Page 13 of 20
FM7.2 | Fall from Height & Vehicular Injuries — SDL Guide
Learning Objectives
- Describe the injury patterns of falls from height, classified by landing position and surface
- Explain the biomechanics of vehicular injuries — primary impact, secondary impact, and run-over injuries
- Define Waddell's triad and explain its forensic significance in pedestrian-vehicle collisions
- Describe the forensic significance of the bumper fracture in reconstructing impact height
- Differentiate railway spine (neurological injury) from vertebral fracture and explain its forensic significance
- Explain crush syndrome — its pathophysiology (rhabdomyolysis → myoglobinuria → ATN) and medico-legal significance in disaster victims
- Apply IPC 304A (death by negligence) and the Motor Vehicles Act to vehicular injury cases
INSTRUCTIONS
Road traffic injuries are the leading cause of trauma deaths and a major source of medico-legal work in India. Falls are the second most common mechanism requiring forensic medical investigation. Together, they generate the majority of injury reports, post-mortem examinations, and court testimonies in any district hospital's forensic department. This module teaches you to reconstruct events from injury patterns — where the bumper struck, which way the victim fell, whether the injuries are consistent with the reported history — because that reconstruction is the core of the medico-legal opinion.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At 11 PM, a 42-year-old woman is found in the street. Police report: 'hit and run; vehicle fled the scene.' The body shows abrasions on the right shin at 45 cm height, a transverse fracture of the right tibia and fibula, bruising over the right hip and pelvis, and severe head injuries. The police ask you: what was the approximate height of the striking vehicle's bumper? Was she struck from the front or the side? Was she standing or seated when struck? And could the head injury have been caused by the vehicle, or by hitting the ground? Your medico-legal opinion on these questions determines whether the case is pursued as a road traffic accident under the Motor Vehicles Act or as culpable homicide under IPC 299.
WHY THIS MATTERS
India has one of the world's highest road traffic fatality rates — approximately 150,000 deaths annually. The forensic physician is central to every road traffic death investigation: the injury report determines the IPC section applied (IPC 304A negligence vs IPC 299 culpable homicide), guides accident reconstruction for insurance and legal proceedings, and may determine the criminal liability of the driver. Falls from height constitute a separate major category: whether a fall was accidental, suicidal, or homicidal depends on injury pattern analysis and scene correlation. Crush syndrome from disaster scenarios — building collapses, industrial accidents, railway accidents — requires the physician to diagnose rhabdomyolysis from injury context, guiding both clinical management and forensic investigation. These competencies (FM7.2) are directly tested in MD Forensic Medicine entrance examinations and form the backbone of daily medicolegal casework.
RECALL
From FM7.1 (previous module):
• Regional injury patterns: skull fractures, intracranial haemorrhages, coup/contre-coup, thoracic and abdominal organ injuries — all produced by the mechanisms covered in this module
• Wound types: abrasion, contusion, laceration — the specific patterns of each are essential for vehicular injury interpretation
• IPC 319–321: simple and grievous hurt categories relevant to road traffic injuries
From Year-1 Physiology and Biochemistry:
• Muscle physiology: myoglobin is an intracellular oxygen-storing protein; released massively when muscle cell membranes are disrupted
• Renal physiology: myoglobin is filtered at the glomerulus; at high concentrations it precipitates in the tubules, causing acute tubular necrosis (ATN)
• Creatine kinase (CK): intracellular muscle enzyme; elevated in proportion to muscle injury; >5000 U/L indicates significant rhabdomyolysis
Fall from Height: Injury Mechanisms and Patterns
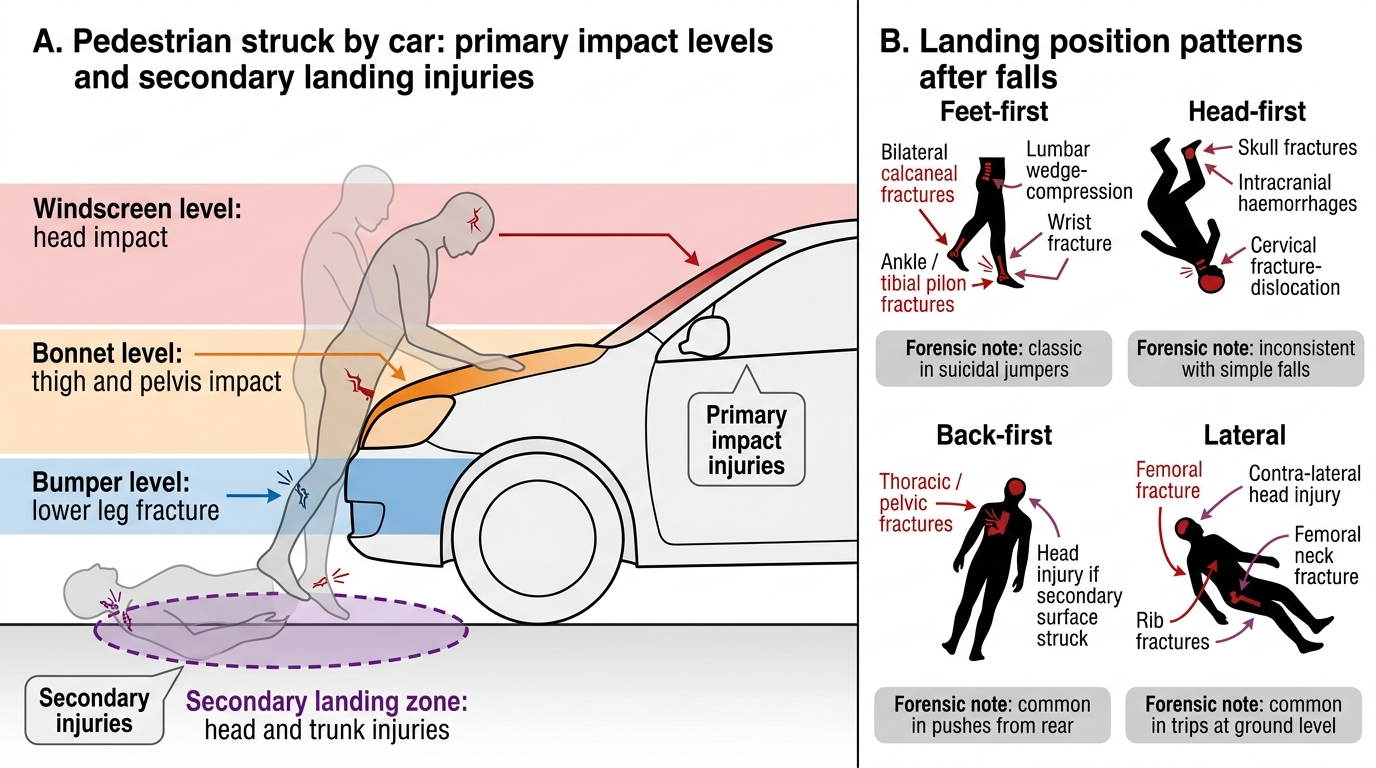
A fall from height is a complex multi-step injury event: the victim accelerates under gravity, strikes an impact surface, and the body decelerates over a very short distance and time. The injuries produced depend on four principal variables: the height of the fall (which determines velocity at impact), the body's landing position (which determines which regions absorb the initial kinetic energy), the surface characteristics (hard concrete vs soft soil; flat vs angular), and any intermediate objects the body strikes on the way down. Understanding these variables allows the forensic physician to reconstruct the circumstances of the fall from the injury pattern — and, critically, to assess whether the injuries are consistent with the reported history.
Feet-first landing is the most common orientation in deliberate jumps from height. The initial impact transmits force upward through the body in sequence: calcaneal (heel bone) fractures are the hallmark — the dense cancellous calcaneum fails first, producing a characteristic compression fracture pattern. Force then travels up through the ankles (pilon/tibial plafond fractures), knees (tibial plateau), lumbar vertebrae (anterior wedge-compression fractures — the classic L1–L2 fractures from axial loading), and thoracic vertebrae. If the height is sufficient, long bone fractures and pelvic ring fractures accumulate. Head injury from secondary rebound (the body tips over after the feet absorb the primary impact) may be relatively minor in short falls but severe in falls >6 metres. Bilateral calcaneal fractures ± lumbar compression fractures ± wrist fractures (from outstretched hands) = the classic feet-first fall triad.
Head-first landing (rare in deliberate jumps; may occur in accidents or homicidal thrown victims) produces massive head injuries — skull fractures, intracranial haemorrhages — as the primary impact, with secondary injuries to the trunk and limbs from the subsequent fall. Cervical spine fracture-dislocation is common.
Lateral or back-first landing distributes impact across a larger body surface — thoracic cage injuries (rib fractures, haemopneumothorax), pelvic injuries, and head injuries depending on head position at landing.
Primary Impact and Secondary Landing Injuries
| Landing Position | Primary Impact Injuries | Secondary Injuries | Forensic Note |
|---|---|---|---|
| Feet-first | Bilateral calcaneal fractures, ankle, tibial pilon | Lumbar wedge-compression, wrist fracture | Classic in suicidal jumpers |
| Head-first | Skull fractures, intracranial haemorrhages | Cervical fracture-dislocation | Inconsistent with simple falls |
| Back-first | Thoracic/pelvic fractures | Head injury (if head hits secondary surface) | Common in pushes from rear |
| Lateral | Hip fracture (femoral neck), rib fractures | Contra-lateral head injury | Common in trips at ground level |
The forensic physician must also consider whether intermediate surfaces were struck — a body falling from the 8th floor and hitting a window ledge at the 4th floor before the ground will show two sets of impact injuries at very different severity levels. The first impact (window ledge) may produce specific patterned injuries consistent with the ledge edge dimensions.
Vehicular Injuries: Primary and Secondary Impact Patterns
Vehicular injuries — particularly pedestrian-vehicle collisions — produce a characteristic, reproducible sequence of injury events that the forensic physician can reconstruct from wound analysis. This reconstruction is the foundation of vehicular accident medico-legal reports and of accident reconstruction evidence in court proceedings.
Primary impact is the initial contact between the vehicle and the victim's body. In a pedestrian struck by a car, the first contact is typically with the bumper, which strikes the lower limbs. The bumper fracture is a transverse fracture of the tibia and/or fibula at the height corresponding to the bumper's contact point on the victim's leg. Measuring this fracture height from the sole of the foot gives the approximate bumper height of the striking vehicle — a forensically significant measurement used to identify the class (sedan, SUV, truck) or potentially the specific make of vehicle. The bumper fracture is most reliable when the victim was standing upright at the time of impact; if the victim was crouching or falling, the fracture height is misleading.
Following the bumper impact, the lower-body momentum is arrested while the upper body continues forward, causing the victim to be thrown over the vehicle's bonnet. Bonnet (hood) injuries are secondary contact injuries at the level of the vehicle's bonnet — producing thigh and pelvic contusions, hip fractures, or abdominal injuries depending on the victim's size and the vehicle's shape. The windscreen may produce further impact injuries to the head or upper trunk as the victim's body continues forward. An imprint of the windscreen glass or the A-pillar (the post beside the windscreen) on the victim's skull can be a key piece of evidence.
Waddell's triad (described for pedestrian-vehicle collisions in adults) describes the three anatomical injury zones: (1) lower limb fracture at bumper level, (2) trunk/pelvic injury from bonnet contact, and (3) head injury from ground impact or windscreen. This triad is a teaching tool — it reminds the physician to look systematically at all three zones — but is not a required 'complete triad' for the collision to be confirmed as a pedestrian impact.
Secondary impact is the victim being thrown from the vehicle and landing on the ground. The ground-contact injuries — typically on the head, shoulder, and hip contralateral to the primary impact — are blunt force injuries from the landing, and may include massive head injuries even if the vehicle impact alone was not immediately lethal. In some cases, the secondary-impact head injury is the cause of death, while the primary impact injury (bumper fracture) is relatively minor. This sequence must be clearly explained to the court to avoid the incorrect conclusion that 'the vehicle killed the victim by hitting her head' when in fact the vehicle hit the legs and the ground killed by hitting the head.
Distinguishing pedestrian from occupant injuries: vehicle occupants (driver, passengers) in frontal collisions show a different injury pattern: steering wheel injuries to the chest (sternal fracture, cardiac contusion), seatbelt injuries (clavicle fracture, shoulder bruising, internal abdominal organ injuries from diagonal belt), and windscreen injuries to the face and head (depending on presence of airbags). The seatbelt bruise across the shoulder and chest is a hallmark occupant injury and indicates the person was belted at the time of collision.
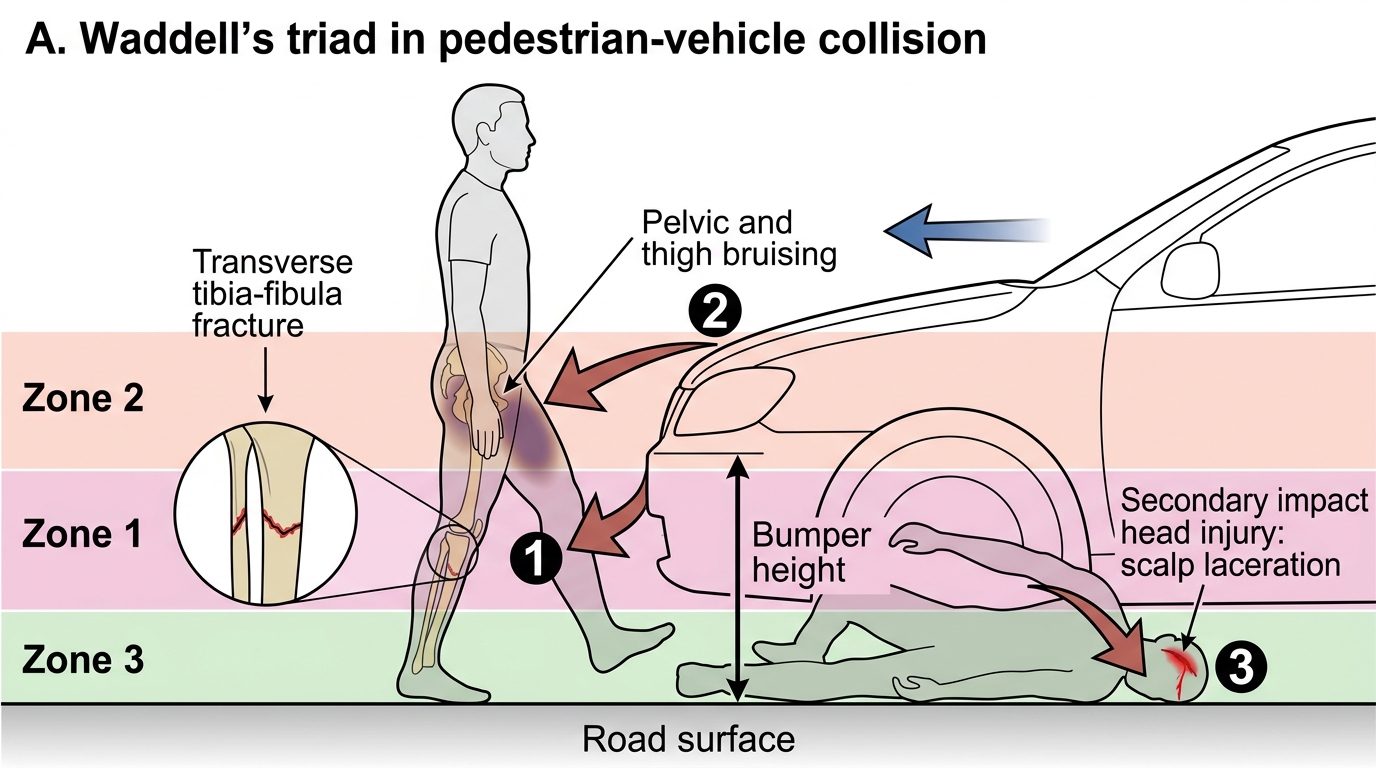
Waddell's Triad in Pedestrian-Vehicle Collision
SELF-CHECK
A pedestrian is found dead at a road traffic scene. Post-mortem shows: a transverse fracture of the left tibia-fibula at 42 cm above the heel, bruising of the left hip and pelvis, and a severe head injury from a scalp laceration. Applying the vehicular injury sequence, which injury represents the primary impact, and what does the fracture height indicate?
A. The head injury is the primary impact; the tibia fracture resulted from the victim falling after the head was struck
B. The pelvic bruising is the primary impact from the vehicle bonnet; the tibia fracture is a secondary fall injury
C. The tibia-fibula fracture is the primary (bumper) impact, indicating the vehicle's bumper was at approximately 42 cm height; the pelvic bruising is secondary (bonnet contact) and the head injury is tertiary (ground impact)
D. All three injuries are simultaneous; the vehicle struck the victim at multiple levels at the same moment
Reveal Answer
Answer: C. The tibia-fibula fracture is the primary (bumper) impact, indicating the vehicle's bumper was at approximately 42 cm height; the pelvic bruising is secondary (bonnet contact) and the head injury is tertiary (ground impact)
In a pedestrian-vehicle collision, the injury sequence is: bumper contact (lower limb fracture) → bonnet contact (thigh/pelvic injury) → ground impact (head injury). The transverse tibia-fibula fracture at 42 cm above the heel is the bumper fracture — primary impact — and its height indicates the striking vehicle's bumper was approximately 42 cm high, consistent with a sedan or small car. Pelvic bruising is secondary impact (bonnet). Head injury is tertiary (ground). Understanding this sequence and documenting the fracture height is essential for vehicle identification and accident reconstruction.
Run-Over and Dragging Injuries
Run-over injuries occur when a vehicle's wheel passes over part of or the entire body after the primary impact has thrown the victim to the ground. These injuries are qualitatively different from the initial impact injuries — they result from the compression of soft tissue and bone between the heavy vehicle wheel and the road surface, combined with the forward motion of the wheel which drags across the surface.
Tyre-tread patterned abrasions are the hallmark of run-over: the tyre's tread pattern is imprinted on the victim's skin as patterned abrasions, allowing forensic examination to determine the type of tyre (commercial vehicle vs passenger car tread pattern), the width of the tyre, and — critically — the direction of travel (the abrasion pattern on skin is oriented in the direction the tread moved, allowing reconstruction of the vehicle's travel direction relative to the victim). Each tyre brand has a unique tread pattern; in cases where a suspect vehicle has been seized, tread pattern comparison between tyre and wound is a forensic science examination.
Organ bursting is characteristic of run-over: when the wheel passes over the abdominal or thoracic region, the sudden compression can exceed tissue failure thresholds, causing the stomach, bladder (especially if full), or liver to rupture — producing visceral injury out of proportion to external wound appearance. The external skin may appear relatively intact (the tread abrasion or a contusion) while internal organs are ruptured.
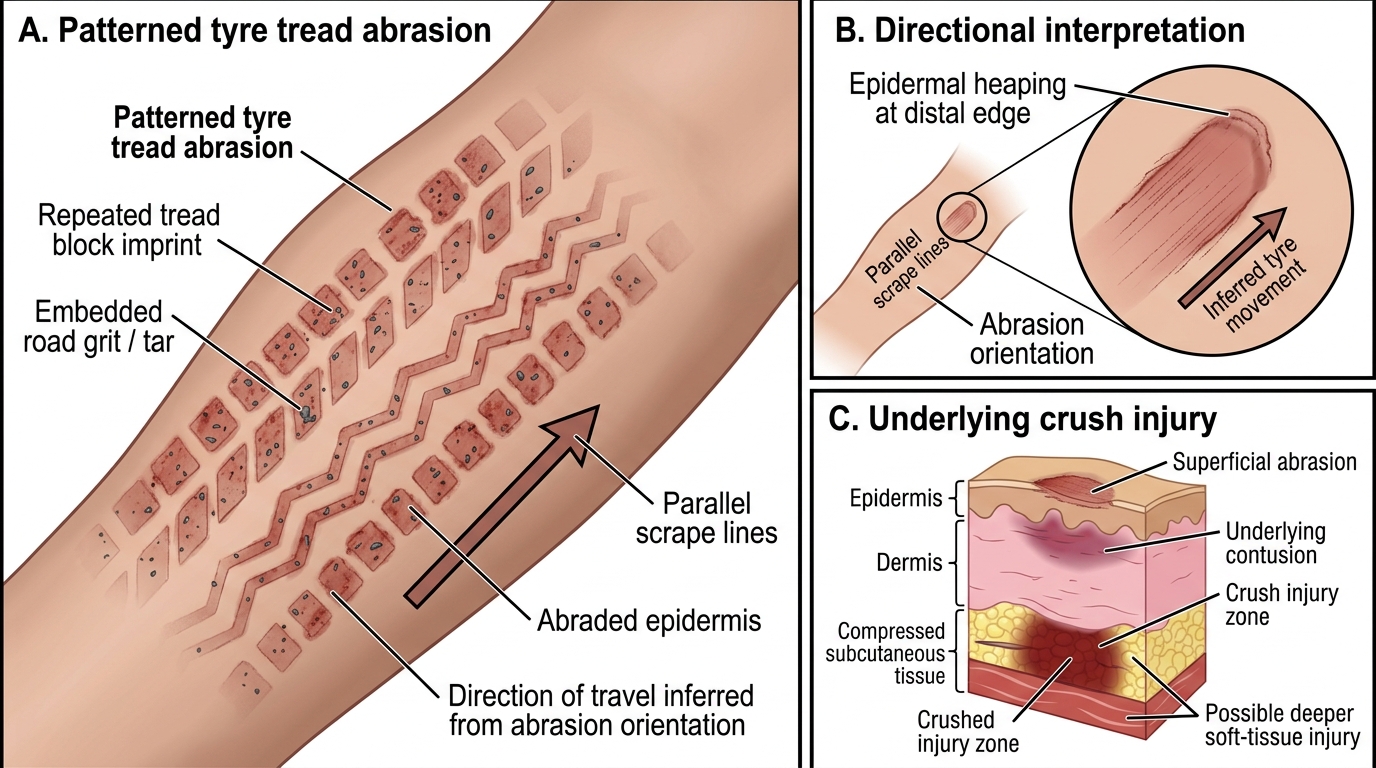
Patterned Tyre Tread Abrasion and Crush Injury
Dragging injuries occur when the victim is dragged along the road surface by the vehicle — entangled in the vehicle's undercarriage or dragged by clothing. Dragging produces extensive linear road abrasions along the length of the body, often with embedded road grit and tar, and in the direction of drag. Multiple layers of clothing may show corresponding abrasion and tears. The distribution and direction of dragging abrasions map the victim's position under or behind the vehicle.
Dry versus wet road: wet road surface produces water-lubricated abrasions that are less deep but wider; dry road produces deeper, narrower abrasions that may embed grit. The presence of road material (tarmac, gravel, glass) in the wound is itself forensic evidence of run-over or dragging.