Page 7 of 17
FM8.8-9 | Pregnancy, Delivery & Disputed Parentage — SDL Guide (Part 2)
Signs of Recent and Remote Delivery in Living and Dead
Determining whether a woman has recently delivered is a critical forensic skill, particularly in cases of concealed delivery, infanticide, or suspected criminal abortion. Signs differ between recent (within days) and remote (weeks to months) delivery, and between living and dead subjects.
Signs of RECENT delivery (within 7-10 days) in a LIVING woman:
- Uterine involution: fundal height regresses at approximately 1 cm per day after delivery; by day 1 it is at the umbilicus, by day 10 it has returned to the pelvis. A uterus palpable above the symphysis pubis in a woman claiming not to have recently delivered is a strong indicator.
- Lochia: vaginal discharge beginning red-brown (lochia rubra, days 1-4), progressing to pale (lochia serosa, days 4-9), then white/yellow (lochia alba, weeks 2-6). The presence of lochia is a reliable sign of recent delivery.
- Perineal changes: perineal lacerations, episiotomy scarring, bruising, or oedema consistent with passage of a term foetus.
- Breast changes: engorgement, colostrum or milk expression (secretion begins from day 2-3 and becomes established milk by day 4-5).
- Cervical os: remains dilated (admits one or two fingers) for 3-4 days post-delivery, then progressively closes.
Signs of RECENT delivery in a DEAD woman (post-mortem):
- Uterus: bulky, the inner surface shows placental site (roughened, raised, pale, haemorrhagic). Placental site dimensions can estimate delivery timing — it takes 4-6 weeks to fully involute.
- Lochia in the vaginal vault.
- Colostrum in the breast ducts.
- Perineal/cervical tears or sutured episiotomy.
- Dilated cervical os in the first 24-48 hours.
Signs of REMOTE delivery (weeks to months prior):
- Striae gravidarum (stretch marks): appear during pregnancy as red/pink, fade to silvery-white — old striae indicate prior pregnancy.
- Uterus slightly larger than nulliparous uterus (permanent change after delivery).
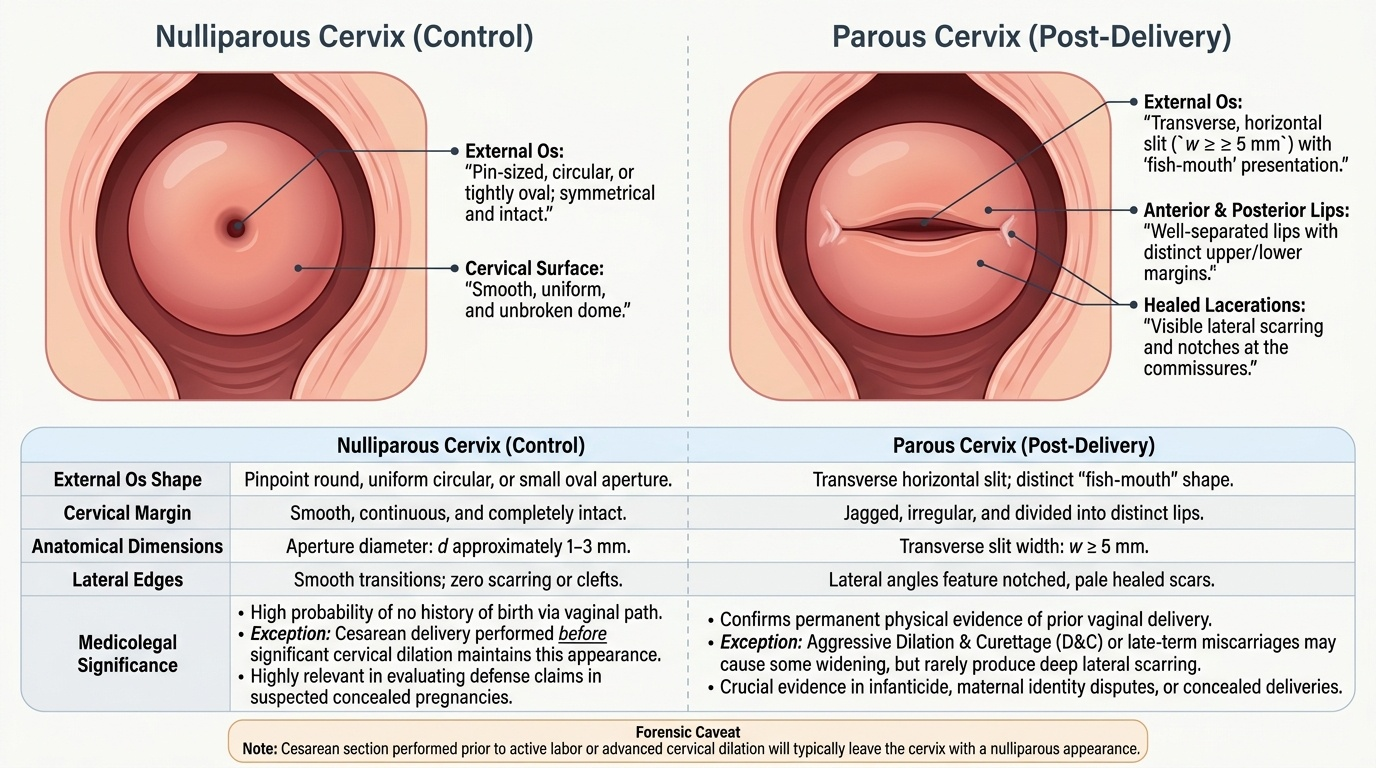
- Cervical os: parous os (wider, transverse slit) versus nulliparous os (small, round).
- Breast changes: persistence of Montgomery's tubercle enlargement, prior lactation evidenced by milk residue in ducts at post-mortem.
- Healed perineal scars.
Provided image
SELF-CHECK
On post-mortem examination of an unidentified woman, the uterus is bulky with a roughened, haemorrhagic placental site measuring 8 cm in diameter. Which inference is most appropriate?
A. The woman is currently pregnant
B. The woman delivered recently — the placental site indicates delivery within the preceding few days to weeks
C. The woman had a recent miscarriage that cannot be distinguished from term delivery
D. No inference about recent delivery can be drawn from post-mortem uterine examination
Reveal Answer
Answer: B. The woman delivered recently — the placental site indicates delivery within the preceding few days to weeks
A bulky uterus with a fresh placental site (roughened, haemorrhagic, raised area) is a reliable post-mortem sign of recent delivery or late pregnancy termination. The placental site begins to involute from the periphery and fully regresses over 4-6 weeks. A fresh, large placental site indicates delivery within days to weeks.
Disputed Paternity and Maternity: Medicolegal Framework
Disputed parentage cases arise in civil law (inheritance, legitimacy, maintenance) and occasionally in criminal investigations (kidnapping of children, surrogacy disputes). The medicolegal framework involves both clinical assessment and molecular genetics.
Disputed paternity: The most common scenario. The legal presumption of legitimacy (Indian Evidence Act Section 112 — recall from FM8.7 SDL) means that a court will only order DNA paternity testing if there is compelling reason to rebut the presumption. The doctor who is asked to advise on paternity must:
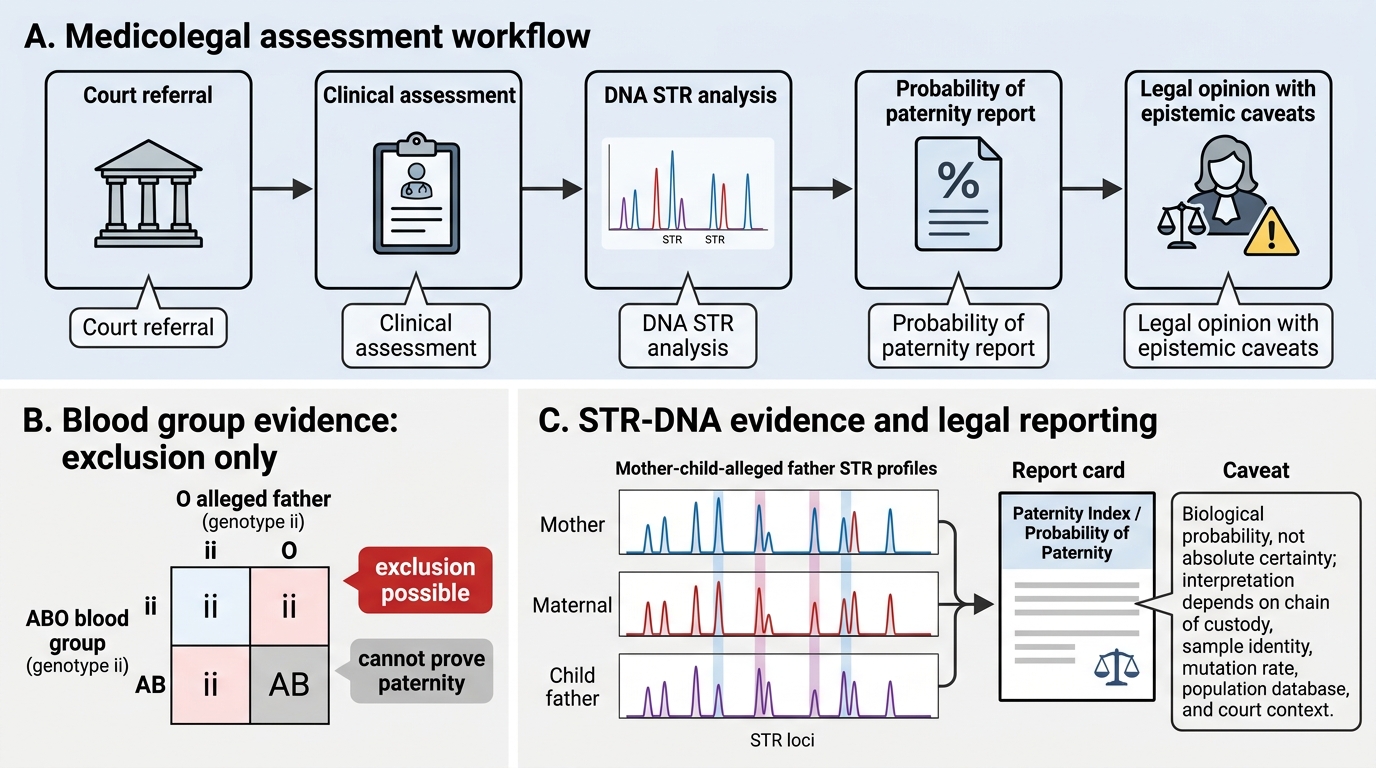
(1) Confirm that a positive paternity test uses short tandem repeat (STR) DNA analysis — the internationally accepted standard. A paternity index of ≥99.9% is required to include a man as the biological father to a reasonable scientific certainty. Exclusion (paternity probability = 0%) is definitive.
(2) Advise on the statistical interpretation of results — DNA evidence is probabilistic, not absolute; the court must still weigh it against the legal presumption.
(3) Note that blood group analysis alone cannot establish paternity — it can only exclude it in certain circumstances (e.g., a child of blood group AB whose alleged father is group O is excluded, but the test cannot affirmatively prove paternity).
Disputed maternity: Rare but arising in cases of alleged baby-switching at birth, surrogacy disputes, or trafficking investigations. Maternity is established by the same STR-DNA analysis. In surrogacy cases, both genetic (gamete donor) and gestational maternity may be at issue — the ART Regulation Act 2021 and Surrogacy Act 2021 (covered in so8-art) create the legal framework for resolving such disputes.
Post-mortem disputed paternity: Where the alleged father is deceased, DNA can be extracted from exhumed remains or archived biological specimens (blood samples, paraffin-embedded tissue blocks) — provided chain of custody is established. Courts in India have permitted such exhumation orders in inheritance disputes.
The doctor's role is advisory and technical: provide accurate biological information about DNA testing methods, limitations, and statistical interpretation. The legal determination of paternity or maternity remains with the court.
Medicolegal Assessment of Disputed Paternity
CLINICAL PEARL
Blood group testing can exclude paternity but cannot establish it. If a child is blood group AB, the father must have at least one A allele and the mother at least one B allele (or vice versa). A putative father who is group O (genotype ii) cannot be the biological father of a child with group AB. However, a man who is group A could be the father — or so could millions of other group A men. For affirmative paternity determination, STR-DNA analysis is mandatory.
SELF-CHECK
In a disputed paternity case, which of the following investigations provides the most definitive biological evidence for inclusion or exclusion of paternity?
A. ABO and Rh blood group typing of child, mother, and alleged father
B. Detailed physical resemblance assessment by a forensic anthropologist
C. Short tandem repeat (STR) DNA analysis comparing alleged father, mother, and child
D. HLA tissue typing
Reveal Answer
Answer: C. Short tandem repeat (STR) DNA analysis comparing alleged father, mother, and child
STR-DNA analysis is the international gold standard for paternity determination. Blood group typing can only exclude paternity in specific circumstances; it cannot establish it. Physical resemblance has no scientific validity for parentage determination. HLA typing was used historically but has been superseded by DNA.