Page 1 of 18
FM10.18 | Medical Negligence — SDL Guide
Learning Objectives
- Define medical negligence and distinguish it from maloccurrence and misadventure
- Classify negligence into civil, criminal, contributory, corporate, and vicarious liability
- Explain the legal doctrine of Res Ipsa Loquitur and its three requisite elements
- Identify defences available to a practitioner in negligence litigation
- Describe preventive strategies to reduce medico-legal risk in clinical practice
INSTRUCTIONS
Medical negligence is the most consequential legal risk facing a practising clinician in India. A single negligence claim can end a career, result in criminal prosecution under IPC 304A, or attract substantial civil compensation. Understanding the legal framework is not an academic exercise — it is a professional survival skill that every doctor must command before entering clinical practice.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old patient is admitted for elective laparoscopic cholecystectomy at a private hospital. The surgery is performed by a senior surgeon, but during the procedure the common bile duct is inadvertently injured. Post-operative jaundice develops; a second operation is required, and the patient suffers prolonged morbidity. The patient's family files a complaint before the State Medical Council and simultaneously lodges a civil suit claiming Rs 50 lakhs compensation. The surgeon argues the bile duct injury is a recognised complication in 0.3–0.6% of laparoscopic cholecystectomies and that he followed standard technique. The Consumer Forum disagrees and awards partial compensation.
Was this medical negligence? What is the difference between a known complication and negligence? Which legal doctrines govern this dispute, and what defences were available?
WHY THIS MATTERS
India reports over 5,000 negligence cases annually before consumer courts and civil courts, and criminal prosecutions under IPC 304A (causing death by negligence) are increasing. The Supreme Court's Jacob Mathew v State of Punjab (2005) ruling fundamentally reshaped the threshold for criminal negligence by doctors. Without a precise understanding of negligence law, a clinician cannot give informed consent to patients, document findings adequately, or defend a complaint. The NMC 2024 curriculum mandates FM10.18 precisely because negligence literacy is a core professional competency — not a luxury elective.
RECALL
Before proceeding, recall these prior concepts:
- Duty of care — the legal obligation a clinician assumes when a doctor–patient relationship is formed. Recall from your earlier FM ethics units.
- Standard of care — the level of skill and judgment expected of a reasonably competent doctor in the same specialty and circumstances.
- Causation — in law, the principle that a breach must be shown to have caused the harm (the 'but-for' test).
- IPC 304A — criminal provision: 'whoever causes death of any person by doing any rash or negligent act not amounting to culpable homicide'. Recall from your criminal law FM sessions.
- Consumer Protection Act 2019 — medical services are covered; distinguish from civil tort liability.
Defining Negligence: Legal and Professional Context
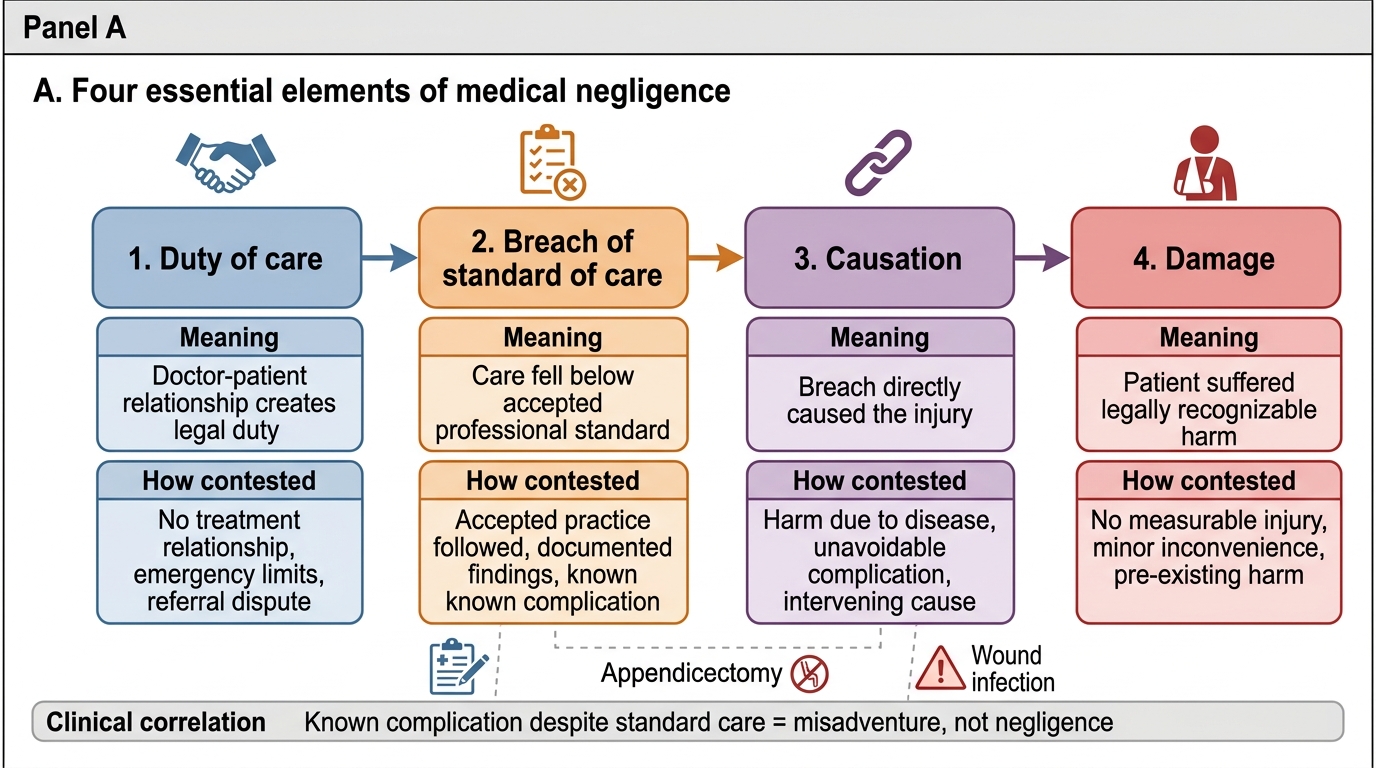
Medical negligence is the failure of a medical practitioner to provide the standard of care that a reasonably competent practitioner in the same field would provide under similar circumstances, resulting in harm to the patient. This definition embeds four essential elements — duty, breach, causation, and damage — each of which must be established for a successful negligence claim. The practitioner who owed no duty (no doctor–patient relationship existed) cannot be found negligent; equally, a breach that caused no harm produces no legal liability.
It is critical to distinguish three concepts that are often conflated but carry entirely different legal consequences. Negligence is a below-standard act or omission — the clinician departed from acceptable practice. Misadventure (also called therapeutic misadventure) is an unforeseen adverse outcome that occurred despite the clinician adhering to standard care — the standard was met but the outcome was bad. Maloccurrence is a bad outcome with no negligence element — complications that are inherent risks of the procedure performed correctly. A bile duct injury during technically standard laparoscopic cholecystectomy is a misadventure, not negligence; a bile duct injury caused by the surgeon's failure to identify the critical view of safety before clipping is negligence.
The concept of standard of care in India is governed by the Bolam test (from Bolam v Friern Hospital Management Committee [1957] 1 WLR 582, adopted by Indian courts): a doctor is not negligent if he acts in accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art, even if another body of medical opinion would have done differently. The Bolitho modification (from Bolitho v City and Hackney HA [1997]) adds a second requirement: the medical opinion must also be logically defensible — it is not enough to show that some body of professionals did it; those professionals must be able to give a rational account of why.
Key legal landmarks in India:
- Jacob Mathew v State of Punjab (2005): Supreme Court held that for criminal negligence under IPC 304A, the standard is gross negligence — mere lack of skill or an error of judgment is insufficient for criminal liability; the negligence must be of a very high degree.
- Indian Medical Association v V P Shantha (1995): Supreme Court confirmed medical services fall under the Consumer Protection Act (then 1986, now 2019), placing doctors within consumer court jurisdiction.
Essential Elements of Medical Negligence
SELF-CHECK
A surgeon performs an appendicectomy. During the procedure, he correctly identifies all anatomical landmarks and follows standard technique, but the patient develops a wound infection post-operatively. The surgeon had documented his findings. Under which category does this outcome MOST appropriately fall?
A. Medical negligence
B. Misadventure
C. Res Ipsa Loquitur
D. Vicarious liability
Reveal Answer
Answer: B. Misadventure
A wound infection following a technically correct appendicectomy with standard precautions is a known complication — an unforeseen adverse event occurring despite standard care. This is misadventure (therapeutic misadventure), not negligence. Negligence requires a departure from the standard of care that causes harm. Res Ipsa Loquitur is a doctrine applicable when negligence is self-evident from the facts. Vicarious liability is about employer–employee responsibility, not about categorising the outcome itself.
Classification of Medical Negligence
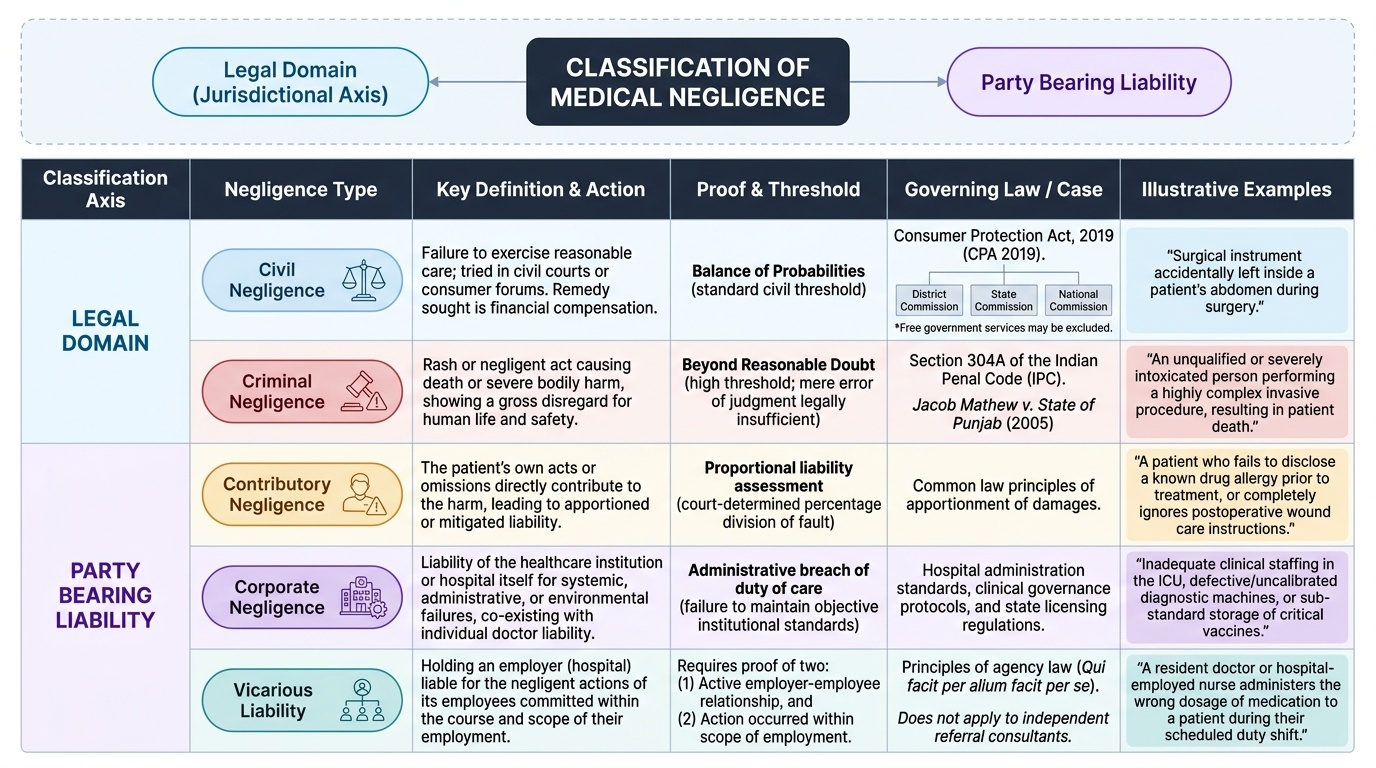
Negligence in medical practice is classified along two principal axes: the legal domain (civil versus criminal) and the party bearing liability (direct, contributory, corporate, or vicarious). Understanding these classifications determines which court has jurisdiction, what standard of proof applies, and who ultimately pays compensation.
Civil negligence is tried in civil courts or consumer forums. The standard of proof is the balance of probabilities. Remedies are compensatory — money damages. Under the Consumer Protection Act 2019 (CPA 2019), a patient may file a complaint before a District Commission, State Commission, or National Commission depending on the compensation sought. Medical services rendered free of cost at hospitals receiving government funding may be excluded from CPA 2019 jurisdiction (a contested area post-2019 Act).
Criminal negligence is prosecuted under IPC 304A (causing death by a rash or negligent act). The standard of proof is beyond reasonable doubt. The threshold for criminal liability is significantly higher than civil liability: following Jacob Mathew (2005), the negligence must be so gross and culpable that it shows utter disregard for human life. An error of judgment or an unfortunate complication does not meet this threshold.
Contributory negligence arises when the patient's own conduct contributed to the harm — for example, a patient who fails to disclose a known allergy, ignores post-operative instructions, or delays seeking care when warned to return. Courts may apportion liability proportionally.
Corporate negligence is the liability of the hospital or healthcare institution itself — for systemic failures such as poor maintenance of equipment, inadequate staffing, failure to credentialize physicians, or defective drug storage. It is distinct from the individual doctor's liability and may coexist with it.
Vicarious liability imposes liability on an employer for negligent acts of an employee performed in the course of employment. A hospital is vicariously liable for a resident's negligent act committed while on duty. The key requirement is that (a) an employer–employee relationship existed and (b) the negligent act occurred within the scope of employment. An independent consultant on a purely referral basis may not trigger vicarious hospital liability.
Provided image
Res Ipsa Loquitur: The Self-Speaking Evidence Doctrine
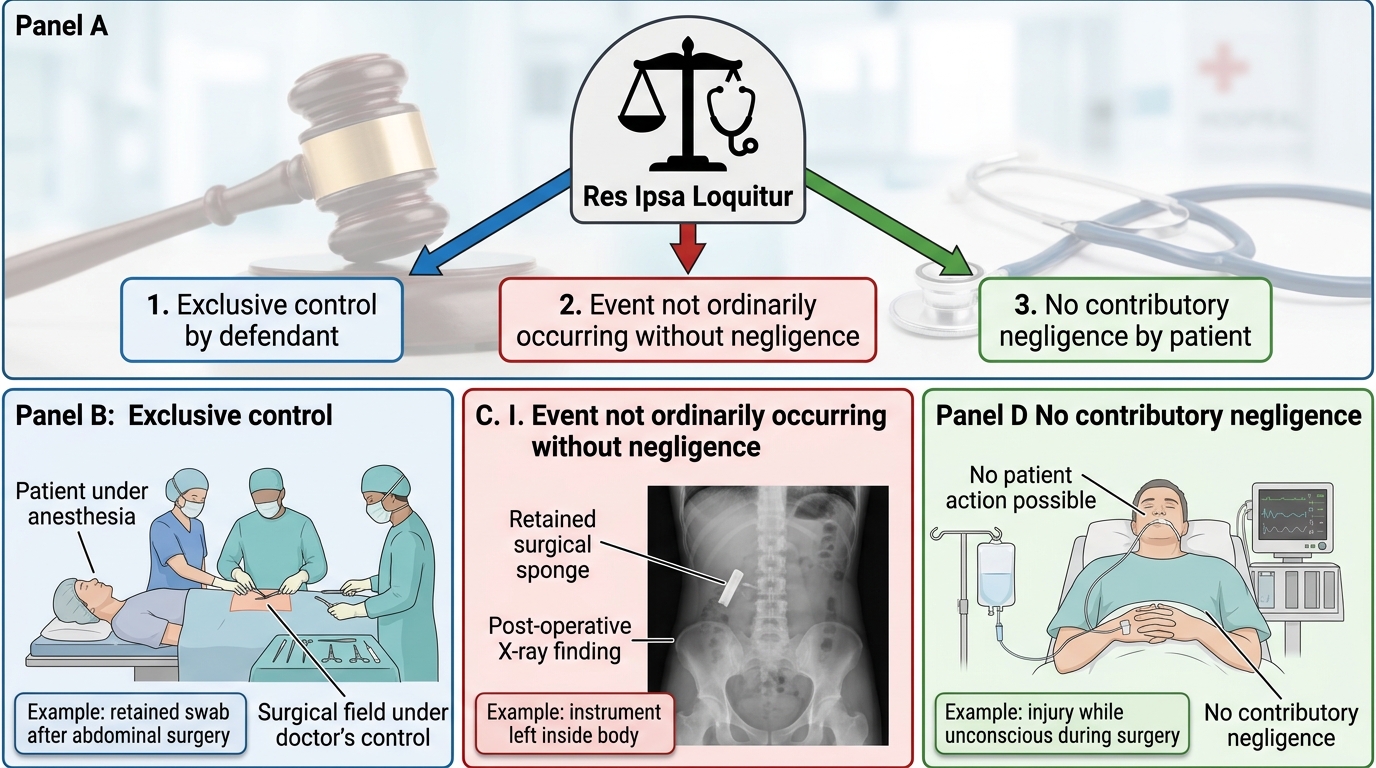
Res Ipsa Loquitur — Latin for 'the thing speaks for itself' — is a legal doctrine that permits a court to infer negligence from the very nature of the occurrence, without direct evidence of how the defendant acted. It is an evidential rule that shifts the burden of explanation to the defendant once the claimant establishes the doctrine's three prerequisite elements.
The three requirements of Res Ipsa Loquitur are:
1. The act or omission was under the exclusive management and control of the defendant (or those for whom the defendant is responsible) at the time of the accident. If the patient or a third party had intervening control, the doctrine is inapplicable.
2. The accident is of a type that does not ordinarily occur without negligence — i.e., in the absence of negligence, this would not have happened. The classic medical example is a swab or instrument left inside a patient post-operatively — this does not happen absent some failure.
3. There was no contributory negligence by the patient — the patient's conduct did not itself cause or contribute to the injury.
Classic examples in medical practice: a foreign body (surgical swab, clamp) left inside a body cavity post-operatively; performing surgery on the wrong site or wrong patient; a patient receiving the wrong blood group during transfusion; an operation on a non-consenting patient when consent was clearly withheld.
Important nuance: Res Ipsa Loquitur does NOT make the defendant automatically liable. It shifts the evidential burden — the defendant must come forward with an explanation showing that the harm occurred without negligence on their part. If the defendant can provide a satisfactory explanation, the burden reverts to the claimant. The doctrine is a procedural tool, not a finding of liability.
Three Conditions for Res Ipsa Loquitur in Medical Negligence