Page 2 of 23
FM10.16-17 | Bioethics & the Four Principles — SDL Guide
Learning Objectives
- Define bioethics and describe its scope as a systematic discipline
- Explain the four principles of biomedical ethics (Beauchamp and Childress): autonomy, non-maleficence, beneficence, and justice
- Apply the four principles to analyse ethical dilemmas in clinical practice
- Recognise situations where principles conflict and describe how such conflicts are approached
INSTRUCTIONS
Every clinical decision a doctor makes has an ethical dimension. When you decide how much information to give a patient before a procedure, or whether to override a patient's refusal of treatment, or how to allocate a scarce hospital bed between two equally sick patients, you are implicitly applying ethical principles. Bioethics provides the systematic framework for making these decisions explicitly and defensibly — not just by instinct or habit, but by reasoning through the relevant principles with clarity. This module introduces the most widely used framework in contemporary medical ethics: the four principles of Beauchamp and Childress.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman is admitted to your ward following a road traffic accident. She has a haemothorax requiring urgent intercostal drainage. She is conscious, oriented, and in pain. As you explain the procedure, she says clearly: 'I refuse. I know what this is, I understand the risk of refusing, and I am refusing.' Her oxygen saturation is 88% and falling. She will likely die without the procedure. She has no known psychiatric diagnosis. You have about three minutes to decide. What do you do — and on what basis? This scenario places four ethical principles in direct conflict: respecting her autonomy says you must defer to her decision; beneficence says you should save her life; non-maleficence says both acting and not acting may cause harm; justice says nothing about this specific conflict but operates in the background. How you reason through this moment is what bioethics is for.
WHY THIS MATTERS
Bioethics is not an academic exercise for philosophers — it is the practical reasoning toolkit for every clinical decision that involves competing obligations, uncertain evidence, or a patient whose values differ from your own. As a doctor, you will face situations daily where doing the technically 'right' thing and doing the ethically 'right' thing are not the same question. The NMC Code of Medical Ethics, your duty of informed consent, your obligations in public health emergencies, your responsibilities in end-of-life care — all of these are applications of bioethical principles. Understanding the four-principle framework lets you reason about these situations systematically rather than relying on intuition that may itself be biased by training, culture, or fatigue.
RECALL
Before we begin:
- In the previous module (me1-history), we saw that the Belmont Report articulated three foundational research ethics principles. Can you name them? How do they compare to the four principles you will learn today?
- Think of a clinical scenario you have observed or read about where a doctor and a patient disagreed about the right course of action. Who had the 'right' to decide — and on what basis?
- What do you understand by the phrase 'informed consent'? What information must a patient receive, and what conditions must be met, for consent to be valid?
Legal and Professional Context: Why Bioethics Matters for Doctors
Bioethics emerged as a distinct academic and practical discipline in the early 1970s, driven by a confluence of medical advances that outpaced existing ethical frameworks — organ transplantation, life-sustaining technology, genetic manipulation, and large-scale clinical trials — and by public revelations of research abuses, most notably the Tuskegee Syphilis Study. The word itself was coined by Van Rensselaer Potter in 1970, who envisioned it as the 'science of survival' — the systematic application of ethical thinking to all matters touching life and living.
In the clinical context, the need for a systematic bioethical framework arises from the power asymmetry of the doctor-patient relationship. The doctor possesses knowledge, skill, institutional authority, and access to resources that the patient does not. Without an ethical framework to structure how that power is exercised, the relationship is vulnerable to paternalism — the doctor deciding what is best for the patient without the patient's meaningful participation. Modern medicine's move away from paternalism toward patient-centred care is, at its core, an ethical project driven by bioethical thinking.
From a legal standpoint, bioethical principles are increasingly codified: the right to informed consent is legally enforceable; the duty of confidentiality has both statutory and common-law basis; the right of a competent adult to refuse treatment — even life-saving treatment — is recognised in Indian case law (though the practical application remains contested). For the forensic medicine student, bioethics is also the theoretical foundation for understanding medical negligence, professional misconduct, and the doctor's legal as well as moral responsibilities.
The most influential systematic framework in contemporary bioethics was developed by American philosophers Tom Beauchamp and James Childress in their foundational text Principles of Biomedical Ethics (first published 1979; most commonly cited 4th edition 1994 and 7th edition 2012). Their four-principle approach — often called principlism — provides a common language and a structured method for analysing ethical problems in medicine.
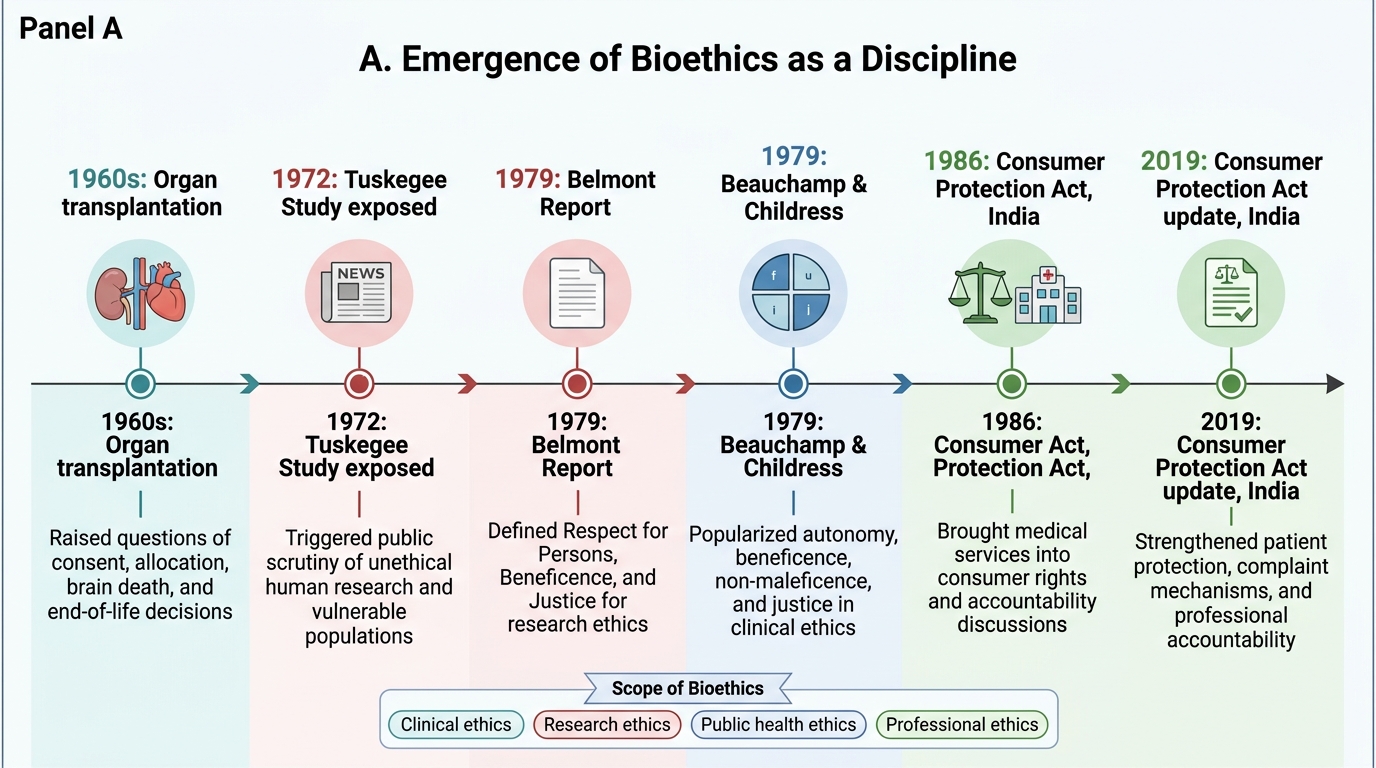
Emergence of Bioethics as a Discipline
What is Bioethics? Definition, Scope and Origins
Bioethics is the systematic, disciplined study of the ethical, social, and legal questions raised by the biological sciences and by medical practice. Its scope extends from the bedside (individual clinical decisions) to the boardroom (health policy and resource allocation) to the laboratory (research ethics and genetic science). In the context of clinical medicine — which is the focus for a medical student — bioethics provides the framework for:
- Clinical ethics: decisions about individual patient care — consent, confidentiality, end-of-life care, refusal of treatment
- Research ethics: the ethics of conducting research on human and animal subjects — informed consent, risk-benefit analysis, vulnerable populations
- Public health ethics: the ethics of population-level health interventions — mandatory vaccination, quarantine, health resource allocation
- Professional ethics: the ethics of the doctor-doctor and doctor-institution relationship — conflicts of interest, professional responsibilities, collegial conduct
The emergence of bioethics as a formal discipline required three convergent developments: first, the recognition that clinical and research ethics raise genuinely difficult problems that cannot be resolved by professional custom alone; second, the availability of philosophical methods capable of systematic moral reasoning; and third, the inclusion of non-medical voices — philosophers, lawyers, patients, and public representatives — in the conversation about medical practice. This multi-disciplinary character distinguishes bioethics from older notions of 'medical ethics' that were primarily controlled by the medical profession.
IMPORTANT: In Indian FM examinations, 'bioethics' and 'medical ethics' are often treated as overlapping but not identical terms. Medical ethics typically refers to the professional code governing physician conduct (NMC Code 2002); bioethics refers to the broader theoretical discipline, of which the four principles are the most clinically applied framework.
The Four Principles of Biomedical Ethics
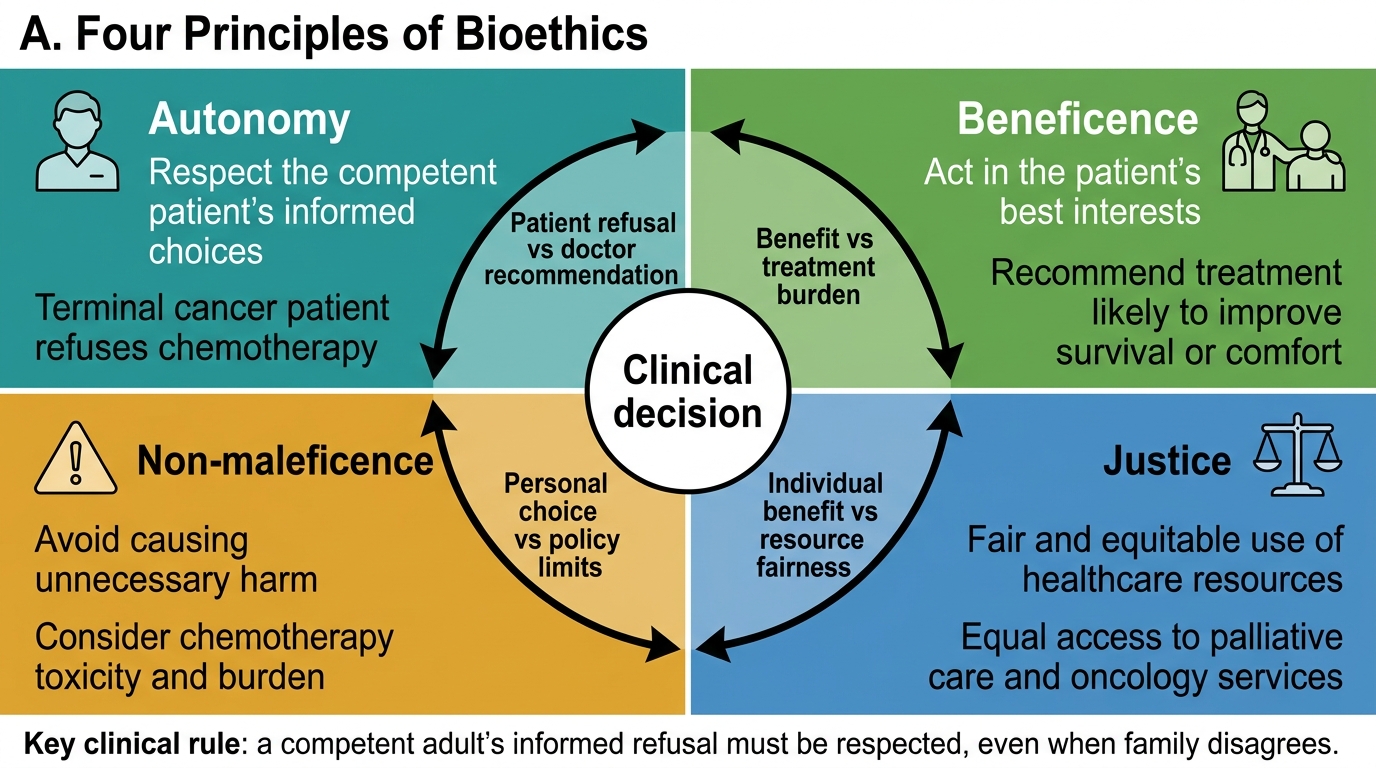
Beauchamp and Childress identified four prima facie moral principles — principles that are binding unless overridden by competing considerations in a specific situation — that together provide a comprehensive framework for analysing biomedical ethical problems.
1. Respect for Autonomy
Autonomy (Greek: autos = self, nomos = law) refers to the capacity of a person to make informed, uncoerced decisions about their own life. In the clinical context, respect for autonomy requires that doctors:
- Provide accurate, adequate, and comprehensible information about diagnosis, treatment options, risks, and alternatives
- Obtain voluntary informed consent before procedures
- Respect a competent patient's refusal of treatment, even when the doctor disagrees
- Maintain confidentiality of patient information
Autonomy is not absolute. It may be legitimately overridden when: the patient lacks decision-making capacity (unconsciousness, severe mental illness); the patient's decision poses a clear and substantial risk to others (infectious disease control); or in genuine emergencies where consent cannot be obtained and the presumed wish is for life-saving treatment.
2. Non-maleficence
Non-maleficence is the obligation to avoid causing harm — encapsulated in the Latin maxim primum non nocere ('first, do no harm'). In practice, almost every medical intervention carries some risk of harm: surgery can cause bleeding; chemotherapy causes toxicity; even well-intentioned advice may cause psychological distress. Non-maleficence therefore does not prohibit all action that might cause harm; rather, it requires that harm be minimised, that the doctor not impose unnecessary or disproportionate harm, and that the risk-benefit ratio be carefully assessed.
Non-maleficence is especially relevant in: prescribing decisions (polypharmacy, interactions); surgical risk assessment; end-of-life care (avoiding futile interventions that prolong suffering); and the doctrine of double effect (an action intended to benefit may have a foreseen but unintended harmful consequence, e.g. morphine for pain relief near end of life may hasten death).
3. Beneficence
Beneficence is the positive obligation to act in the patient's best interest — to do good. It goes beyond simply not harming: it requires that the doctor actively promote patient welfare. In the clinical context, this means:
- Providing technically competent care
- Referring when beyond one's competence
- Advocating for the patient's interests in the healthcare system
- Considering the patient's overall wellbeing, not just the presenting complaint
The tension between beneficence and autonomy is the most frequently encountered conflict in modern clinical ethics. The old paternalistic model gave beneficence near-absolute priority (the doctor decides what is best). Modern ethics gives substantial weight to autonomy — the patient's own values and goals are central to what counts as 'best interest'.
4. Justice
Justice in bioethics refers primarily to distributive justice — the fair allocation of healthcare resources and the equitable treatment of patients and populations. It asks: who gets access to scarce organs, expensive treatments, or overcrowded hospital beds? It also encompasses procedural justice (fair processes for making allocation decisions) and substantive justice (the right of each person to equal treatment, free from discrimination on grounds of race, caste, gender, religion, or socioeconomic status).
In Indian healthcare, justice is particularly salient given the enormous disparities in access to care between urban and rural populations, and between the insured and the uninsured. The justice principle underpins public health policy, the Ayushman Bharat scheme, and the ethical obligations of doctors working in resource-limited settings.
Four Principles of Bioethics in Clinical Decision-Making
SELF-CHECK
A 70-year-old man with terminal lung cancer refuses chemotherapy and states he wishes to spend his remaining time at home. His family insists that 'everything should be done' and pressures the treating doctor to override his decision. Which ethical principle most directly supports honouring the patient's refusal?
A. Justice — the patient has an equal right to treatment as any other
B. Non-maleficence — chemotherapy would cause harm
C. Respect for autonomy — a competent patient's informed refusal must be respected
D. Beneficence — it is in the patient's best interest to be treated
Reveal Answer
Answer: C. Respect for autonomy — a competent patient's informed refusal must be respected
Respect for autonomy is the directly applicable principle here: the patient is a competent adult, has made an informed decision about his own treatment, and his refusal must be respected even if the family disagrees and even if the doctor believes treatment might extend his life. Non-maleficence is relevant (chemotherapy causes harm) but is secondary. Beneficence, applied paternalistically, might suggest overriding his decision — but the modern ethical framework gives autonomy priority when the patient is competent and fully informed.