Page 8 of 14
FM14.{18,20} | Court Skills: Dying Declaration & Expert Evidence — SDL Guide (Part 2)
Method and Documentation: Step-by-Step Skill Performance
Provided image
The governing principles described above must now be translated into a reproducible, step-by-step procedure that can be performed correctly under the pressure of a dying patient or a courtroom. This section provides the precise procedure for each skill — not the theory, but the doing.
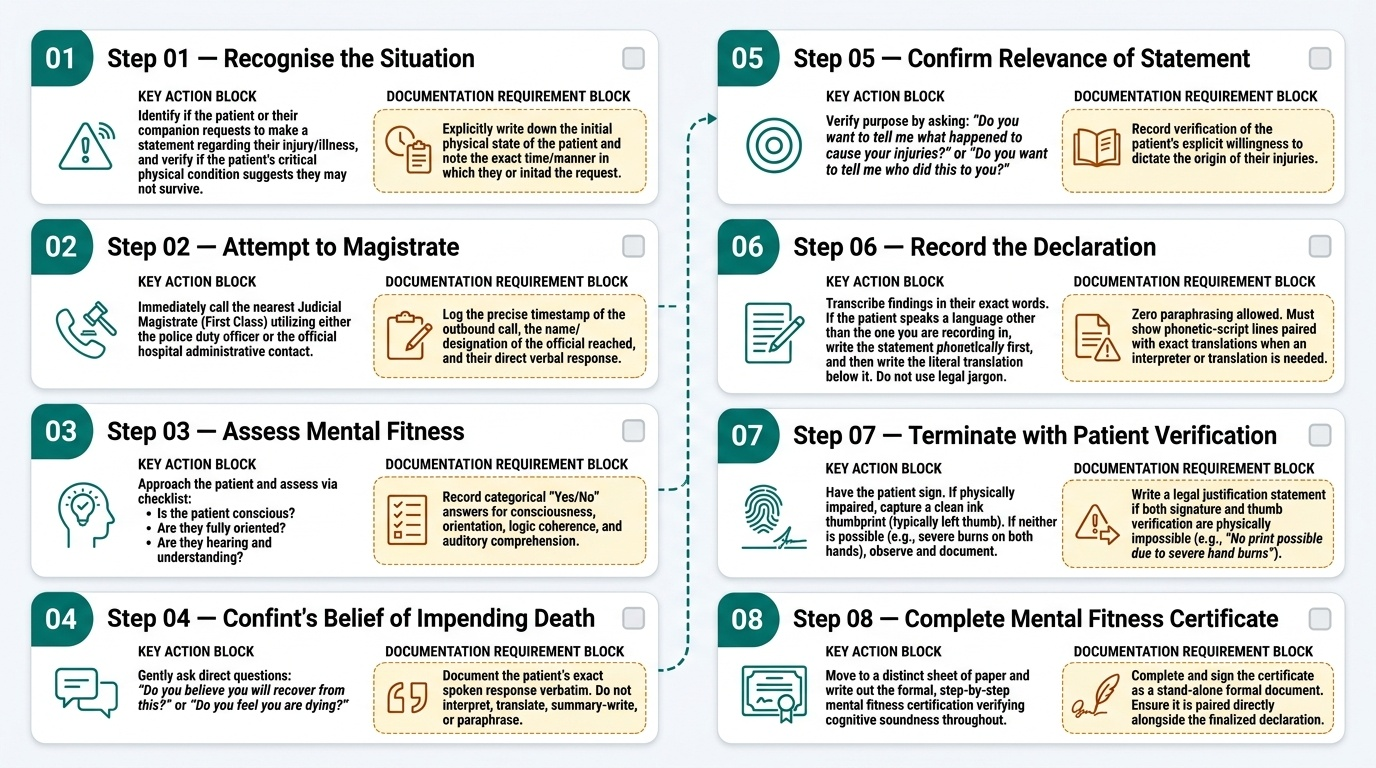
SKILL A: Recording a Dying Declaration (Step-by-Step)
Step 1 — Recognise the situation: The patient or their companion indicates the patient wants to make a statement about how they were injured or became ill, and the patient's condition suggests they may not survive.
Step 2 — Attempt to reach a magistrate: Immediately call the nearest Judicial Magistrate (First Class) through the police duty officer or hospital administrative contact. Note the time of the call and the response in writing.
Step 3 — Assess mental fitness: Approach the patient and assess: Is the patient conscious? Are they oriented (know their name, where they are, approximately what time it is)? Can they give a coherent account? Can they hear and understand your questions? Record your findings.
Step 4 — Confirm the patient's belief in impending death: Ask gently: 'Do you believe you will recover from this?' or 'Do you feel you are dying?' Note the patient's response verbatim.
Step 5 — Confirm the relevance of the statement: Ask: 'Do you want to tell me what happened to cause your injuries?' or 'Do you want to tell me who did this to you?'
Step 6 — Record the declaration: Ask the patient to tell you what happened. Write their account in their own words — verbatim where possible. If the patient uses a language other than the one you are writing in, write the statement phonetically in the patient's language and provide a translation below it. Do not paraphrase or translate into formal legal language. Do not interpret or elaborate — record exactly what the patient says.
Step 7 — Have the patient sign or thumb-impress the statement: If the patient is physically able to sign, ask them to sign the written statement. If not able to sign, obtain a thumb impression. If neither is possible due to the patient's physical condition (e.g., both hands burned), note this explicitly.
Step 8 — Complete the mental fitness certificate: On a separate sheet, write the formal mental fitness certificate (as described in the Governing Principles section). Sign, date, and affix your hospital stamp.
Step 9 — Provide copies: Hand the original declaration and the mental fitness certificate to the investigating police officer as soon as possible (against a receipt). Retain a certified copy in the hospital records.
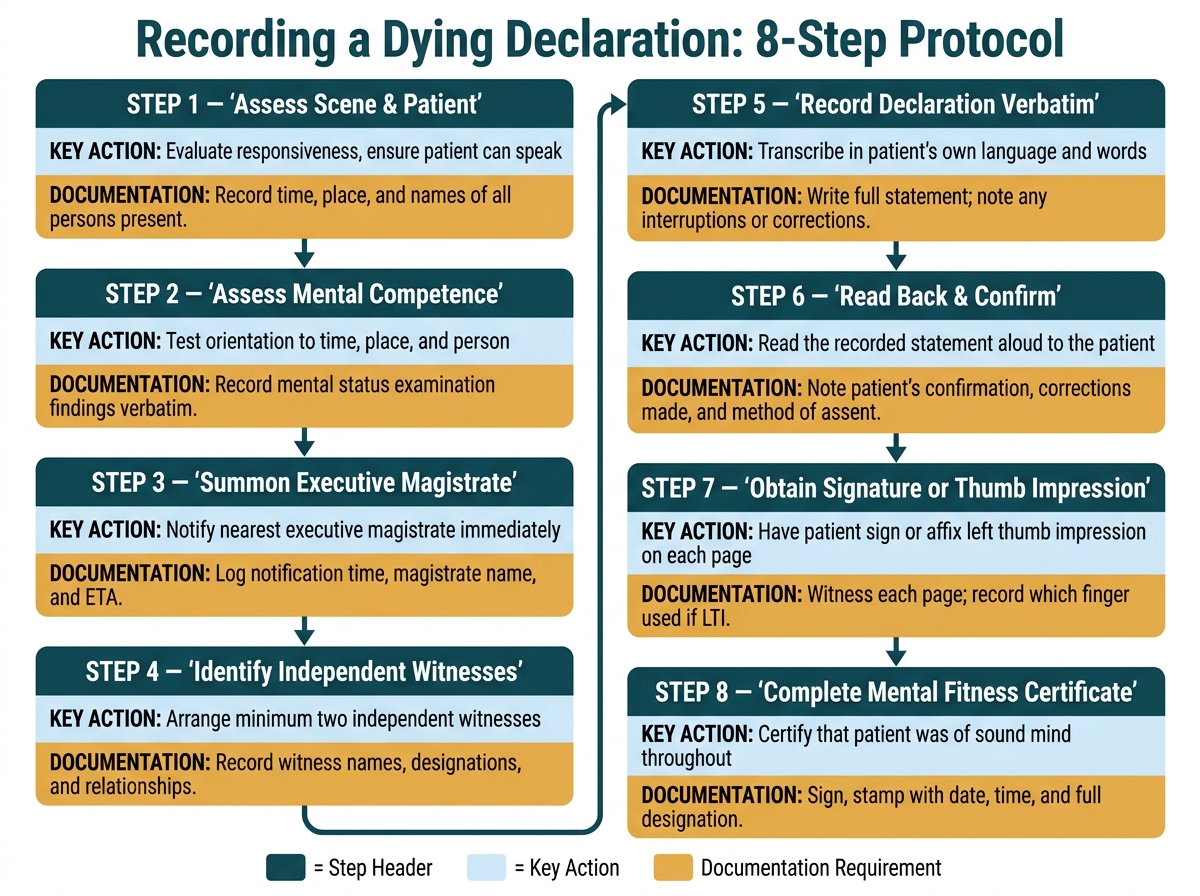
Eight-Step Protocol for Recording a Dying Declaration
SKILL B: Giving Expert Evidence — Preparation and Performance
Before court:
- Re-read your original report, notes, and any photographs at least 24 hours before the court date
- Identify the two or three most technically challenging aspects of your evidence — areas where the defence is likely to probe
- For each challenging area, formulate a clear, honest answer: what do you know with confidence, what is uncertain, what would change your opinion
- Bring all original documents, including the original wound certificate or post-mortem report, with a certified copy if available
- Arrive at court 15–30 minutes early; identify the courtroom; speak to the prosecutor to confirm the expected sequence of examination
In the witness box:
- State your full name, designation, hospital, and qualifications clearly
- When giving examination-in-chief: listen carefully to each question, answer precisely what is asked, use precise wound-type terminology, and give opinions as opinions ('In my opinion...') not as facts ('The injury was caused by...')
- When cross-examined: remain composed; answer leading questions with the evidence as it stands; concede genuine uncertainty without collapsing your entire testimony; distinguish between 'I cannot exclude X' (which means X is logically possible) and 'X is likely' (which requires positive evidence); never answer beyond your area of expertise
- If a question is misleading or based on a false premise, identify the premise politely: 'I would respectfully point out that the premise of that question is not consistent with my findings — my findings were...'
- If you need time to think, it is acceptable to pause before answering; a court is not a quiz show
- After re-examination: clarify any points the cross-examination may have made unclear; do not introduce new information
SELF-CHECK
During a moot court exercise, the defence counsel asks you (as the forensic expert): 'Is it not possible that the injuries you described could have been caused by a fall, rather than an assault?' The injuries include a single sharp incised wound with clean margins and no tissue bridges. Your most professionally appropriate response is:
A. 'No, that is not possible — falls do not cause clean incised wounds'
B. 'Yes, it is possible — any explanation is theoretically possible'
C. 'The wound characteristics — clean margins, no tissue bridges — are consistent with a sharp cutting weapon and are not characteristic of injuries typically caused by falls, which tend to produce lacerations with irregular margins and tissue bridges'
D. 'I cannot comment on what caused the injury — I only describe what I found'
Reveal Answer
Answer: C. 'The wound characteristics — clean margins, no tissue bridges — are consistent with a sharp cutting weapon and are not characteristic of injuries typically caused by falls, which tend to produce lacerations with irregular margins and tissue bridges'
The expert's duty is to give an honest, scientifically grounded opinion. Option A is overreaching (it states an absolute impossibility that may not be defensible). Option B is an abdication of expertise. Option D avoids giving an expert opinion, which defeats the purpose of the expert. Option C correctly states the wound characteristics, explains why they are more consistent with a sharp weapon than a fall, and does not overstate certainty — it says 'consistent with' and 'not characteristic of,' which reflects the genuine weight of the forensic evidence. This is exactly how expert evidence should be framed.
Applied Practice: Worked Scenarios
The principles and procedures above are now applied to two worked scenarios — the same scenarios introduced in the hook of this module. Working through these annotated examples prepares you for the OSPE assessment and for real-world performance.
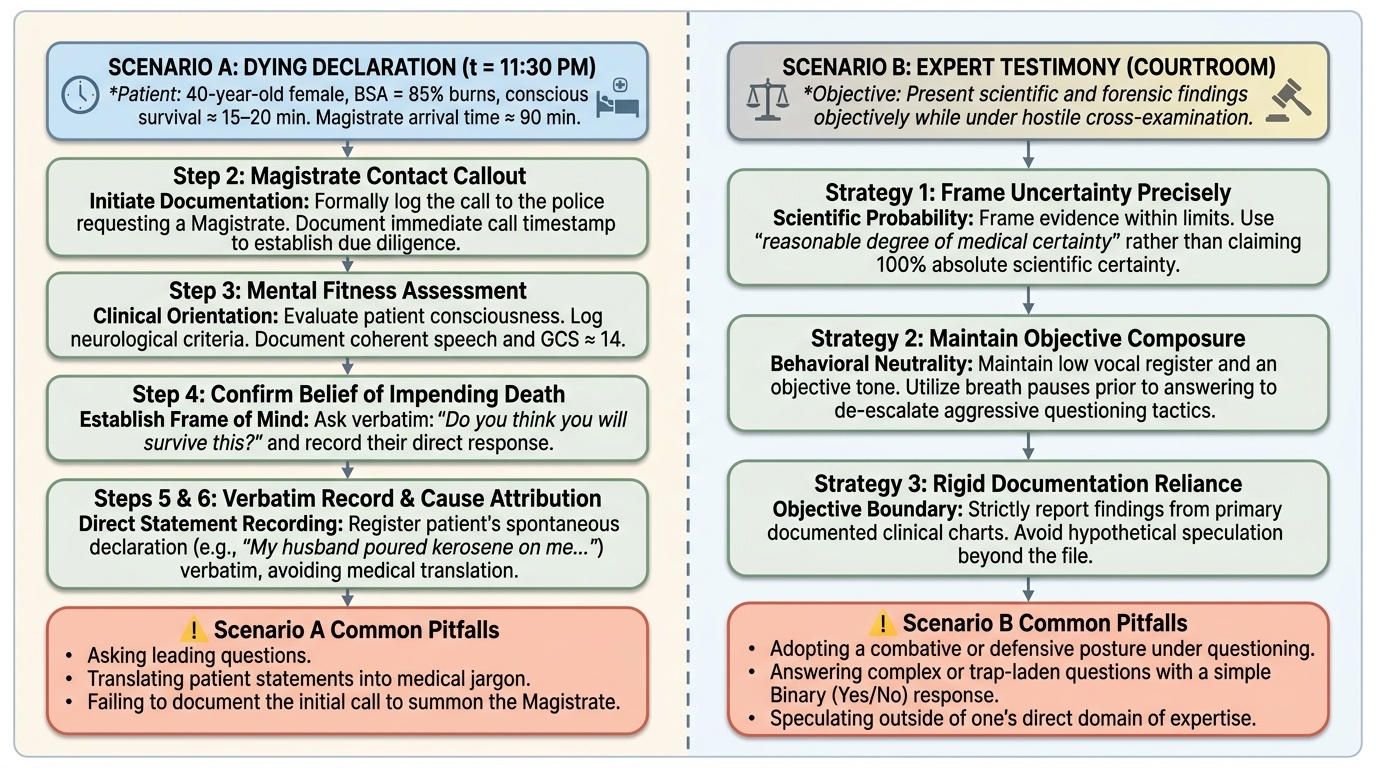
WORKED SCENARIO A: Burns Patient — Dying Declaration (11:30 PM)
Patient: 40-year-old woman, 85% BSA burns, declining SpO2, 15–20 minutes estimated conscious survival. Magistrate 90 minutes away. No other legally authorised recording agent available.
Step-by-step application:
Step 2 (Magistrate contact): You call the duty police officer and ask them to inform the magistrate. You note the time and the magistrate's estimated arrival in writing. This shows the court you tried to obtain magistrate attendance.
Step 3 (Mental fitness): You assess the patient: she opens eyes to voice, answers her name correctly, knows she is in hospital, is crying but coherent. You document: 'Patient conscious, oriented to person and place, able to follow questions and give purposeful answers. GCS approximately 14.'
Step 4 (Impending death belief): You ask: 'Do you think you will survive this?' She replies: 'No, doctor, I'm going to die. Please write what I say.' You document this response verbatim.
Step 5 (Relevance): She says spontaneously: 'My husband did this.' You note that the statement relates directly to the cause of her injuries.
Step 6 (Recording): You write: 'Statement of [Name], recorded on [Date] at [Time] at [Hospital]. Patient states in her own words: "My husband [Name] poured kerosene on me from behind and lit a match. It was at about 9 PM in our kitchen. He ran out of the house after that. I want to name him."' You do not add any interpretation or legal language.
Step 7 (Signature): You ask the patient to thumb-press the statement. Given that her hands are burned, you note: 'Due to full-thickness burns of both hands, the patient was unable to sign or thumb-press. This is documented in the clinical records and the police have been informed.'
Step 8 (Mental fitness certificate): You write a separate document: 'I, [Name], [Designation], [Hospital], hereby certify that at [Time] on [Date], [Patient Name], aged approximately 40 years, was conscious, oriented to person and place, able to communicate purposefully, and understood the questions put to her. She was not under any sedating medication at the time of recording this statement. I am satisfied that she was mentally competent at the time of making the above statement. Signature, Date, Hospital Stamp.'
Common pitfalls in this scenario:
- Recording the statement BEFORE assessing mental fitness — the court will ask whether the mental fitness was assessed before or after the declaration
- Not attempting to contact the magistrate — if no attempt is documented, the defence will argue the doctor bypassed the preferred procedure
- Paraphrasing the patient's account — 'She said her husband attacked her' instead of her verbatim words
- Writing the mental fitness certificate as a marginal note on the declaration itself rather than as a separate document
WORKED SCENARIO B: Expert Testimony — Sessions Court
Six months later, the case comes to trial. The husband is charged under BNS 2023. You are called as an expert by the prosecution.
Examination-in-chief: You state your qualifications, the date and circumstances of the examination, and your clinical findings (mental fitness, the declaration, and your clinical management of the patient). The prosecutor asks your opinion on the patient's mental state at the time of recording. You state: 'In my opinion, based on my clinical assessment, the patient was conscious, oriented, and mentally competent to make a valid statement at the time of recording.'
Cross-examination: The defence counsel asks: 'Is it not true that a patient in severe pain and with 85% burns would be in severe psychological distress, affecting their reliability?' You respond: 'Psychological distress and pain do not in themselves impair the cognitive functions required for a dying declaration — orientation, coherence, and purposeful communication. The patient demonstrated all three at the time of my assessment. I documented my assessment contemporaneously.'
The defence then asks: 'Could the patient have been hallucinating due to pain, carbon monoxide from the fire, or shock?' You respond: 'Carbon monoxide exposure may cause cognitive impairment, and I address that specifically: the patient was brought by ambulance with supplementary oxygen and had a carboxyhaemoglobin level within acceptable limits at the time of the recording. I assessed her orientation and coherence directly before recording began. There was no clinical evidence of cognitive impairment from any of the causes you have mentioned at the time of the declaration.'
Lesson: Anticipate challenges to mental fitness. Document your reasoning at the time of the examination, not retrospectively. The contemporaneous clinical record is your strongest defence.
Provided image
SELF-CHECK
In the dying declaration for the burns patient, the doctor failed to note the time of the mental fitness assessment in the certificate. The defence uses this omission to argue the doctor assessed mental fitness hours after the declaration. How damaging is this omission?
A. Not damaging — the doctor's clinical judgement is sufficient regardless of when the assessment was documented
B. Moderately damaging — the court will note the omission but will still accept the declaration
C. Potentially fatal to admissibility — the defence can credibly argue the mental fitness was assessed retrospectively, undermining the validity of the certificate
D. Correctable by the doctor providing an oral statement in court that the assessment was done before the declaration
Reveal Answer
Answer: C. Potentially fatal to admissibility — the defence can credibly argue the mental fitness was assessed retrospectively, undermining the validity of the certificate
Contemporaneous recording is the foundational principle of all medicolegal documentation. A mental fitness certificate without a time stamp is legally vulnerable because the defence can argue — and the court may accept — that the assessment was made retrospectively, perhaps after the patient had deteriorated cognitively. This could render the dying declaration inadmissible. An oral statement in court that the assessment was done first carries much less weight than contemporaneous documentation. The lesson: record the time of every step in the dying declaration procedure as you perform it.
CLINICAL PEARL
In both skills covered in this module, the most common failure mode is the same: doing the right thing but not documenting it in a way that can withstand legal scrutiny. The courts do not doubt that most doctors act with integrity — they demand that integrity be demonstrable from the document, not just from the doctor's say-so. For the dying declaration: make the mental fitness certificate a separate, timed, signed document. For expert evidence: write 'In my opinion' before every interpretive statement in your report. These small disciplinary habits are the difference between a legally defensible performance and a professional embarrassment.