Page 3 of 23
FM10.16-17 | Bioethics & the Four Principles — SDL Guide (Part 2)
Applying the Four Principles: Clinical Tensions and Resolution
The four principles are prima facie — they are binding unless overridden by competing principles in a specific situation. The practical work of clinical ethics is frequently the work of navigating conflicts between them. No principle automatically trumps the others: the weight each carries depends on the specifics of the situation, the stakes involved, and the strength of competing considerations.
The most clinically important conflicts include:
Autonomy vs Beneficence — the paternalism problem. When a patient refuses a treatment that the doctor believes is in their best interest, autonomy and beneficence pull in opposite directions. Modern ethics gives priority to autonomy for competent adults. But the doctor must first confirm that the patient has genuine decision-making capacity, has been adequately informed, and is not making the decision under duress or acute psychological distress. If capacity is impaired, beneficence — acting in best interest — takes priority, with the involvement of appropriate surrogates.
Autonomy vs Non-maleficence — the 'harm to self' problem. A patient may autonomously choose an action (refusing a blood transfusion for religious reasons; continuing to drive despite early dementia) that risks harm to themselves or others. The doctor's obligation under non-maleficence conflicts with their duty to respect the patient's choice. Resolution depends on the severity and directness of the harm, whether third parties are at risk, and the legal framework in the specific jurisdiction.
Beneficence vs Justice — the resource allocation problem. A doctor wants to do everything possible for each individual patient (beneficence), but doing so may consume resources that are needed by other patients (justice). The intensive care doctor who must decide whether to continue ventilating a patient with no realistic chance of recovery — while other patients need the ventilator — faces this conflict directly. Neither principle can be applied in isolation.
| Principle | Definition | Core Clinical Application | Key Limits |
|---|---|---|---|
| Autonomy | Patient's right to self-determination | Informed consent, refusal of treatment, confidentiality | Incompetence, harm to others, genuine emergencies |
| Non-maleficence | Obligation to avoid causing harm | Risk-benefit assessment, minimise side-effects | Cannot avoid all harm; must be balanced against benefit |
| Beneficence | Obligation to act in patient's best interest | Active promotion of welfare, referral, advocacy | Must not override patient's own values (paternalism) |
| Justice | Fair treatment and equitable resource allocation | Triage, public health policy, non-discrimination | Requires fair procedures; does not require equal outcomes |
The four-principle approach does not resolve all ethical problems — it provides a structured framework for identifying, articulating, and reasoning through them. In genuine hard cases, it may not yield a single unambiguous answer, but it ensures that all relevant moral considerations have been identified and weighed.
SELF-CHECK
Which bioethics principle is MOST directly associated with the legal requirement for informed consent before a surgical procedure?
A. Justice
B. Non-maleficence
C. Beneficence
D. Respect for autonomy
Reveal Answer
Answer: D. Respect for autonomy
Informed consent is the legal operationalisation of respect for autonomy — the patient's right to make an informed decision about what happens to their body. The consent process ensures the patient has adequate information, understands it, has decision-making capacity, and gives agreement voluntarily. Non-maleficence requires that the risks be disclosed (part of the information), but the consent requirement itself is grounded in autonomy.
Applied Practice: Case-Based Reasoning with the Four Principles
The four-principle framework is most valuable when applied to concrete cases. Consider the following worked examples that illustrate how the principles interact in practice.
Case 1: The Jehovah's Witness patient. A 28-year-old Jehovah's Witness is admitted with a ruptured spleen after a road traffic accident. She is conscious, fully oriented, and refuses blood transfusion on religious grounds. The surgical team states she will likely die without transfusion during the splenectomy. She has signed an advance directive refusing transfusion.
Analysis: Autonomy — she is competent, informed, and her refusal is consistent, voluntary, and supported by an advance directive. Beneficence — surgery and transfusion would maximise her chance of survival. Non-maleficence — death is the harm of not transfusing; transfusion violates her religious integrity and autonomy (a different kind of harm). Justice — other patients are not affected.
Resolution: Modern ethics and Indian case law (though the law is not definitively settled for all cases) support honouring the competent adult's informed refusal even at risk of death. The surgeon should document the conversation thoroughly, ensure capacity, and respect the refusal. Bloodless surgical techniques should be maximised.
Case 2: The confused elderly patient. A 78-year-old man with moderate dementia is admitted with a hip fracture. His daughter, who holds no formal legal authority, insists that he be 'kept comfortable only' and not operated on, as she says 'he wouldn't want this.' The surgical team believes surgery would significantly reduce his pain and improve his function.
Analysis: Autonomy — the patient cannot give informed consent (impaired capacity); the daughter has no legal authority as substitute decision-maker in India (unlike some jurisdictions). Beneficence — surgery is likely in his best interest clinically. Non-maleficence — surgery carries surgical risks, but non-surgical management means ongoing pain. Justice — not directly applicable.
Resolution: In the absence of capacity and formal advance directives or legal guardianship, the treating team must act in the patient's best interest, guided by available information about his prior expressed wishes. The daughter's input is relevant but not legally determinative. The hospital ethics committee should be consulted for significant decisions.
Steps for applying the four principles to any clinical scenario:
1. Identify the relevant facts — diagnosis, prognosis, treatment options, the patient's capacity and expressed wishes
2. Identify which principles are in tension — autonomy, non-maleficence, beneficence, justice
3. Assess the weight of each — what are the stakes? how strong is the autonomy claim? how clear is the harm?
4. Consider legal and institutional context — what does Indian law require in this situation?
5. Document the reasoning — not just the decision, but why it was reached
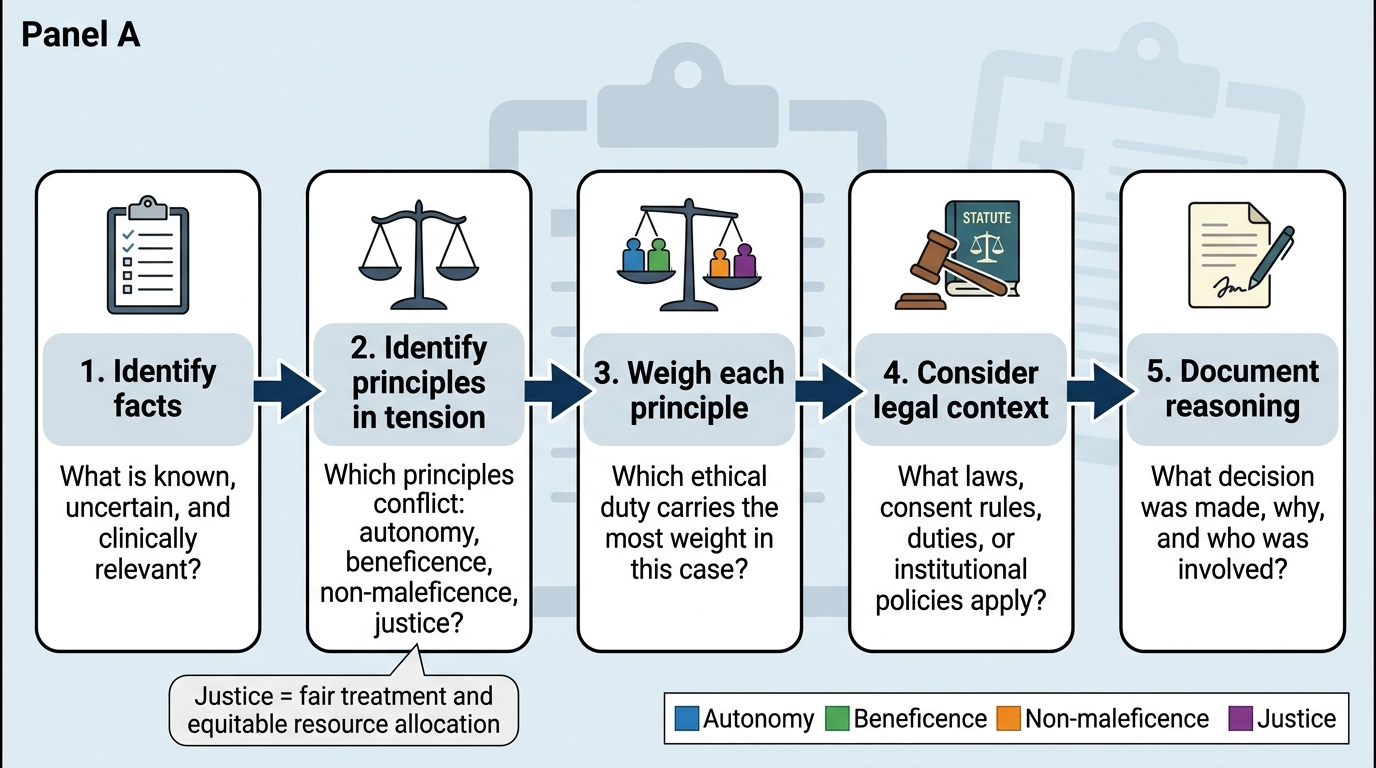
Five-Step Clinical Ethics Reasoning Process
SELF-CHECK
In the Beauchamp and Childress four-principle framework, 'justice' in the clinical context primarily refers to:
A. The legal right of doctors to practise without undue interference
B. The obligation to report crimes committed by patients to the police
C. Fair and equitable treatment of patients and distribution of healthcare resources
D. The duty to provide the highest standard of care to every individual patient
Reveal Answer
Answer: C. Fair and equitable treatment of patients and distribution of healthcare resources
In bioethics, justice refers primarily to distributive justice — the fair allocation of healthcare resources and equitable treatment of patients. It addresses questions like: who gets a scarce ICU bed, how should limited medicines be allocated, does every patient receive equal treatment regardless of socioeconomic status? The obligation to provide the highest standard of care to every patient is beneficence. Reporting crimes is a legal duty, not a justice principle in the bioethics sense.
CLINICAL PEARL
Autonomy is the principle most likely to create discomfort for doctors trained in a paternalistic tradition — and that discomfort is worth examining. When a patient makes a decision you believe is wrong, the instinct to override it is often framed as 'beneficence' (acting in their best interest). But genuine beneficence, as Beauchamp and Childress emphasise, must be shaped by the patient's own values and goals — not just by the doctor's clinical judgment of what is medically optimal. The therapeutic question is not 'what would produce the best outcome by my criteria?' but 'what outcome matters most to this patient, given what they value about their life?' This shift — from technical to patient-centred beneficence — is one of the most important intellectual moves in modern medicine.