Page 12 of 17
FM8.15-16 | Abortion & the MTP Act — SDL Guide
Learning Objectives
- Classify abortion (spontaneous, induced — therapeutic/criminal, missed, incomplete, inevitable, septic)
- Describe the methods used for MTP at different gestational stages
- Explain the MTP Act 2021 with its amendments — including the extended gestational limits and categories of survivors eligible for termination up to 24 weeks
- Describe the evidence of abortion in living and dead women and the methods used in criminal abortion
- State the doctor's duties in cases of criminal abortion and investigations of death from criminal abortion
INSTRUCTIONS
Abortion occupies a critical intersection of law, ethics, and clinical medicine in India. The Medical Termination of Pregnancy (MTP) Act was enacted in 1971 and significantly amended in 2021. The 2021 amendment extended gestational limits for specific vulnerable categories and updated provider eligibility. This module covers both the clinical and the forensic aspects — what abortion is, how it is performed, what signs it leaves, and how the law governs it.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl who was raped and is now 21 weeks pregnant presents seeking termination. A 28-year-old woman presents at 23 weeks with a diagnosis of Trisomy 18 on amniocentesis. A 32-year-old woman presents with signs of septicaemia; on examination there is evidence of an attempted termination by an unqualified person using an unsterile instrument. Three presentations, three different legal and clinical pathways, all governed by the MTP Act and its 2021 amendment.
WHY THIS MATTERS
India was among the first countries in the world to legalise abortion (MTP Act 1971), yet unsafe abortion remains a significant cause of maternal mortality. The clinical and legal framework governs who may perform abortion, under what circumstances, up to what gestational age, and with what documentation. The forensic aspects — recognising signs of illegal abortion, the methods used, and the doctor's duties — are equally important because criminal abortion deaths present to emergency facilities and to the post-mortem room.
RECALL
From obstetrics: recall that termination methods differ by gestational age — medical methods (mifepristone + misoprostol) are safe up to 9-10 weeks; surgical methods (suction evacuation) for first trimester; dilatation and evacuation (D&E) or induction of labour for second trimester. From MTP Act basics: you may have encountered the original 1971 provisions (up to 20 weeks gestational limit). The 2021 amendment is the current law — always cite 2021 provisions, not 1971 original.
Classification of Abortion
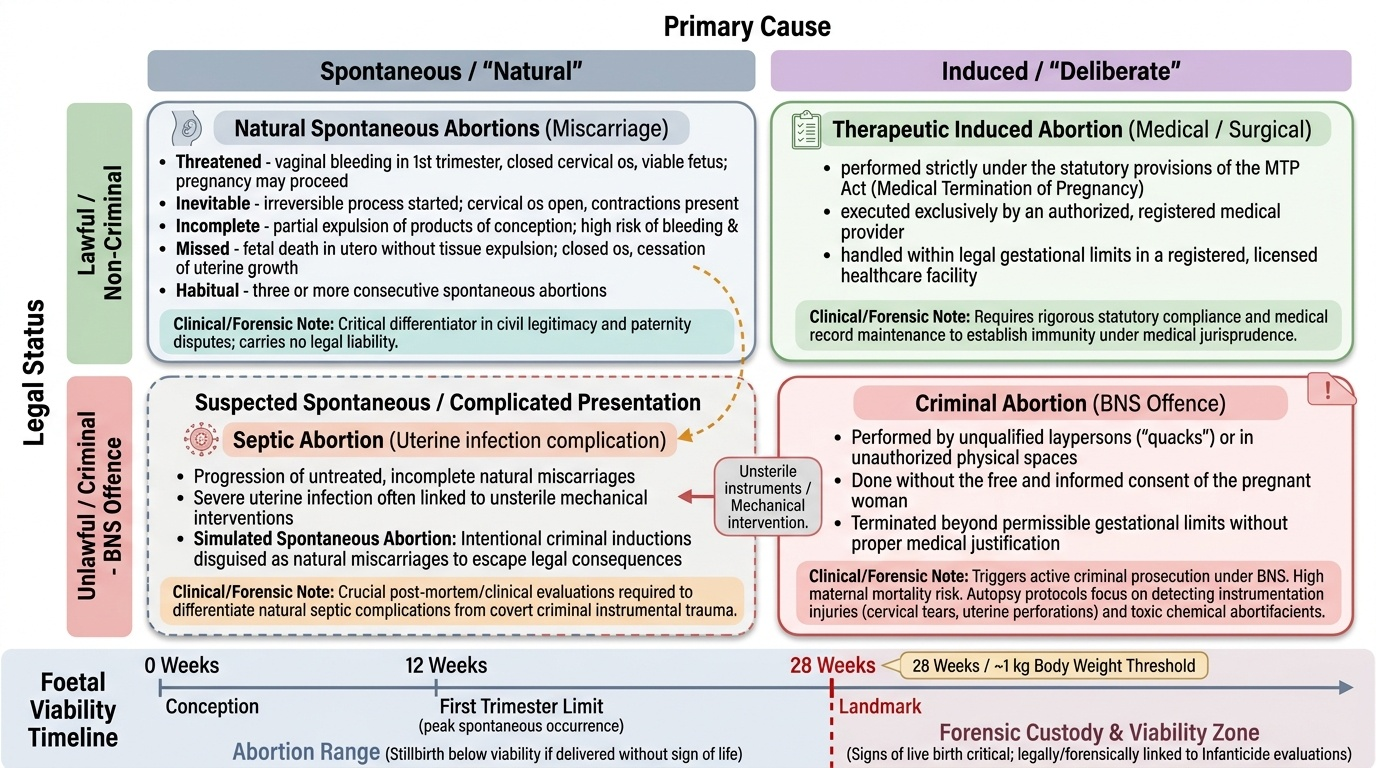
Abortion refers to the expulsion or extraction of the products of conception before viability. In Indian legal context, the foetal viability threshold is 28 weeks (approximately 1 kg body weight) — a foetus delivered before 28 weeks with no signs of life is generally considered a stillbirth below viability; above 28 weeks, signs of live birth become legally and forensically critical (see so11-infanticide SDL).
Abortions are classified along two dimensions: the primary cause and the clinical presentation.
By cause:
- Spontaneous abortion (miscarriage): Occurs naturally without intervention; most common in the first trimester (chromosomal abnormalities are the leading cause). Not a criminal matter.
- Induced abortion: Deliberate termination of pregnancy. Two subcategories:
- Therapeutic (lawful): Performed in accordance with the MTP Act by an authorised provider; legal.
- Criminal abortion: Performed in violation of the MTP Act — by an unqualified person, outside a registered facility, beyond the legal gestational limit without proper authorisation, or without the woman's consent. A criminal offence under BNS.
By clinical type:
- Missed abortion: Foetal death in utero without expulsion; the uterus does not enlarge; closed cervical os.
- Incomplete abortion: Partial expulsion of products of conception; retained tissue causes continued bleeding and risk of infection.
- Inevitable abortion: Irreversible process has begun — cervical os open, contractions present.
- Septic abortion: Abortion complicated by uterine infection; may result from criminal abortion using unsterile instruments; life-threatening.
- Habitual abortion: Three or more consecutive spontaneous abortions; an obstetric diagnosis relevant to legitimacy disputes.
- Threatened abortion: Vaginal bleeding in first trimester with a closed os and viable foetus — pregnancy may continue.
Provided image
MTP Act 2021: Current Legal Framework
The Medical Termination of Pregnancy Act, originally enacted in 1971, was substantially amended by the MTP (Amendment) Act 2021 and the MTP Rules 2021. The 2021 amendment is the current operative law. Key provisions:
Provided image
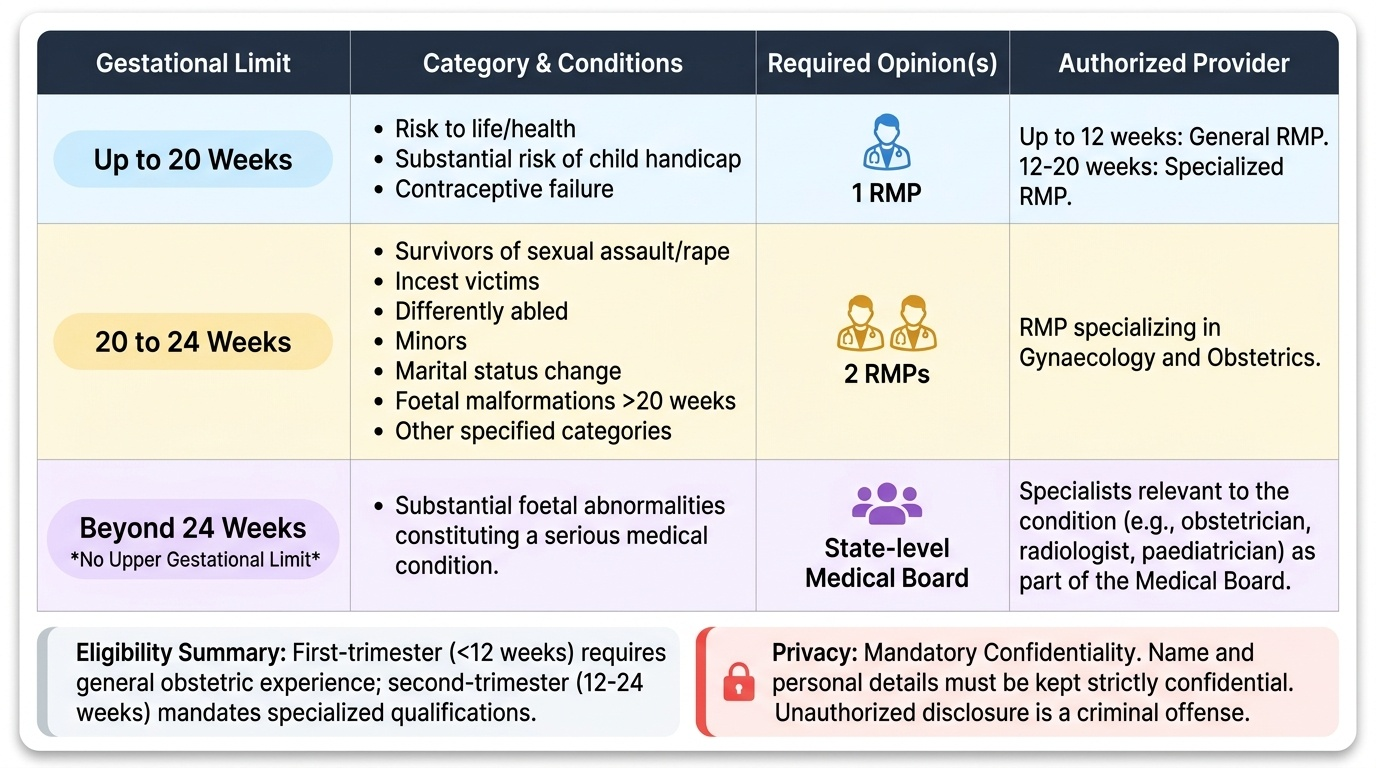
Gestational limits (standard categories — up to 20 weeks):
- Up to 20 weeks gestation: termination may be performed on the opinion of one registered medical practitioner (RMP), on one of three grounds:
1. Continuation of the pregnancy would involve risk to the life of the pregnant woman, or of grave injury to her physical or mental health
2. There is a substantial risk that, if born, the child would suffer physical or mental abnormalities constituting serious handicap
3. Pregnancy resulting from failure of contraceptive method used by a married woman or her husband (for unmarried women: any contraceptive failure)
Extended gestational limit — up to 24 weeks (2021 Amendment — CRITICAL PROVISION):
The 2021 amendment extended the upper limit to 24 weeks for specific categories of survivors, requiring the opinion of two RMPs (not one):
1. Survivors of sexual assault or rape
2. Victims of incest
3. Differently abled women (as per MTP Rules 2021)
4. Minors
5. Change of marital status during ongoing pregnancy (widowhood, divorce)
6. Women with foetal malformations detected after 20 weeks
7. Other categories as specified in MTP Rules 2021
Beyond 24 weeks — substantial foetal abnormalities:
For termination beyond 24 weeks where there is a substantial foetal abnormality, a Medical Board (constituted at every state-level hospital) must opine. The Medical Board includes specialists relevant to the condition (obstetrician, radiologist, paediatrician, etc.). There is no upper gestational limit for Medical Board-approved terminations on foetal abnormality grounds.
Provider eligibility:
- First trimester (up to 12 weeks): any RMP with experience in obstetric practice
- Second trimester (12-20 weeks and 20-24 weeks for eligible categories): RMP with specialisation in gynaecology and obstetrics, or specified equivalent experience
Privacy provision: The 2021 Act added an explicit privacy protection — the name and personal details of a woman who undergoes MTP must be kept confidential; disclosure to any person not permitted by the Act is a criminal offence.
Documentation: The prescribing/performing doctor must maintain prescribed forms. Medical records must be retained for 5 years.
SELF-CHECK
A 17-year-old rape survivor presents at 22 weeks gestation seeking termination. Under the MTP (Amendment) Act 2021, which of the following correctly describes the legal framework?
A. Termination is not possible beyond 20 weeks for any reason
B. Termination is possible up to 24 weeks for rape survivors; requires two registered medical practitioners' opinions; provider must have relevant specialisation
C. Termination requires only one doctor's opinion because she is a minor
D. Termination beyond 20 weeks requires a High Court order for all minors
Reveal Answer
Answer: B. Termination is possible up to 24 weeks for rape survivors; requires two registered medical practitioners' opinions; provider must have relevant specialisation
The MTP Amendment Act 2021 extended the gestational limit to 24 weeks for rape survivors and minors (both apply here). Two RMPs' opinions are required for the 20-24 week window. No court order is needed for terminations within the gestational limit — the Medical Board is required only beyond 24 weeks for foetal abnormalities.
Methods of Abortion: Therapeutic and Criminal
Understanding abortion methods is essential for both clinical practice and forensic recognition — because the method used in a criminal abortion often leaves characteristic physical evidence.
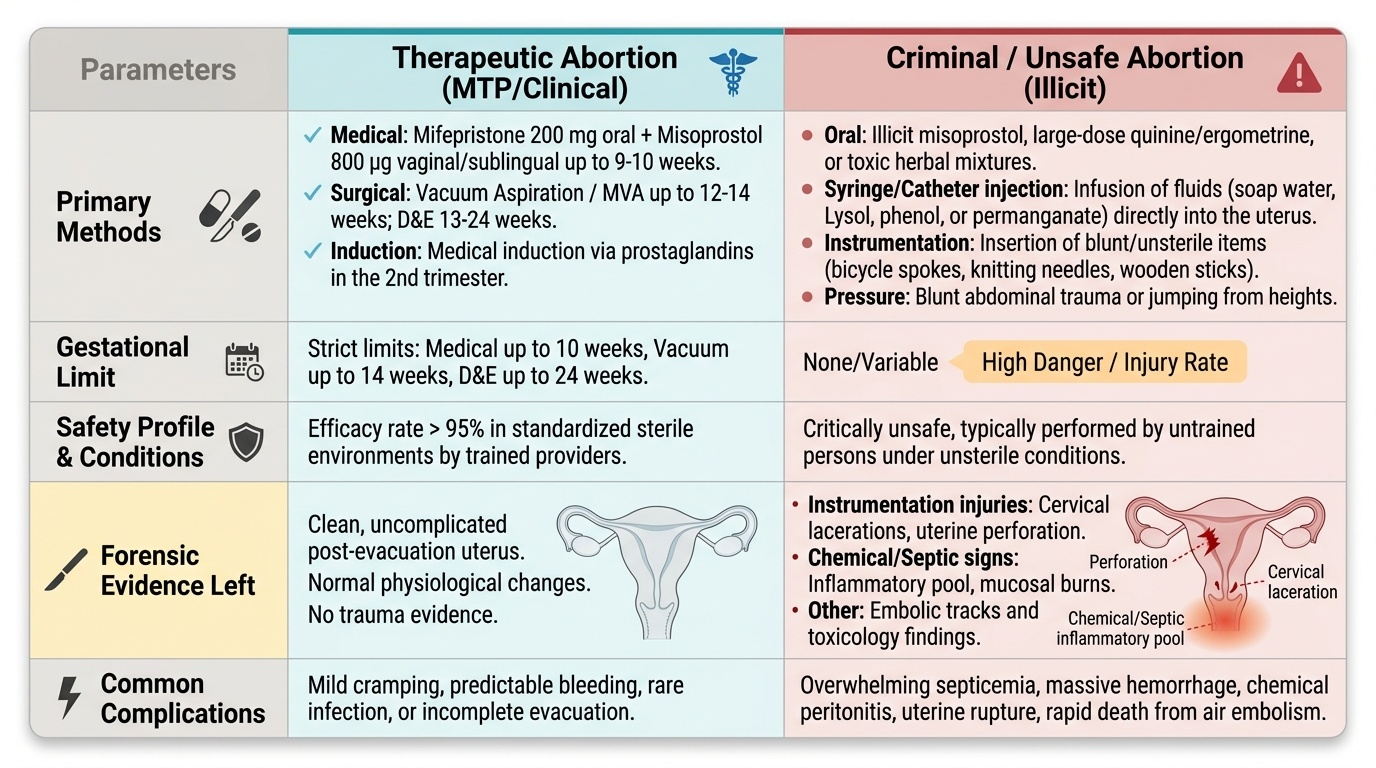
Therapeutic (MTP) methods:
- Medical termination: Mifepristone (antiprogestogen) + misoprostol (prostaglandin E1 analogue) — the combination is approved for termination up to 9-10 weeks. Mifepristone is given first (200 mg orally) followed 24-48 h later by misoprostol (800 μg vaginally or sublingually). Efficacy ≥95% in the first trimester.
- Vacuum aspiration / manual vacuum aspiration (MVA): Suction evacuation; safe for up to 12-14 weeks; performed under paracervical block or general anaesthesia.
- Dilatation and evacuation (D&E): For 13-24 weeks; cervical priming (misoprostol/osmotic dilators) followed by surgical evacuation.
- Medical induction: Prostaglandin induction (misoprostol or other prostaglandins) for mid-trimester terminations — produces uterine contractions and labour.
Criminal abortion methods (from forensic medicine perspective):
Criminal abortion is attempted when a woman cannot or does not wish to obtain legal termination, or when an unqualified person performs it. Methods are typically dangerous:
- Oral abortifacients: Ergometrine, quinine in large doses, misoprostol obtained illicitly, herbal preparations (common in rural India). Signs at post-mortem: gastric mucosal congestion, chemical injury to mucosa, drug traces.
- Syringe/catheter introduction: Introduction of fluids (soapy water, lysol, phenol, lemon juice, permanganate solutions) into the uterus via catheter or syringe. Highly dangerous: septicaemia, air embolism, chemical peritonitis, uterine perforation.
- Instrumentation: Introduction of unsterile metal instruments (bicycle spokes, knitting needles, sticks) into the cervix/uterus. Evidence at examination: cervical lacerations, uterine perforation, peritonitis, septicaemia.
- Pressure methods: External pressure on the abdomen, jumping from heights — largely ineffective and potentially dangerous from the trauma rather than the abortion.
Forensic significance of criminal abortion methods: The method determines the pattern of injury and the cause of death. Instrumentation deaths show cervical/vaginal lacerations and uterine perforation. Chemical method deaths show mucosal burns and systemic toxicity. Air embolism (from syringe injection) causes frothy blood in the heart chambers at post-mortem — a specific finding the forensic pathologist must look for.
Provided image
SELF-CHECK
At post-mortem examination of a woman who died after a suspected criminal abortion, the pathologist finds frothy blood in the right heart chambers on incising the right ventricle under water. What does this indicate?
A. She died from septicaemia following uterine infection
B. She died from air embolism — likely from syringe injection of fluid into the uterus introducing air into the venous circulation
C. The frothy appearance is a post-mortem decomposition artefact
D. She had concurrent pulmonary oedema from fluid overload
Reveal Answer
Answer: B. She died from air embolism — likely from syringe injection of fluid into the uterus introducing air into the venous circulation
Frothy blood in the right heart chambers (the right ventricle technique — incising under water and looking for air bubbles) is the classic post-mortem finding of air embolism. In criminal abortion, this occurs when air is introduced into the venous sinuses of the uterus during syringe/fluid injection. This is a specific and significant finding that must be actively looked for in suspected criminal abortion deaths.
Evidence of Abortion in the Living and Dead; Doctor's Duties
Recognising that abortion has occurred — and whether it was criminal — requires both a systematic clinical examination and knowledge of the legal framework.
Evidence of abortion in the living:
- History of amenorrhoea (pregnancy) followed by vaginal bleeding and expulsion or attempted expulsion
- Uterine size discrepancy (uterus smaller than expected for gestational age if incomplete or recent complete abortion)
- Dilated and softened cervix, blood-stained discharge
- Retained products of conception on ultrasound
- Signs of complication: fever, peritonism (septicaemia), cervical shock (vasovagal from instrumentation), signs of chemical burn if chemical abortifacients used
- Specific examination findings suggesting instrumentation: cervical lacerations, uterine tenderness, peritonitis
Evidence of abortion in the dead:
- Uterus shows signs of recent pregnancy: placental site, decidua, haemorrhage
- Products of conception (foetal remnants) in uterus if incomplete
- Signs of the abortion method: cervical/uterine lacerations (instrumentation), mucosal burns (chemical), frothy cardiac blood (air embolism), peritonitis (septicaemia)
- Toxicological evidence from blood and gastric contents (oral abortifacients)
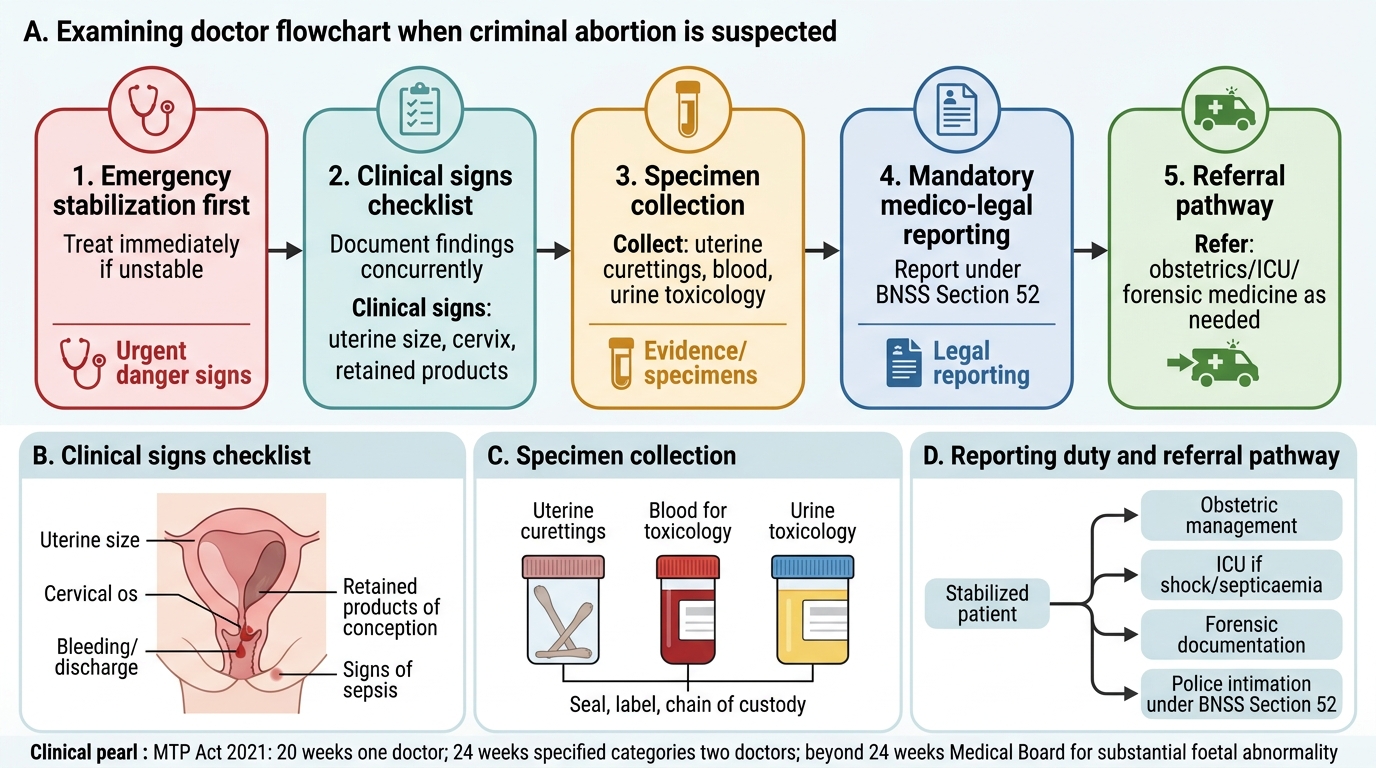
Doctor's duties in criminal abortion:
1. Treat the woman — her life takes priority over any investigation. Do not withhold treatment to preserve evidence.
2. Document injuries and findings accurately — describe every finding that might indicate method used.
3. Collect and preserve evidence — blood for toxicology, vaginal swabs if chemical agent suspected, photography of injuries.
4. Report to police under BNSS Section 52 — injuries from criminal abortion constitute an offence; mandatory reporting applies.
5. Maintain patient confidentiality — the woman's identity is protected by the MTP Act's privacy provisions; however, the mandatory reporting duty to police under BNSS takes precedence over confidentiality where a criminal offence has occurred.
6. Do not name the abortionist based on the woman's statement — record her account verbatim as history; it is hearsay evidence. The police will investigate.
Dying declaration: If the woman's condition is critical and unlikely to survive, her statement about who performed the abortion should be recorded as a dying declaration (with a magistrate if possible; in emergency, before any competent witness including a doctor). A dying declaration is admissible as evidence in Indian law.
Doctor’s Flowchart for Suspected Criminal Abortion
CLINICAL PEARL
The most important MTP Act 2021 exam facts: (1) standard upper limit = 20 weeks (one doctor); (2) extended limit = 24 weeks for rape survivors, incest survivors, minors, differently abled women, and women with change of marital status — two doctors required; (3) beyond 24 weeks = Medical Board for substantial foetal abnormalities only. Always cite the MTP Amendment Act 2021, not the 1971 original. Many textbooks still cite the pre-2021 framework.
SELF-CHECK
A woman arrives at the emergency department after what appears to be an illegal abortion performed by a village midwife. She has signs of septicaemia and is haemodynamically compromised. The police call asking for a statement. The correct immediate action is:
A. Give the police a statement before treating the patient — evidence must be preserved first
B. Refuse all interaction with police until the patient is stable
C. Treat the woman immediately; concurrently document clinical findings; report to police under BNSS Section 52; collect blood for toxicology once treatment is initiated
D. Delay treatment until a magistrate arrives to record a dying declaration
Reveal Answer
Answer: C. Treat the woman immediately; concurrently document clinical findings; report to police under BNSS Section 52; collect blood for toxicology once treatment is initiated
Treatment is the immediate priority. Evidence collection (blood for toxicology, documentation of injuries) proceeds concurrently with treatment — it does not require delay. BNSS Section 52 reporting is mandatory. A dying declaration should be recorded if the patient's condition is critical and she is conscious — but this is done by a magistrate/witness, not by delaying treatment.
KEY TAKEAWAYS
Abortion is classified as spontaneous or induced (therapeutic/criminal). Clinical types: missed, incomplete, inevitable, septic, habitual, threatened. MTP Act 2021: up to 20 weeks — one doctor's opinion; up to 24 weeks for specific survivor categories (rape, incest, minors, differently abled, change of marital status, foetal malformations) — two doctors' opinions; beyond 24 weeks for substantial foetal abnormality — Medical Board required. MTP methods: mifepristone+misoprostol (up to 9-10 weeks), vacuum aspiration (up to 12-14 weeks), D&E, induction for later terminations. Criminal abortion methods: oral abortifacients, syringe/fluid injection (air embolism risk), instrumentation (cervical/uterine lacerations). Doctor's duties: treat first; document; collect evidence; report under BNSS Section 52; record dying declaration if indicated.
REFLECT
A woman who is 23 weeks pregnant presents stating she was sexually assaulted by a family member (incest). She wants termination. Work through the legal framework: (1) Is she eligible under the MTP Act 2021? (2) What is the gestational limit that applies? (3) How many doctors' opinions are required? (4) What documentation must you complete? (5) What confidentiality obligations apply?