Page 2 of 18
FM10.18 | Medical Negligence — SDL Guide (Part 2)
Documentation, Prevention, and Defences in Negligence Litigation
Good documentation is the single most powerful defence in any negligence proceeding. The medical record is the contemporaneous account of what was found, what was decided, and why — and it is treated by courts as the most reliable evidence of the standard of care applied. In practice, clinical documentation serves three functions in a negligence context: it proves the clinician's thought process, demonstrates informed consent was obtained, and records that post-procedure monitoring was conducted. Incomplete or post-hoc altered records raise a presumption of concealment and may destroy an otherwise valid defence.
Key documentation standards in FM10.18 practice:
- Record the clinical indication for every intervention clearly in the notes.
- Obtain and document informed consent in writing, including disclosure of material risks, alternatives, and the patient's questions and responses.
- Document the standard technique used — instrument checks, swab counts (particularly in open surgical procedures), and the outcome of the procedure.
- Record any complication, its timing, and the clinical response immediately — delayed or sanitised documentation of complications is a red flag in litigation.
- Maintain legible, dated, timed, and authenticated records.
Defences available in negligence litigation:
- Standard of care defence: demonstrate adherence to an accepted and logically defensible body of practice (Bolam + Bolitho). Expert witness testimony is key.
- No causation defence: the breach, even if established, did not cause the harm complained of ('but-for' causation absent).
- Contributory negligence: the patient's own conduct contributed materially to the harm; compensation is apportioned accordingly.
- Res Judicata / limitation: the claim is time-barred (Consumer Protection Act 2019 — 2-year limitation from date cause of action arose; Civil courts — 3 years under Limitation Act).
- No duty of care: no doctor–patient relationship was formed; the treating duty was never assumed.
- Good Samaritan / emergency exception: Section 134A of the Motor Vehicles Act (amended 2019) provides limited protection to persons rendering emergency care at road accident scenes in good faith — a narrow but important practical defence.
Prevention strategies:
- Adhere strictly to standard operating procedures (SOPs) for high-risk procedures.
- Perform regular audit and morbidity/mortality review meetings to identify system risks before they cause harm.
- Maintain current professional indemnity insurance (Medical Indemnity Insurance — see FM10.21).
- Obtain valid informed consent before every invasive procedure — verbal for minor interventions, written for operations, anaesthesia, and procedures with significant risk.
- Foster a culture of open disclosure: patients who are informed promptly about an adverse event and offered an apology are demonstrably less likely to litigate.
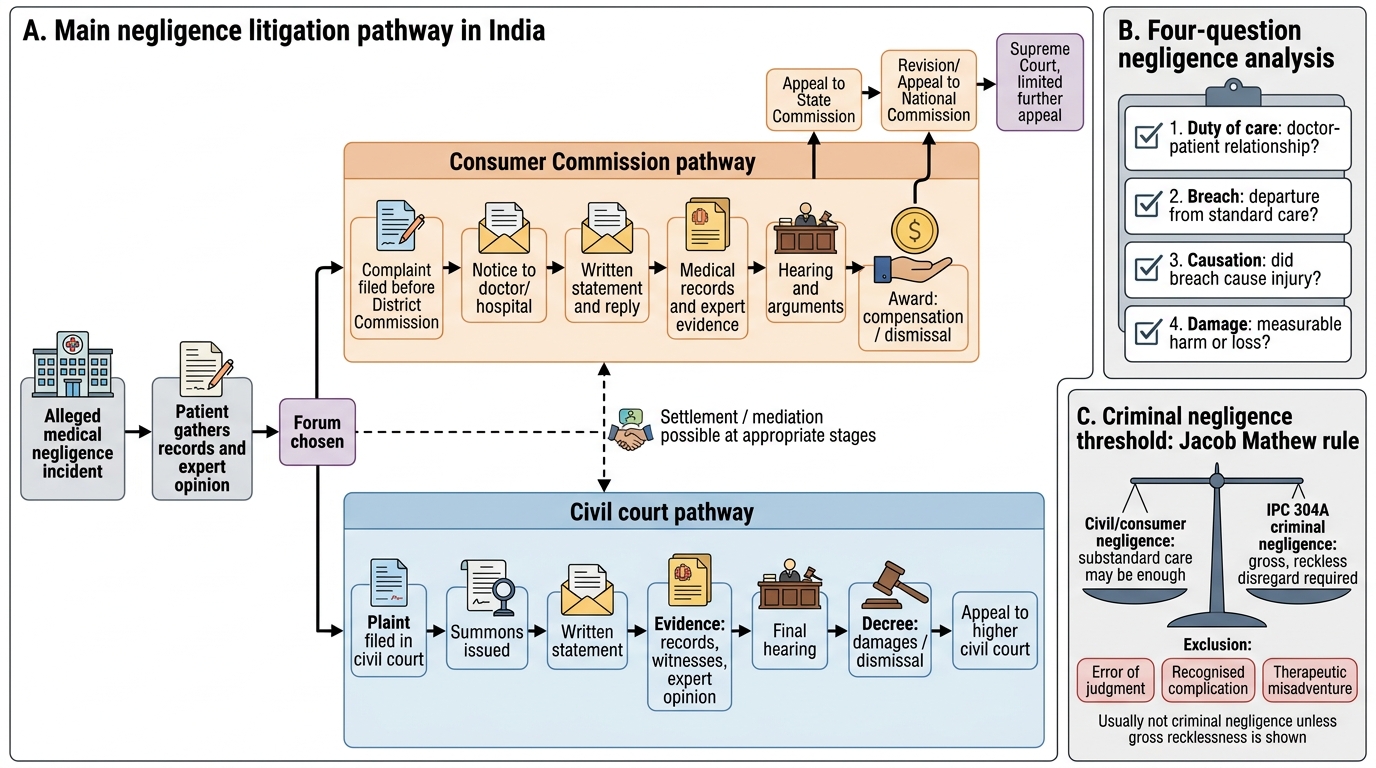
Negligence Litigation Pathway in India
CLINICAL PEARL
The Jacob Mathew rule for criminal negligence: After Jacob Mathew v State of Punjab (2005), courts require that for IPC 304A prosecution of a doctor, the negligence must be gross — so egregious that it reflects utter disregard for patient life. An error of clinical judgment, a recognised complication of a technically-performed procedure, or a therapeutic misadventure does NOT meet the criminal threshold. In practice, this means criminal cases require (a) a specific identifiable departure from standard care and (b) evidence that the departure was reckless rather than merely substandard. The Jacob Mathew principle effectively raised the bar for criminal prosecution and is the cornerstone of every criminal negligence defence.
Applied Practice: Analysing a Negligence Complaint
When a clinician or a hospital faces a negligence complaint — whether before a Consumer Commission, the State Medical Council, or a criminal court — a structured four-question analysis should be applied to determine the strength of the claim and the appropriate response.
Step 1 — Establish the duty of care: Was a doctor–patient relationship formed? Did the clinician accept responsibility for treating this patient? This is rarely disputed in in-patient cases but may arise in casual consultations, telephone advice, or Good Samaritan scenarios.
Step 2 — Identify the alleged breach: What specific act or omission is said to have fallen below the standard of care? Map it to the Bolam test: can the defendant show that a responsible body of opinion would have acted the same way, AND that this opinion is logically defensible (Bolitho)?
Step 3 — Test causation: Even if a breach occurred, did it cause this specific harm? A common defence is that the harm would have occurred regardless — e.g. the patient's underlying disease was the proximate cause, not the clinician's error.
Step 4 — Assess damages: What harm was caused? Is the harm directly attributable to the breach? Courts assess compensation under heads of loss: medical expenses, pain and suffering, loss of earnings, and future care costs.
Practical worked example: A patient is prescribed gentamicin for a urinary tract infection. No baseline renal function was tested. The patient develops acute kidney injury. Analysis: (1) Duty — clearly established. (2) Breach — failure to check renal function before prescribing a nephrotoxic drug with a narrow therapeutic index may fall below the standard of a reasonably competent physician. (3) Causation — the AKI is temporally and clinically linked to gentamicin; evidence of existing renal impairment would need to be considered. (4) Damages — dialysis costs, hospital admission, residual CKD. This case is likely to establish negligence in a civil forum. Whether it meets the criminal threshold depends on whether the prescribing was reckless rather than merely negligent.
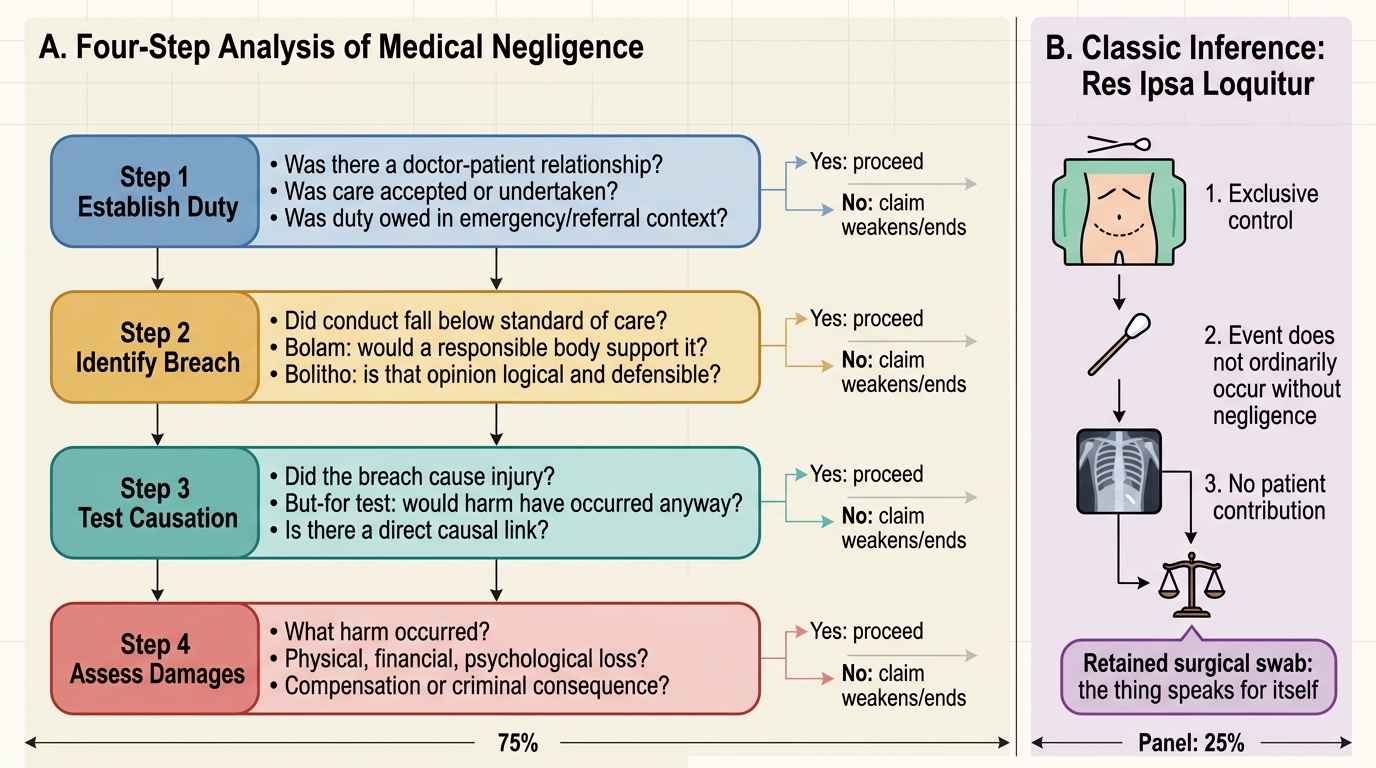
Four-Step Analysis of Medical Negligence
SELF-CHECK
A patient files a consumer complaint against a gynaecologist alleging negligence during a hysterectomy. A post-operative X-ray reveals a surgical swab inside the abdomen. The gynaecologist argues she cannot be held liable without direct evidence of her intra-operative conduct. Which legal doctrine BEST applies to rebut the surgeon's argument?
A. Contributory negligence
B. Vicarious liability
C. Res Ipsa Loquitur
D. Standard of care defence
Reveal Answer
Answer: C. Res Ipsa Loquitur
A retained surgical swab inside the abdomen after surgery is the classic example of Res Ipsa Loquitur ('the thing speaks for itself'). All three elements are satisfied: (1) the abdominal cavity was under the surgeon's exclusive control during the procedure; (2) a retained swab does not ordinarily occur without negligence (swab counts are a standard safety protocol); (3) there is no suggestion of patient contributory negligence. The doctrine allows the court to infer negligence without direct evidence of the intra-operative act, shifting the explanatory burden to the surgeon.
SELF-CHECK
Under the Jacob Mathew v State of Punjab (2005) Supreme Court ruling, which standard of negligence is required for a doctor to be prosecuted under IPC 304A?
A. Any departure from standard of care that results in death
B. Gross negligence — a very high degree of recklessness showing utter disregard for patient life
C. The Bolam test — failure to meet any accepted body of practice
D. Contributory negligence by the patient must be excluded first
Reveal Answer
Answer: B. Gross negligence — a very high degree of recklessness showing utter disregard for patient life
The Supreme Court in Jacob Mathew v State of Punjab (2005) held that for criminal prosecution under IPC 304A, mere lack of skill or an error of judgment is insufficient. The negligence must be gross — of a very high degree reflecting utter disregard for patient life. This is a significantly higher threshold than civil negligence (balance of probabilities, Bolam test). The ruling was designed to protect doctors from criminal prosecution for honest clinical errors while preserving liability for genuinely reckless acts.