Page 6 of 17
FM8.8-9 | Pregnancy, Delivery & Disputed Parentage — SDL Guide
Learning Objectives
- List the signs of pregnancy (presumptive, probable, and positive) relevant to medico-legal contexts
- Define and explain superfoetation, superfecundation, and their medicolegal significance
- Describe the signs of precipitate labour and their forensic importance
- Differentiate signs of recent delivery from signs of remote delivery in living and dead women
- Explain the medico-legal aspects of disputed paternity and maternity, including the role of DNA testing
INSTRUCTIONS
Pregnancy and delivery generate a wide range of medico-legal questions — from inheritance and legitimacy disputes to criminal investigations of concealed births and infanticide. The examining doctor must be able to determine whether a woman is or has recently been pregnant, estimate gestational age, and assess whether delivery has occurred. This module covers the clinical and forensic foundations of these determinations.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young woman is found unconscious in a remote area. There is blood-stained material nearby and signs of recent labour. Is she the mother of a recently delivered child? Has she recently delivered a live or dead infant? How can the examining doctor tell whether delivery has occurred at all — and if so, approximately when? Separately, a court dispute over the inheritance of a substantial estate hinges on whether a child born to a widow 9 months after her husband's death is his legitimate heir. These are the questions this module addresses.
WHY THIS MATTERS
Pregnancy and delivery questions arise across a broad spectrum of medico-legal practice: criminal investigations (concealed pregnancy, infanticide, criminal abortion), civil proceedings (inheritance, legitimacy, disputed paternity), and public health (maternal mortality audits, coroner's inquests). The examiner who cannot reliably identify signs of recent delivery, or who cannot explain the clinical basis for disputed parentage testing, is unable to serve these judicial purposes effectively.
RECALL
From Year-1 obstetrics basics: pregnancy lasts approximately 280 days (40 weeks or 10 lunar months) from the last menstrual period. The embryo becomes a foetus at 8 weeks. Quickening (foetal movements felt by the mother) typically occurs at 18-20 weeks in primigravidae and 16-18 weeks in multigravidae. From anatomy: the uterus rises out of the pelvis at approximately 12 weeks and reaches the umbilicus at 20 weeks. From FM8.7 SDL: the Indian Evidence Act Section 112 presumes legitimacy for children born within 280 days of marriage dissolution.
Signs of Pregnancy: Presumptive, Probable, and Positive
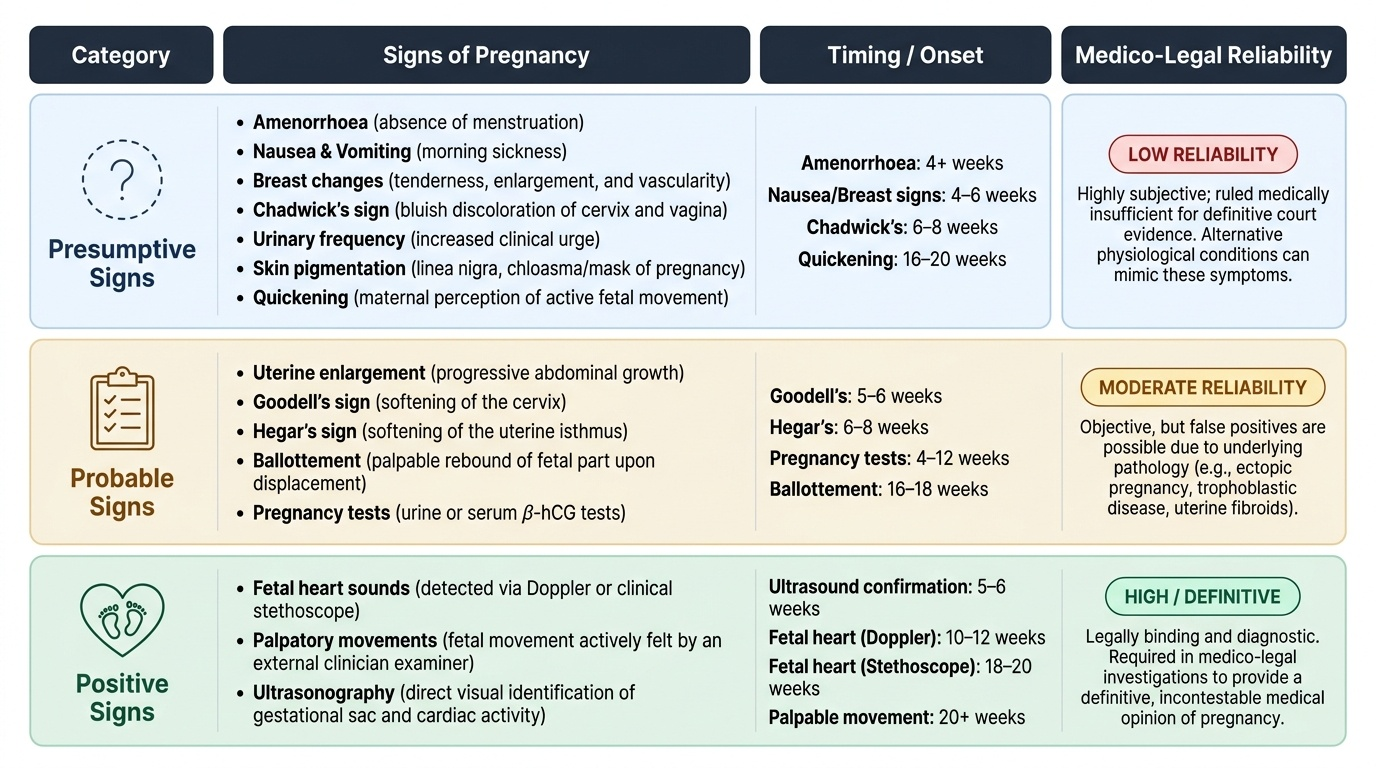
Signs of pregnancy are conventionally classified into three groups reflecting the reliability of each sign as evidence of pregnancy. This three-tier classification is important in medico-legal practice because courts require the doctor to assess confidence level.
Presumptive signs are subjective symptoms and early physical changes that suggest but do not prove pregnancy: amenorrhoea, nausea and vomiting (morning sickness), breast tenderness and enlargement, Chadwick's sign (bluish discolouration of the vagina and cervix from vascular congestion, appearing from 6-8 weeks), urinary frequency, skin pigmentation changes (linea nigra, chloasma), and quickening.
Probable signs are objective findings that strongly suggest pregnancy but have other explanations: uterine enlargement (may occur from fibroids), Goodell's sign (cervical softening), Hegar's sign (isthmic softening between corpus and cervix, 6-8 weeks), ballottement (foetal part rebounds on displacement), and pregnancy tests (urine or serum beta-hCG). A positive urine pregnancy test is a probable sign because false positives occur (ectopic pregnancy, trophoblastic disease, exogenous hCG).
Positive signs are diagnostic of intrauterine pregnancy: foetal heart sounds heard on auscultation (Doppler from 10-12 weeks, stethoscope from 18-20 weeks), foetal movements palpated by the examiner (not just felt by the mother), and ultrasonographic visualisation of the intrauterine foetus with cardiac activity.
In the medico-legal context, the positive signs are required for a definitive medical opinion that a woman is pregnant. For determining whether a woman was previously pregnant (in the context of investigations), the examiner looks for physical signs of pregnancy that persist after delivery — see below.
Provided image
Superfoetation and Superfecundation
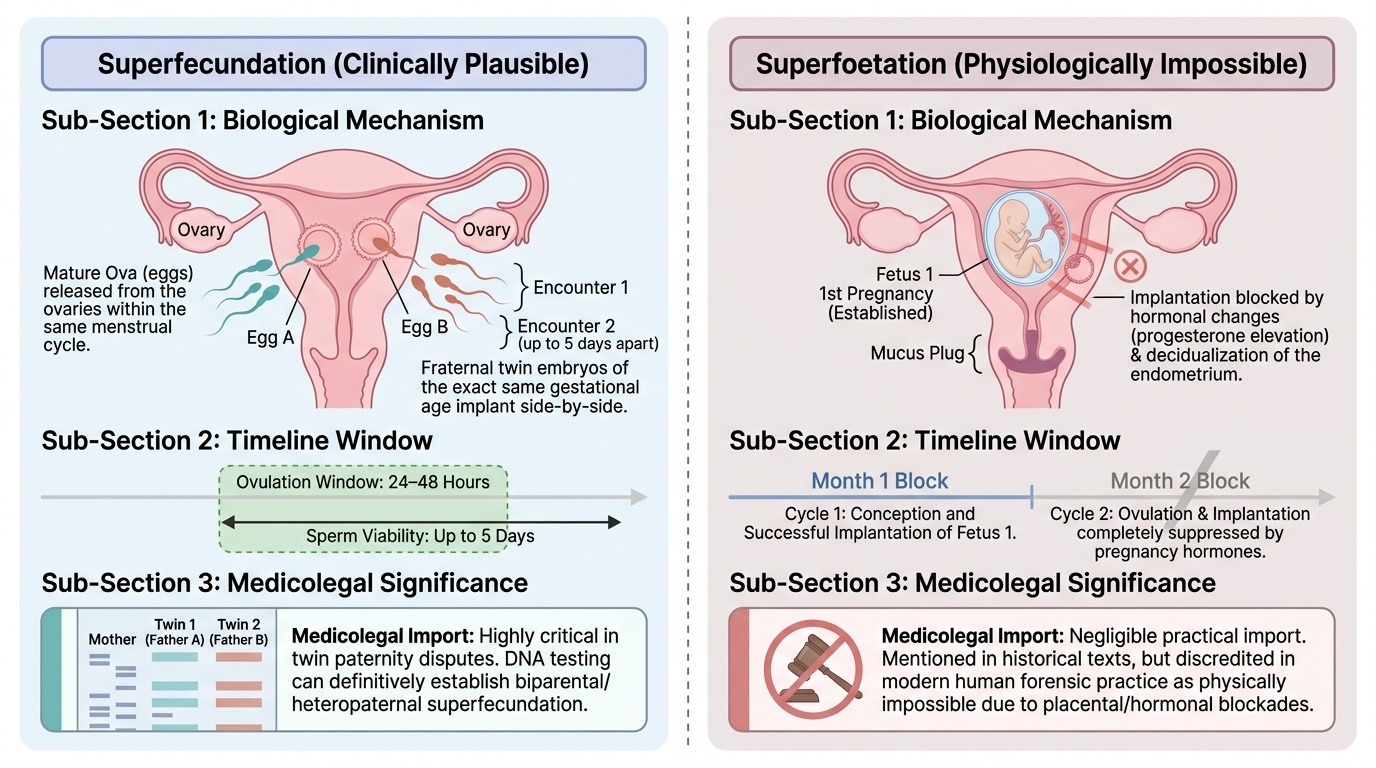
Two unusual but medico-legally important biological phenomena may arise in disputed parentage cases.
Superfecundation refers to the fertilisation of two or more ova during the same menstrual cycle by sperm from two different sexual encounters — which may be with the same or different men. In the latter case, a woman may give birth to fraternal twins with different biological fathers. This is theoretically possible because ova may be released over a 24-48 hour window and spermatozoa remain viable for up to 5 days in the female reproductive tract. Superfecundation is exceedingly rare but has been documented. Its medicolegal significance lies in paternity disputes involving twin pregnancies — DNA testing of both twins may reveal different paternity.
Superfoetation refers to the alleged occurrence of a second conception in a woman who is already pregnant — resulting in two foetuses of different gestational ages in the same uterus. This is considered virtually impossible in humans because once conception occurs, hormonal changes and decidualization of the endometrium prevent implantation of a second blastocyst. It is of theoretical interest and is mentioned in older forensic texts but has no established medicolegal case in modern practice. Its claimed medicolegal significance — that a woman might appear postterm on the basis of one foetus while another was delivered at term — is therefore of negligible practical import.
For practical examinations: know the definition of both; know that superfecundation (different fathers for twins) is the clinically plausible one; superfoetation in humans is considered physiologically impossible.
Provided image
Precipitate Labour: Definition and Forensic Significance
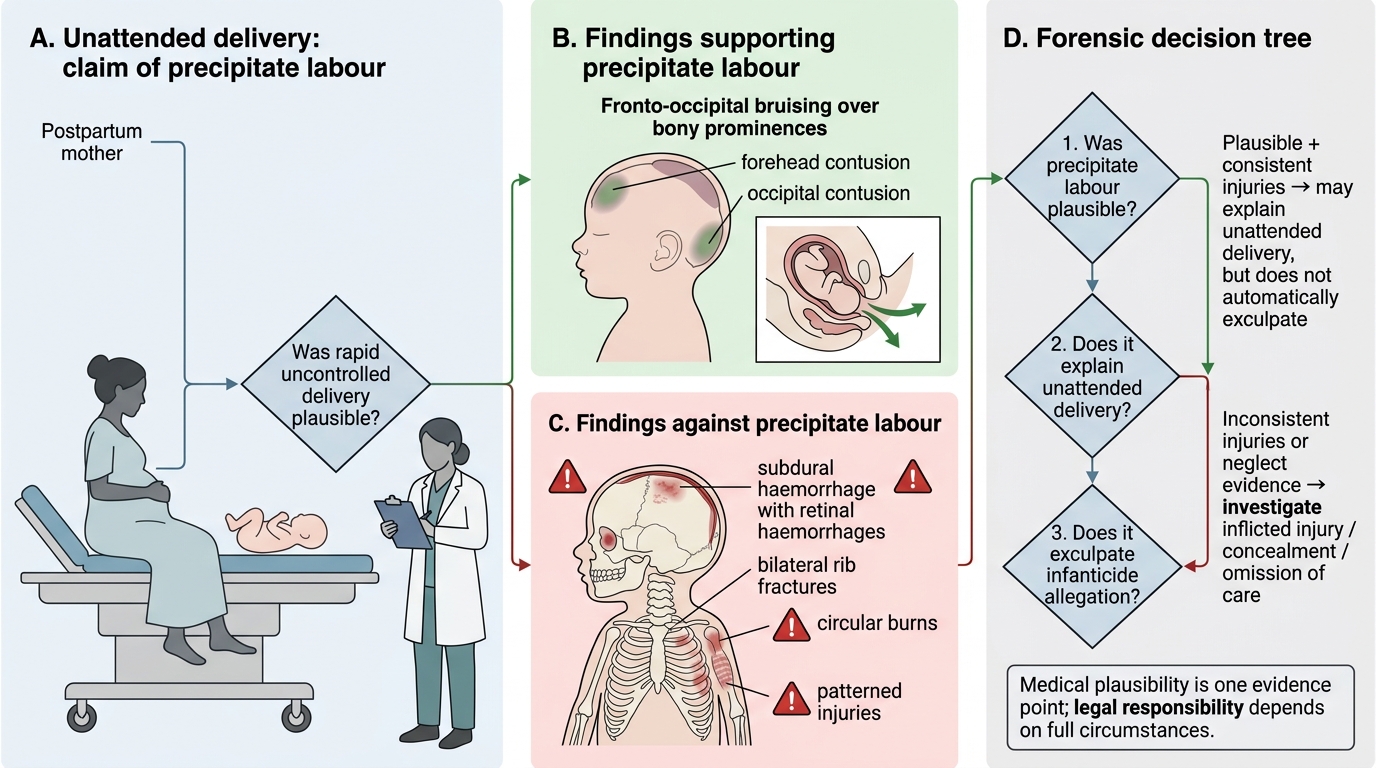
Precipitate labour is defined as labour in which delivery is completed within 3 hours of onset of uterine contractions. It is more common in multiparous women and may also occur in first pregnancies, particularly when the presenting part descends rapidly. The forensic significance of precipitate labour is substantial: a woman may deny knowledge of labour and delivery, claiming she was unaware she was about to deliver. This is one of the common explanations given in cases of alleged infanticide or concealed birth.
The relevance of precipitate labour to forensic practice: (1) it may explain why a delivery occurred in an unusual location without medical attendance; (2) it does not, by itself, explain why a live-born baby was not immediately cared for — failure to provide medical care to a live-born child is an offence under Indian law regardless of whether labour was precipitate; (3) injuries in the baby consistent with a precipitate or unattended delivery (e.g., fronto-occipital contusion from a rapid uncontrolled exit) must be distinguished from deliberate inflicted injury.
The doctor's role in a case with alleged precipitate labour is to document: (1) signs confirming recent delivery in the woman; (2) any injuries that may have resulted from rapid delivery versus those inconsistent with it; (3) neonatal injuries in the context of both spontaneous precipitate delivery and deliberate harm.
Forensic Assessment of Precipitate Labour Claim
SELF-CHECK
A multiparous woman is found with a freshly delivered baby that shows fronto-occipital bruising. She claims she delivered rapidly without warning. Which finding would be most consistent with precipitate labour as the cause of the infant's head injury?
A. Subdural haemorrhage with retinal haemorrhages
B. Fronto-occipital contusions over bony prominences, consistent with rapid uncontrolled expulsion through the birth canal
C. Multiple circular burns
D. Bilateral rib fractures
Reveal Answer
Answer: B. Fronto-occipital contusions over bony prominences, consistent with rapid uncontrolled expulsion through the birth canal
In precipitate labour, the infant's head may be expelled rapidly without controlled delivery, causing contusions over bony prominences (occiput, forehead) from contact with the pelvic floor or delivery surface. Subdural haemorrhage with retinal haemorrhages, rib fractures, and burns are inconsistent with precipitate labour and suggest inflicted injury.