacity
C. The will can only be valid if countersigned by a psychiatrist
D. The will requires court approval before it can be probated
Reveal Answer
Answer: B. The will is valid because it was executed during a lucid interval with intact testamentary capacity
A will executed during a lucid interval is legally valid. Full remission in bipolar disorder, with intact orientation, cognition, and no psychotic features at the time of execution, constitutes a lucid interval. The mere presence of a mental illness diagnosis does not void a will — the question is whether testamentary capacity (knowing the nature of the act, extent of property, claims of potential beneficiaries) was intact at the specific moment of execution. A psychiatrist's countersignature is not a legal requirement, although contemporaneous psychiatric assessment is strong evidentiary support.