Page 13 of 17
FM8.4-5,FM14.12 | Infanticide, Foetal Age & Signs of Live Birth — SDL Guide
Learning Objectives
- Define infanticide, foeticide, and stillbirth and distinguish between them
- List the signs of intrauterine death, signs of live birth, and the criteria for foetal viability
- Explain foetal age determination at post-mortem using length, weight, and ossification centres (DOAP)
- Describe the hydrostatic test (Breslau's test) and its limitations
- Explain sudden infant death syndrome (SIDS) and Munchausen syndrome by proxy in the context of infant deaths
INSTRUCTIONS
The discovery of a dead newborn raises one of the most challenging questions in forensic pathology: was this a stillbirth, a live birth followed by natural death, or a live birth followed by deliberate killing? The entire criminal inquiry — and whether anyone will face a charge of infanticide or murder — rests on the medical evidence. This module equips you to approach neonatal death investigation systematically and to understand the limits of each test.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A newborn baby is found wrapped in a cloth behind a village bus stop. She appears full-term, shows no signs of decomposition, and has an intact umbilical cord. The police request a post-mortem to determine: Was this baby alive at birth? How old was the foetus? Did she die from natural causes, or was she killed? Three medical questions, three distinct examination steps, each with its own reliability and limitations.
WHY THIS MATTERS
Infanticide investigations are medico-legally among the most consequential, because the difference between a stillbirth and a neonatal homicide means the difference between no prosecution and a murder charge. Courts in India have accepted erroneous medical conclusions in infanticide cases with devastating consequences for mothers prosecuted for the natural death of a premature infant. The forensic clinician's precision — and their honesty about uncertainty — protects both the accused and the justice system.
RECALL
From obstetrics Year-1: recall foetal development milestones — crown-heel length approximately 10 cm at 12 weeks, 25 cm at 20 weeks, 35 cm at 28 weeks, 50 cm at 40 weeks (term). From anatomy: ossification of foetal bones follows a predictable sequence — long bone epiphyses, calcaneus, talus, and distal femoral epiphysis are forensically important. From FM so10-abortion SDL: foetal viability in India is 28 weeks / approximately 1 kg body weight.
Definitions: Infanticide, Foeticide, and Stillbirth
Precise definitions are the starting point because they determine both the forensic investigation pathway and the applicable criminal charge.
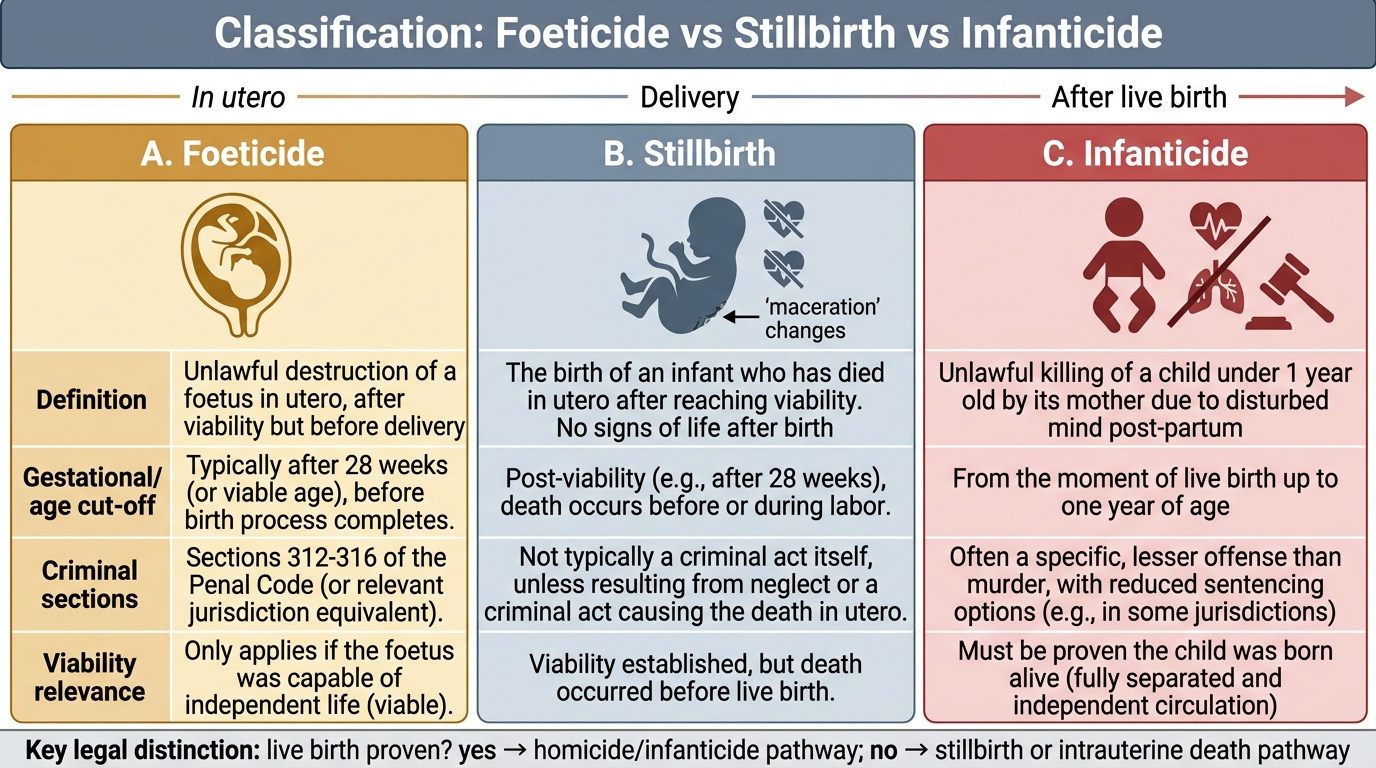
Foeticide is the killing of a foetus in the uterus. It may be induced by external trauma to the abdomen (e.g., assault on a pregnant woman) or by deliberate intervention. Foeticide that occurs before 28 weeks of gestation (before viability) is not separately criminalised as infanticide; it may constitute grievous hurt or culpable homicide depending on circumstances. Foeticide after 28 weeks (of a viable foetus) may constitute murder if done with intention to kill the foetus.
Stillbirth is the birth of a dead foetus — one that showed no signs of life after delivery. This may result from intrauterine death before labour (antepartum stillbirth) or death during labour (intrapartum stillbirth). A stillbirth is not a criminal event unless the death resulted from an external act (assault, criminal abortion). Registration of stillbirths is mandatory under the Registration of Births and Deaths Act when the foetus is ≥28 weeks.
Infanticide is the killing of a live-born infant. In Indian law, infanticide is charged under BNS provisions for murder or culpable homicide. The Infanticide Act in England specifically reduced the charge to manslaughter where a mother killed her infant while her mind was disturbed due to childbirth or lactation — no equivalent statutory concession exists in India, though the circumstances of delivery (exhaustion, mental state, precipitate labour) are considered in sentencing. The first legal requirement in any suspected infanticide investigation is to establish that the infant was born alive.
Live birth vs stillbirth — the central forensic question: A foetus is considered born alive if it shows any sign of life after complete expulsion from the mother — breathing, heartbeat, voluntary muscle movement, or pulsation of the cord, regardless of whether the cord has been cut. This follows the World Health Organisation's definition and is used in Indian forensic practice. Note: a foetus may breathe a few times in utero during a difficult labour (intrauterine respiration) — a specific trap in the Breslau/hydrostatic test.
Foeticide, Stillbirth, and Infanticide: Forensic Classification
Signs of Intrauterine Death and Signs of Live Birth
Signs of intrauterine death (maceration — the most important marker):
When a foetus dies in utero, autolytic changes begin within 6-12 hours. These changes are called maceration (distinct from post-mortem putrefaction which requires exposure to air/bacteria):
- 1st degree (6-12 hours): Skin slippage (epidermis separates from dermis in fluid-filled blebs), loss of firmness
- 2nd degree (2-3 days): Discolouration of skin (green, brown), slipping of scalp hair, mummification/collapse beginning
- 3rd degree (7+ days): Overlapping skull bones (Spalding's sign — important radiological finding of intrauterine death on plain X-ray), gas formation in major vessels, significant collapse
Maceration is a finding exclusively of intrauterine death — it cannot occur after a live birth. A macerated foetus is definitively a stillbirth. No maceration means no conclusion about live birth vs stillbirth from this sign alone — the infant may have been alive.
Signs of live birth (positive evidence):
These findings indicate that the infant breathed and/or had a functioning circulation after delivery:
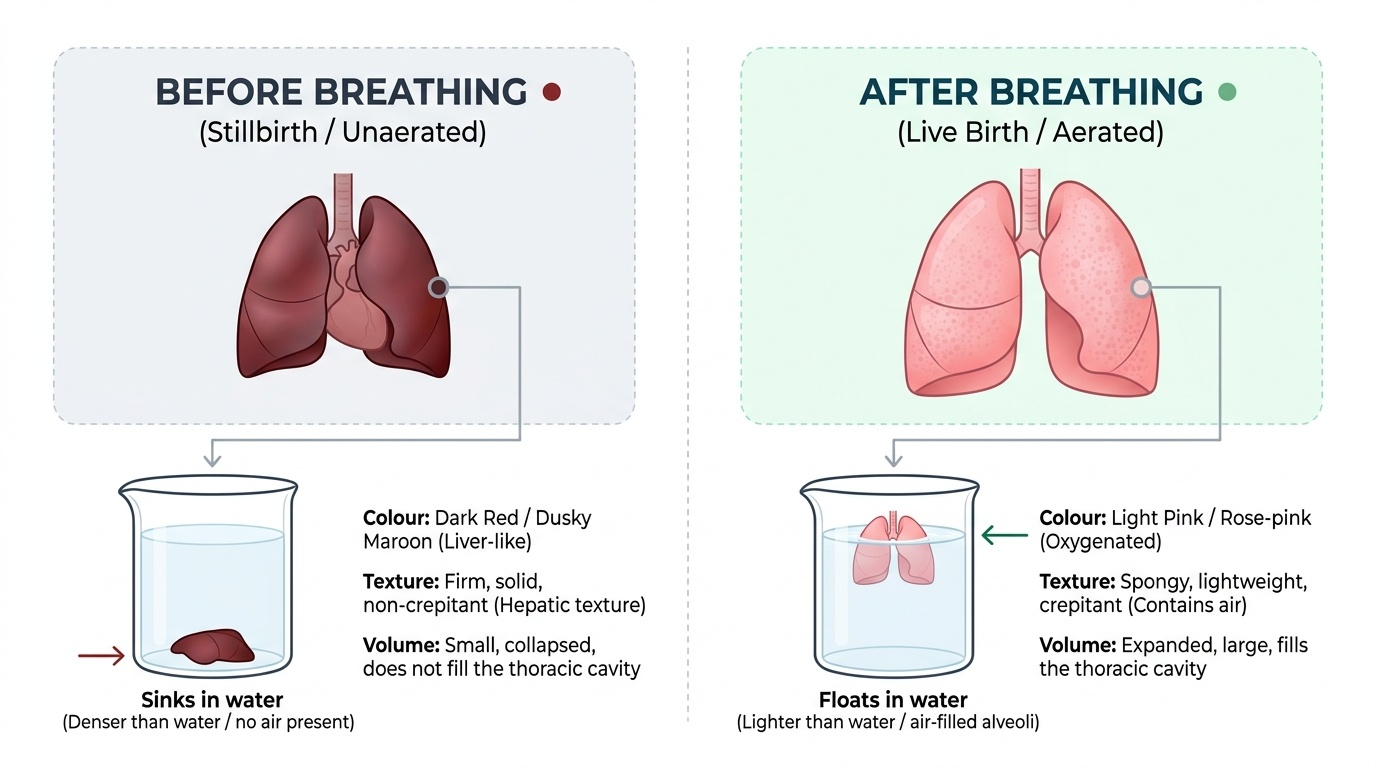
1. Hydrostatic test (Breslau's test / docimasia pneumatica): The most important traditional test. After death, the entire lung is placed in water. If the infant breathed, air entered the alveoli, making the lungs lighter than water — they float. If the infant never breathed (stillbirth), the lungs are airless and denser than water — they sink.
- Limitations (critical to state): (a) Artificial inflation — if attempts at resuscitation were made, or if the body was decomposing and gas formed from decomposition, the lungs may float falsely. (b) Putrefaction — post-mortem gas makes lungs buoyant regardless of respiratory function. (c) Intrauterine respiration — a foetus may make respiratory movements during prolonged labour, partially aerating the lungs, causing partial floating even in a stillbirth. Therefore: floating lungs = probable live birth (not conclusive); sinking lungs = probable stillbirth (not absolute). The test must be interpreted with the full post-mortem context.
- Gastric and intestinal air: If the infant breathed and swallowed air, gas will be present in the stomach and intestines. Confirmed by opening stomach and bowel under water — bubbles indicate aeration. This is the gastrointestinal docimasia or intestinal hydrostatic test. It is positive only when the infant survived for some hours post-delivery (time needed for swallowed air to pass into bowels).
3. Other signs of live birth:
- Expanded lungs that fill the pleural cavity completely
- Lung colour: pinkish-red and marbled (aerated) vs dark purple/violet (unexpanded foetal lungs)
- Blood in the hepatic sinuses (indicates circulation after delivery)
- Umbilical blood vessels show signs of functional closure (beginning of physiological change)
- Presence of food in stomach (if survived and fed)
- Meconium in bowel (foetal; some is passed shortly after birth)
Provided image
SELF-CHECK
At autopsy of a suspected infanticide, the lungs are placed in water and they float. However, the body shows significant post-mortem putrefaction with bloating. What is the most appropriate interpretation of the hydrostatic test result?
A. The infant was definitely born alive
B. The lungs floating is conclusive evidence of live birth regardless of other findings
C. The result is unreliable because putrefaction gas can produce buoyancy independent of respiration; the hydrostatic test in this case cannot confirm live birth
D. The result is valid only if reinforced by the intestinal hydrostatic test
Reveal Answer
Answer: C. The result is unreliable because putrefaction gas can produce buoyancy independent of respiration; the hydrostatic test in this case cannot confirm live birth
Putrefaction produces gas in tissues including the lungs, causing them to float regardless of whether the infant breathed. The hydrostatic test result is invalidated by significant putrefaction. The pathologist must note this limitation clearly in the report — a statement that 'lungs floated but the result is unreliable due to putrefaction' is the correct conclusion.
Foetal Viability and Foetal Age Determination at Post-Mortem
Foetal viability is the gestational age at which a foetus can survive extrauterine life, with or without support. In Indian legal context, viability is set at 28 weeks gestation or approximately 1 kg body weight. This threshold is used in the MTP Act context (see so10-abortion SDL) and in neonatal death investigations.
Foetal age determination at post-mortem (FM14.12): The pathologist must estimate gestational age from post-mortem measurements, particularly where the foetal age is disputed or unknown. The principal methods are:
1. Crown-heel length and body weight:
- 28 weeks: CHL approximately 35 cm, weight approximately 1 kg
- 32 weeks: CHL approximately 40 cm, weight approximately 1.5 kg
- 36 weeks: CHL approximately 45 cm, weight approximately 2.5 kg
- 40 weeks (term): CHL approximately 50 cm, weight approximately 3.2-3.5 kg
The Haase's rule approximates CHL: for the first 5 lunar months, CHL = square of the lunar month (e.g., 3 months = 9 cm); for months 5-10, CHL = lunar month × 5 (e.g., 7 months = 35 cm).
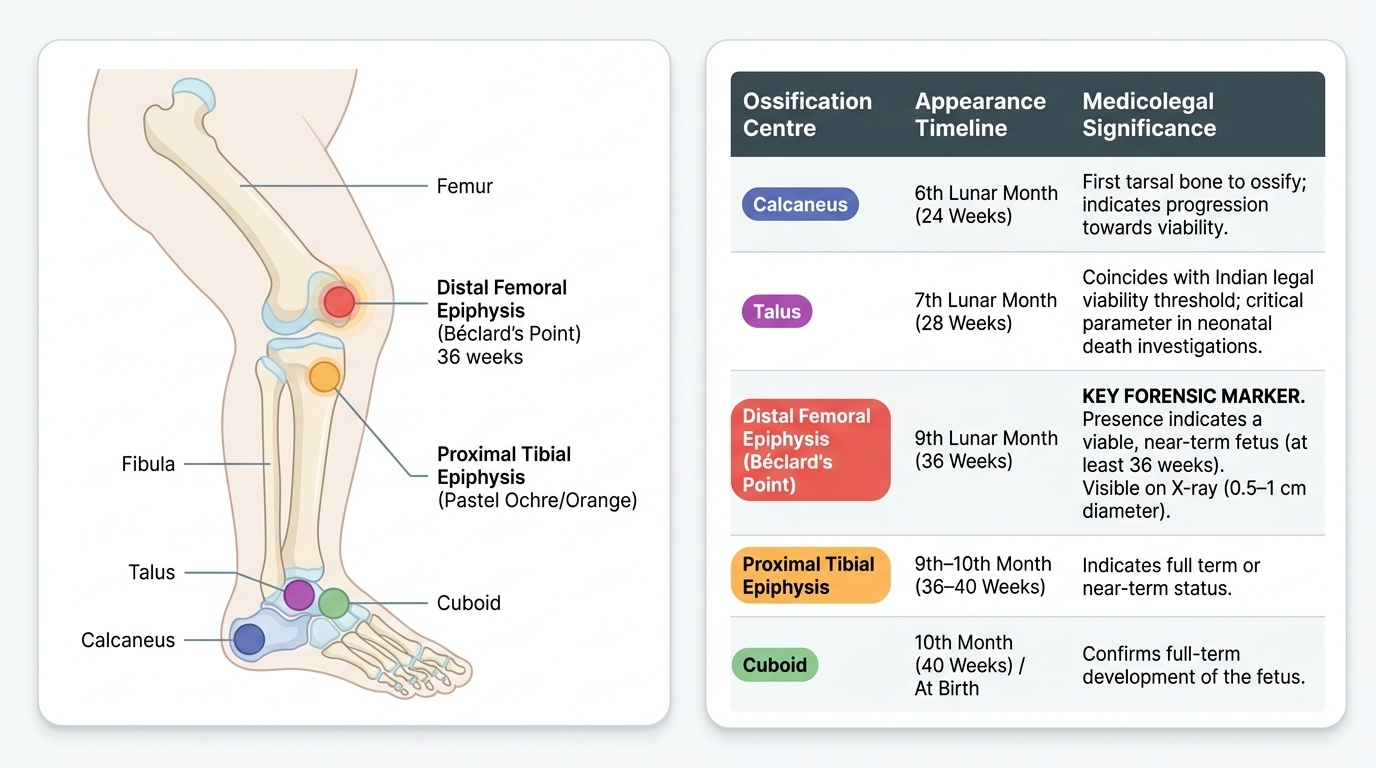
2. Ossification centre appearance (DOAP — Date of Appearance of Ossification centres): Ossification centres appear in a predictable sequence and can be demonstrated on X-ray or direct dissection:
| Ossification Centre | Appearance (Gestational Age) | Forensic Significance |
|---|---|---|
| Calcaneus | 6th month (24 weeks) | First tarsal bone to ossify |
| Talus | 7th month (28 weeks) | Coincides with viability threshold |
| Distal femoral epiphysis (Béclard's point) | 9th month (36 weeks) | KEY marker for near-term foetus |
| Proximal tibial epiphysis | 9th-10th month (36-40 weeks) | Indicates term or near-term |
| Cuboid | 10th month (40 weeks) / just after birth | Confirms term |
Béclard's point (distal femoral epiphysis) is the most forensically important ossification centre: its presence indicates the foetus was at least 36 weeks, making it viable and near term. The centre is 0.5-1 cm in diameter at term, visible on X-ray. Presence of Béclard's point = term or near-term foetus; absence = probable preterm.
Additional markers: myelination of spinal cord, state of skin (lanugo, vernix caseosa at term), testicular descent (testes usually descended by 36 weeks), nail development.
Provided image
SELF-CHECK
At post-mortem examination of a suspected neonatal death, X-ray of the knee shows a small ossification centre at the distal femoral epiphysis measuring 8 mm. What is the most appropriate inference?
A. The foetus was premature — Béclard's point is not fully formed
B. The presence of Béclard's point (distal femoral epiphysis) indicates the foetus was at least 36 weeks gestation and near term
C. The ossification centre at this location appears at 24 weeks — the foetus was non-viable
D. X-ray ossification centres cannot be used for age estimation in forensic cases
Reveal Answer
Answer: B. The presence of Béclard's point (distal femoral epiphysis) indicates the foetus was at least 36 weeks gestation and near term
Béclard's point (distal femoral epiphysis) appears at approximately 36 weeks gestation. Its presence confirms the foetus was at or near term (≥36 weeks), well within the viability threshold. This is a critical finding in infanticide investigations because it establishes that the infant was viable and near-term at delivery.
SIDS and Munchausen Syndrome by Proxy
Not all infant deaths are homicides or stillbirths. The forensic pathologist must also recognise natural causes of sudden infant death and a specific form of child abuse that mimics natural illness.
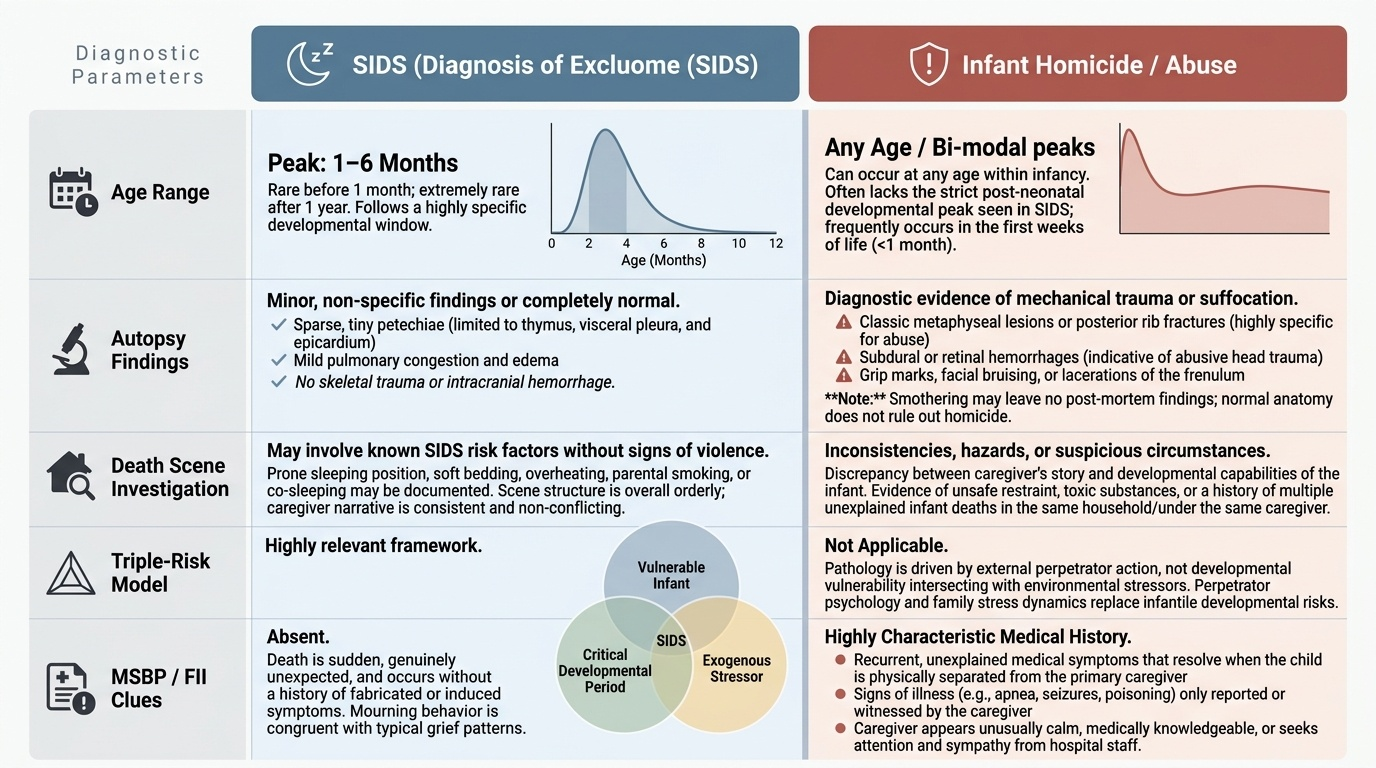
Sudden Infant Death Syndrome (SIDS) — also called cot death — is defined as the sudden, unexpected death of an apparently healthy infant under 1 year of age that remains unexplained after a thorough post-mortem examination, review of the clinical history, and investigation of the death scene. It is the leading cause of death in infants aged 1-6 months in high-income countries. The aetiology is multifactorial and incompletely understood — proposed mechanisms include immature arousal mechanisms, prone sleeping position, soft bedding, overheating, and parental smoking. The post-mortem examination in SIDS typically shows only minor non-specific findings (thymic petechiae, pulmonary congestion) — no single diagnostic finding establishes SIDS; it remains a diagnosis of exclusion.
Forensic significance: SIDS and infant homicide (overlaying/suffocation) can be extremely difficult to distinguish at autopsy. The absence of post-mortem findings does not exclude smothering. A thorough death-scene investigation (sleeping position, bedding, presence of co-sleepers, surveillance), careful review of prior medical consultations, and a systematic exclusion of other causes is required before concluding SIDS. Multiple SIDS deaths in the same family should raise a high index of suspicion for homicide.
Munchausen Syndrome by Proxy (Fabricated or Induced Illness — FII): This is a form of child abuse in which a caregiver (most commonly the mother) fabricates or induces illness in a child to obtain medical attention and sympathy. The child may be presented with recurring unexplained symptoms that resolve when separated from the caregiver. Methods include: smothering (to produce apnoea/cyanosis), inducing vomiting, administering toxins or drugs, tampering with medical samples. The clinical presentation is that of a child with recurrent mysterious illnesses that no doctor can explain. Medicolegal clues: symptoms occur only or primarily when the caregiver is present; symptoms resolve on hospital admission (when caregiver is restricted); multiple unexplained admissions; co-occurrent SIDS or sudden illness in siblings. The diagnosis has severe legal implications — it is a form of child cruelty under POCSO and BNS provisions.
Provided image
CLINICAL PEARL
The key Breslau's test limitation to state in any medico-legal report: 'The hydrostatic test is positive (lungs float), indicating probable respiratory function after delivery. However, this finding must be interpreted with caution as false positives can occur due to: (a) post-mortem gas in decomposed specimens, (b) artificial inflation from resuscitation attempts, and (c) partial intrauterine respiration during prolonged labour.' Always state these limitations — the court needs to know that a floating result is not absolute proof of live birth.
SELF-CHECK
A 6-month-old infant is found dead in his crib. Post-mortem examination shows only mild thymic petechiae and pulmonary congestion with no other significant findings. The parents sleep in the same room. Which is the most appropriate conclusion?
A. The infant died of SIDS — the post-mortem findings confirm it
B. The diagnosis is infanticide — multiple unexplained SIDS deaths confirm homicide
C. Post-mortem findings are non-specific; a thorough death scene investigation and history review are required before concluding SIDS; the possibility of overlaying or suffocation cannot be excluded on autopsy findings alone
D. The minor thymic petechiae confirm a natural cause of death
Reveal Answer
Answer: C. Post-mortem findings are non-specific; a thorough death scene investigation and history review are required before concluding SIDS; the possibility of overlaying or suffocation cannot be excluded on autopsy findings alone
SIDS is a diagnosis of exclusion. Non-specific post-mortem findings (thymic petechiae, pulmonary congestion) are consistent with SIDS but do not confirm it and do not exclude smothering. A thorough death-scene investigation, family history review, and systematic exclusion of other causes must be completed. Thymic petechiae are non-specific and can be seen in both SIDS and asphyxial deaths.
KEY TAKEAWAYS
Foeticide = killing of a foetus in utero. Stillbirth = birth of a dead foetus (maceration indicates intrauterine death). Infanticide = killing of a live-born infant. Live birth requires at least one sign of post-delivery vital activity. Hydrostatic test (Breslau's) — floating lungs = probable live birth, NOT conclusive; limitations: putrefaction, artificial inflation, intrauterine respiration. Foetal viability: 28 weeks / 1 kg in India. Age estimation: crown-heel length (Haase's rule), body weight, ossification centres — Béclard's point (distal femoral epiphysis) at 36 weeks is the key near-term marker. SIDS: diagnosis of exclusion; non-specific post-mortem findings; death-scene investigation required; multiple deaths in same family raises homicide suspicion. Munchausen syndrome by proxy: caregiver-induced illness; smothering is a recognised method; symptoms resolve away from caregiver.
REFLECT
A macerated foetus of approximately 32 weeks gestation is found in a plastic bag near a hospital. The hydrostatic test is not performed because of significant decomposition. Describe your approach to determining: (1) whether this foetus was born alive or was a stillbirth; (2) the approximate gestational age using available methods; (3) what other evidence you would look for and what the limitations of your conclusions are. How would you present this in your post-mortem report?