Page 7 of 14
FM14.{18,20} | Court Skills: Dying Declaration & Expert Evidence — SDL Guide
Learning Objectives
- Demonstrate the step-by-step procedure for recording and certifying a dying declaration in a simulated or supervised clinical environment, including assessment of mental fitness
- Prepare a structured expert witness report for submission to a court, including qualifications, basis of examination, findings, expert opinion, and caveats
- Demonstrate appropriate conduct and responses in a simulated cross-examination as a medical expert witness, applying the principles of duty to court and scientific honesty
INSTRUCTIONS
Forensic medicine competencies FM14.18 and FM14.20 are performance skills — they are assessed not by recall of theory but by demonstration of correct procedure in simulated or supervised real-world settings. This module takes you from knowing the rules (which earlier SDLs covered) to doing the procedure correctly, under time pressure and with the specific pitfalls that typically trip up even well-read students. Both skills — recording a dying declaration and giving expert evidence — require the integration of legal knowledge, clinical assessment, structured documentation, and professional composure, simultaneously. This module walks you through each skill step-by-step.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
SIMULATED SCENARIO A — It is 11:30 PM. A 40-year-old woman is admitted to your casualty with 85% body surface area burns. She is conscious and says, in a barely audible voice: 'My husband poured kerosene on me and set me alight. I want you to write this down. I know I won't survive.' The duty magistrate is on leave; the night-duty magistrate answers your call but says he is 35 km away and cannot reach the hospital for at least 90 minutes. The woman's SpO2 is falling. You have 15 minutes, perhaps less. What do you do, in what order, and what do you write? SIMULATED SCENARIO B — Six months later, you receive a Sessions Court summons in the same case. The husband's defence lawyer has learned that you recorded the dying declaration without a magistrate and is preparing to challenge its validity. He will also cross-examine you on whether the woman was truly mentally competent at the time — was she delirious from pain? Was she in shock? Could she have fabricated the account to destroy her husband out of spite? You sit in the witness box, and the cross-examination begins. Both scenarios require not just knowledge, but the ability to perform under pressure with precision. This module builds both skills.
WHY THIS MATTERS
The dying declaration and expert evidence skills are among the highest-stakes clinical competencies in forensic medicine. Unlike most clinical procedures, these skills directly determine outcomes in criminal justice proceedings — whether a perpetrator is convicted, whether a victim's last testimony reaches the court, whether the truth survives a legal challenge. In many districts of India, the forensic physician is the only medically trained person available at the moment of a dying declaration; there is no other safety net. And in every murder, rape, or grievous assault trial that reaches the Sessions Court, the forensic physician's testimony is a central pillar of the prosecution's case. These skills are therefore not optional career competencies — they are core duties of every registered medical practitioner.
RECALL
From the earlier SDLs in this cluster, bring to mind: (1) the four conditions for a valid dying declaration — belief in impending death, mental competence of the declarant, relation to cause of death, and attestation by magistrate or doctor in the magistrate's absence; (2) the distinction between a dying declaration (no oath, no cross-examination, doctor may record) and a dying deposition (oath required, cross-examination, magistrate mandatory); (3) the examination sequence in court — examination-in-chief, cross-examination (leading questions permitted), re-examination, court questions; (4) the expert witness's duty to the court, not to either party; and (5) that perjury under BNS 2023 carries imprisonment up to seven years. These knowledge anchors are the foundation on which this module's practical skills are built.
Legal and Professional Context for Clinical Performance Skills
The performance skills in this module occupy a specific legal and professional space that is distinct from routine clinical procedure. When you take a blood pressure reading, the primary risk of doing it incorrectly is a clinical one — you might miss a diagnosis. When you record a dying declaration incorrectly, you may fatally compromise a murder prosecution, or — equally serious — you may cause an innocent person to be wrongly implicated. When you give expert evidence incorrectly, you may be found in contempt of court, have a stricture recorded against you by the judge, or be reported to the NMC for professional misconduct.
The legal authority for recording a dying declaration in the absence of a magistrate flows from the Bharatiya Sakshya Adhiniyam (BSA) 2023 — specifically the provisions making the statement of a deceased person admissible as evidence. The courts have repeatedly held that a dying declaration recorded by a doctor — even without a magistrate — is admissible, provided the doctor certifies the mental fitness of the declarant at the time. The key Supreme Court cases (such as Paras Yadav vs State of Bihar, and the consistent line of High Court authority on the subject) establish that the doctor's fitness certificate is the functional equivalent of the magistrate's attestation when a magistrate cannot be obtained in time.
The authority for a doctor to give expert evidence flows from BSA 2023 Section 45, which empowers courts to receive expert opinion on questions of science or specialised knowledge. The forensic physician is an expert under this section by virtue of their medical qualifications and forensic training. However, the BSA does not simply allow the doctor to say anything they choose — the expert opinion must be founded on a proper examination, recorded in a proper report, and given honestly. An expert who departs from this standard does not merely face professional criticism — they may face criminal liability for perjury (BNS 2023) or civil liability for negligent expert evidence.
Under the NMC Act 2020, a doctor's obligations as a professional extend into the courtroom and into every medicolegal role they perform. The Professional Conduct Regulations require the doctor to act with the highest standards of integrity in all professional capacities. A doctor who gives expert testimony that is deliberately favourable to the party who called them — or who records a dying declaration inaccurately because the correct account was inconvenient — is in breach of these regulations and may face suspension or deregistration.
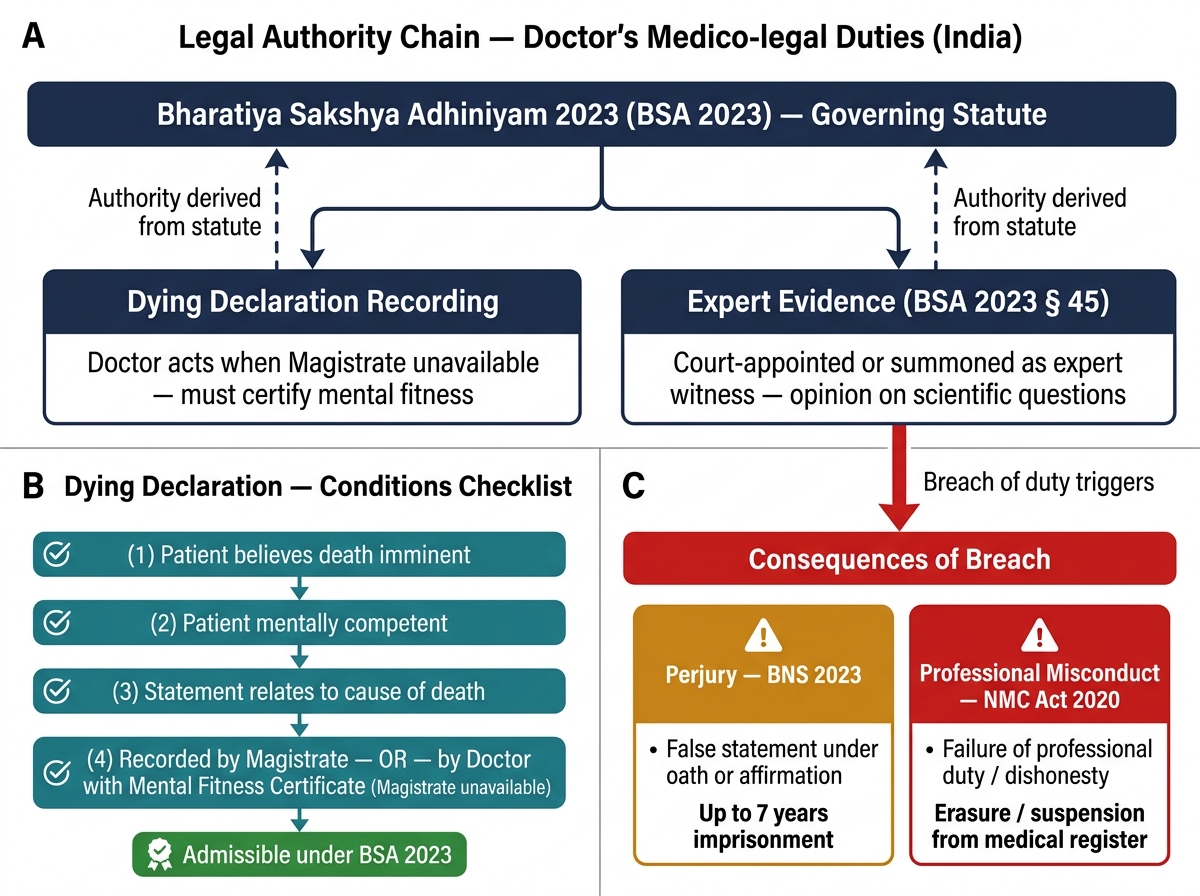
Legal Authority Chain: Dying Declaration & Expert Evidence — Duties and Consequences
Governing Principles: Dying Declaration Recording
Before performing the skill of recording a dying declaration, the practitioner must internalise the governing principles — the legal framework, the conditions checklist, and the boundaries of their authority. These principles are what you will draw on under time pressure when there is no opportunity to look up a textbook.
The legal basis
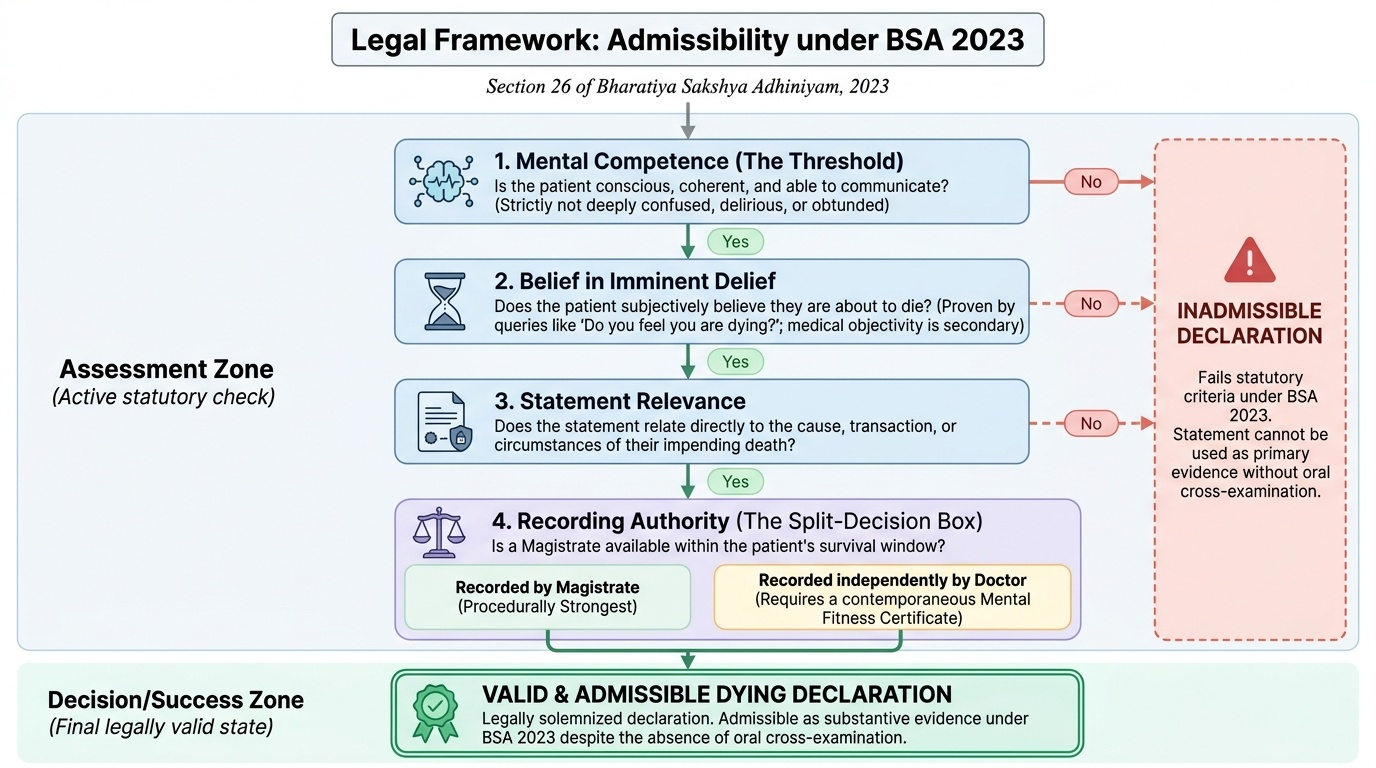
A dying declaration is admissible under the BSA 2023 as the statement of a deceased person, because the law treats the imminence of death as providing a guarantee of truthfulness equivalent to the solemnity of an oath. This is a legal presumption — it does not mean dying declarations are always true, but it means they are treated as specially reliable evidence and are admissible without requiring the declarant to be alive to testify. The critical prerequisite is that the declarant must have believed they were about to die at the time of making the statement.
The conditions checklist (COMMIT to memory)
Before recording begins, the doctor must confirm ALL of the following conditions:
- Is the patient conscious and able to communicate? Not merely responsive to pain, but able to answer purposeful questions, identify themselves, and give a coherent account. This is the mental fitness threshold — a patient who is deeply confused, delirious, or obtunded does NOT meet this standard, and recording a statement from such a patient is likely to be challenged and may be inadmissible.
- Does the patient believe they are about to die? Ask directly: 'Do you believe you will survive this?' or 'Do you feel you are dying?' The patient need not be certain — a genuine belief in impending death is sufficient. It does not matter whether the doctor also believes the patient will die; the test is the patient's subjective belief.
- Does the patient want to make a statement about the cause or circumstances of their situation? The statement must relate to the cause or circumstances of the danger the patient is in, or to the transaction connected with their death.
- Is a magistrate available within the time the patient can survive? If a magistrate can reach the patient in time, wait for the magistrate — the magistrate's presence makes the declaration procedurally stronger. Call for the magistrate immediately upon recognising the situation. Only proceed to record independently if the magistrate cannot reach in time and the patient's condition is deteriorating.
Mental fitness certification
The doctor's mental fitness certificate is the document that establishes the evidentiary validity of the declaration in the magistrate's absence. It must state:
- The date, time, and place of the examination
- That the doctor personally examined the patient and assessed their level of consciousness
- That at the time of making the declaration the patient was conscious, oriented to person and time, able to understand questions put to them, and able to give a coherent account of events
- That the doctor is satisfied the patient was not under the influence of substances that might compromise cognition
- A note of any medications the patient had received prior to the declaration and whether they could affect cognition
This certificate must be written separately from the declaration itself — as a distinct, signed, dated document — not merely as a marginal note.
Provided image
SELF-CHECK
A severely injured patient is brought to casualty. She is moaning in pain, responds to her name, but her answers are confused and she does not consistently know what day it is. She begins to give an account of how she was attacked. Should the doctor record this as a dying declaration?
A. Yes — the patient is responding to her name and giving an account, which is sufficient mental fitness
B. Yes — if the doctor certifies the declaration was made while the patient was in pain, courts will accept it
C. No — the patient is confused and disoriented; the mental fitness threshold (conscious, oriented, coherent communication) is not met
D. No — a dying declaration can only be recorded by a magistrate, not a doctor
Reveal Answer
Answer: C. No — the patient is confused and disoriented; the mental fitness threshold (conscious, oriented, coherent communication) is not met
Mental fitness for a dying declaration requires more than basic responsiveness. The patient must be conscious, oriented (to person, place, time), and capable of giving a coherent, purposeful account. A patient who is confused and disoriented does not meet this standard. Recording a declaration from such a patient is likely to be challenged in court, and the doctor's fitness certificate — certifying a confused patient as mentally competent — would be false. The correct action is to manage the patient, repeat the fitness assessment as the patient's condition improves, and record the declaration only when the mental fitness threshold is genuinely met.
Governing Principles: Expert Evidence
The forensic physician who is called to give expert evidence in court is not merely a professional appearing in an unusual setting — they are occupying a specific legal role with specific obligations and specific protections. Understanding the governing principles of expert evidence is the foundation for the practical skill of expert testimony.
Who is an expert under BSA 2023?
Under BSA 2023 Section 45, an expert is a person specially skilled in foreign law, science, art, handwriting, or finger impressions, or any other field of specialised knowledge. A forensic physician qualifies as an expert in medicine as applied to legal questions — cause of death, nature of injuries, toxicology, age estimation, and similar matters. Crucially, the court determines whether a person qualifies as an expert — the doctor must be prepared to state their qualifications, experience, and training when asked. If a court determines that a witness is not an expert in the relevant field, their opinion evidence cannot be admitted as expert evidence (though they may still give factual testimony about what they observed).
The expert's duty is to the court
This principle — stated earlier as a theory — has specific operational implications. The expert's opinion must be the opinion they genuinely hold based on their examination and scientific knowledge. If asked to give an opinion that they do not hold, the expert must decline. If the scientific evidence genuinely supports more than one conclusion, the expert must say so rather than picking the conclusion that favours the party who called them. If the evidence is inconclusive, saying 'the evidence is inconclusive' is the correct — and legally required — answer.
Many experienced defence lawyers use a particular strategy: they ask a series of questions designed to get the expert to agree that the evidence is also consistent with an innocent explanation. The forensic physician must engage with this honestly. If the injuries are consistent with an innocent explanation (e.g., a fall rather than an assault), the expert must concede that possibility — but they can, and should, also state whether that explanation is more or less likely than the violent cause, and why, based on the wound characteristics.
The expert report
Before testifying, the forensic physician typically prepares a formal expert report. The structure of a sound expert report follows five sections:
- Expert qualifications: Name, degree(s), postgraduate qualifications, current post, years of forensic experience, number of autopsies or examinations performed. This section establishes the basis for the court to accept the doctor as an expert.
- Basis of examination: Date, time, and place of examination; whether the examination was of a living patient or a deceased person; who was present; the source of any history relied upon.
- Objective findings: The factual findings of the examination — injuries described in precise anatomical and wound-type terms, as per the wound certificate format. Only what the doctor personally observed.
- Expert opinion: The doctor's interpretation of those findings — what they imply about cause of death, weapon used, time since death, nature and mechanism of injury. Stated as 'In my opinion, based on the above findings...' — never as fact.
- Caveats and limitations: Honest acknowledgement of the limits of the evidence — 'I cannot determine the exact time of death,' 'The wound characteristics are consistent with either X or Y,' 'Further toxicological analysis would be required to confirm.' A good expert report that acknowledges limitations is more credible than one that claims false certainty.
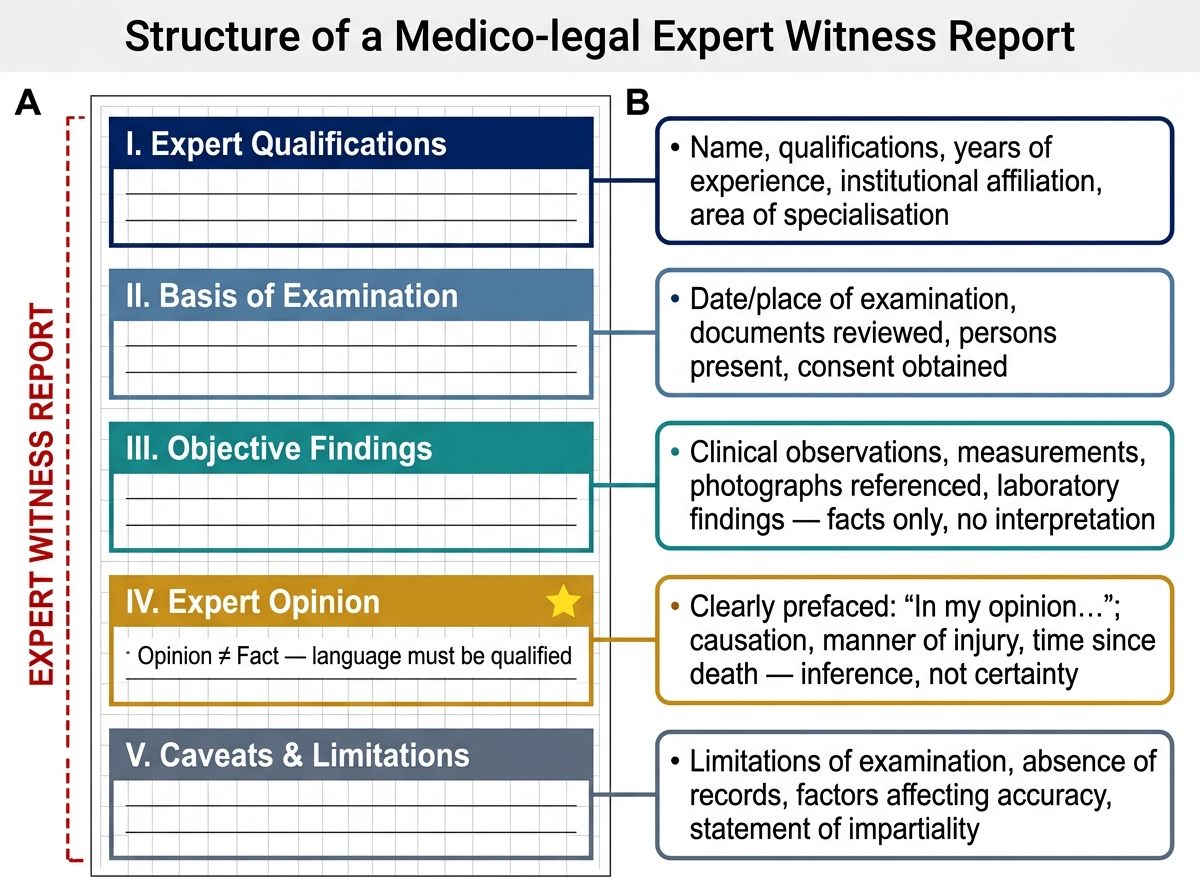
Anatomy of an Expert Witness Report: Five-Section Structure with Annotation