Page 11 of 33
FM13.15 | Agrochemical & Pesticide Poisoning — SDL Guide
Learning Objectives
- Describe the mechanisms of toxicity, clinical features, and post-mortem findings for organophosphates, carbamates, organochlorines, pyrethroids, paraquat, and aluminium/zinc phosphide
- Apply the specific antidote protocols for organophosphate poisoning, including the critical time-window for pralidoxime (PAM)
- Recognise the clinical presentation of paraquat poisoning and explain why oxygen supplementation is contraindicated
- Describe the management of phosphine gas toxicity from aluminium/zinc phosphide ingestion
- Prepare a medicolegal report for pesticide poisoning, including specimen collection and statutory framework
INSTRUCTIONS
Pesticide poisoning is the leading cause of poisoning mortality in India and much of South Asia. Organophosphate and carbamate insecticides, together with rodenticides like aluminium phosphide and herbicides like paraquat, account for tens of thousands of deaths annually. The forensic medicine graduate must master both the clinical recognition of these agents and the medicolegal documentation that follows. This SDL is high-stakes — the antidote protocols and contraindications covered here are life-saving.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three cases arrive in the emergency department of a rural district hospital on the same morning during a harvest season dispute. The first: a 55-year-old farmer who was found unconscious in his field, sweating profusely, with tiny pupils and muscle twitching — his nephew says he was spraying insecticide. The second: a 28-year-old woman who admitted swallowing some 'green tablets' from the granary in a dispute — she now has mild GI symptoms but the nurses have put her on high-flow oxygen. The third: a 20-year-old student who swallowed what looks like a yellow tablet from a rat-poison packet and appears alert but complains of burning in the throat. The first case is straightforward organophosphate; the second case has received potentially lethal treatment; and the third poses a specific immediate airway and metabolic risk. How do you approach all three?
WHY THIS MATTERS
Pesticide poisoning is the number one cause of poisoning death in India, driven by easy agricultural accessibility, high self-harm rates (especially in farming communities under economic stress), and accidental occupational exposure. The diversity of agents — organophosphates, carbamates, organochlorines, pyrethroids, paraquat, and phosphide rodenticides — each with distinct mechanisms and management nuances, makes this the most complex single module in forensic toxicology. Errors in management (particularly giving oxygen to paraquat patients, or missing the pralidoxime time window in OP poisoning) are fatal. This is the clinical content most likely to be tested in your NEXT professional examination and most likely to matter in your first posting.
RECALL
Retrieve your pharmacology and physiology knowledge:
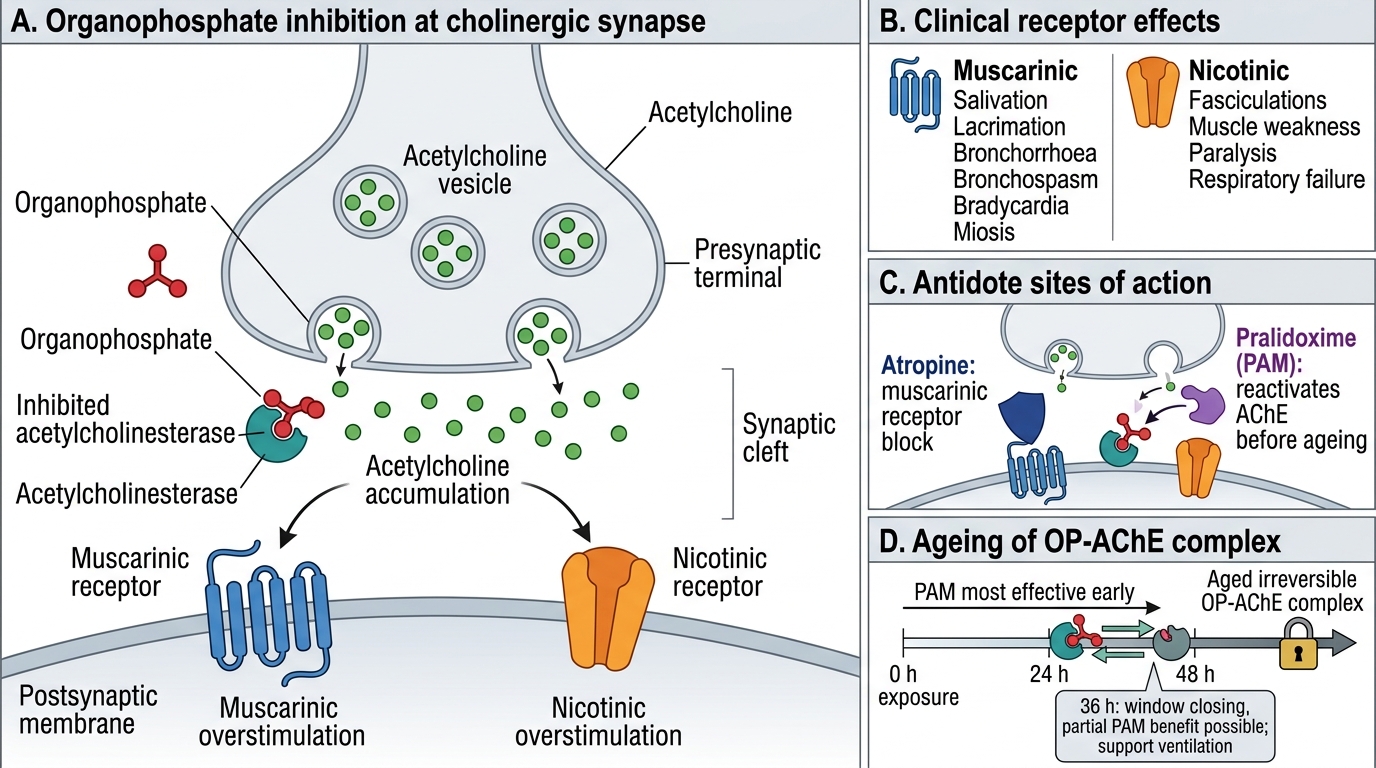
- Pharmacology (Year 2): the cholinergic synapse — acetylcholine (ACh) released from presynaptic terminal → binds muscarinic receptors (parasympathetic smooth muscle, glands, heart) and nicotinic receptors (skeletal muscle, autonomic ganglia) → acetylcholinesterase (AChE) in the synaptic cleft hydrolyses ACh, terminating the signal. Organophosphates block AChE → ACh accumulates → cholinergic excess.
- Physiology: the mnemonic SLUDGE for cholinergic excess — Salivation, Lacrimation, Urination, Defaecation, GI distress, Emesis. Add B for Bradycardia + Bronchospasm.
- Biochemistry: reactive oxygen species (ROS) and the Fenton reaction — free radical generation leading to lipid peroxidation. Paraquat generates superoxide radicals (O₂•⁻) in lung tissue via a redox cycling mechanism.
- Biochemistry: phosphine gas (PH₃) is produced by the reaction of aluminium or zinc phosphide with water/acid in the stomach — this is the mechanism behind tablet-form rodenticide toxicity.
Medicolegal Significance of Pesticide Poisoning in India
Pesticide poisoning represents the single most important cause of acute poisoning in India from a forensic medicine perspective, precisely because its high case volume intersects with complex medicolegal questions at every level of the health system. A forensic medicine doctor may encounter these patients as:
- A clinical emergency (the acutely poisoned farmer or suicide attempt) requiring immediate diagnosis and treatment
- A post-mortem case (suicidal, homicidal, or accidental death) requiring cause-of-death determination and specimen collection
- A compensation/occupational disease case (chronic organochlorine exposure in agricultural workers)
- A criminal case (intentional administration of pesticide in food or water — documented in Indian courts)
The forensic significance of each agent type:
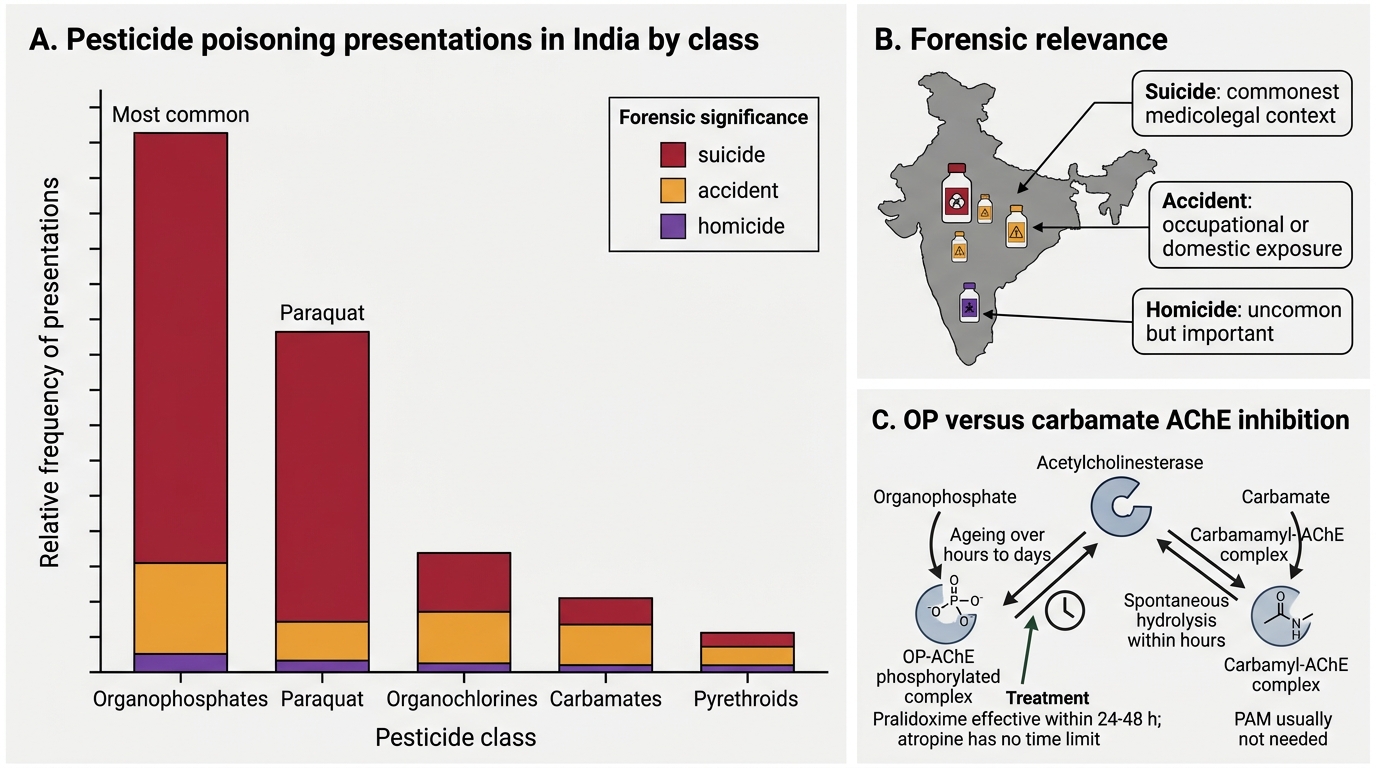
Organophosphates (OPs) and carbamates account for the majority of acute pesticide poisoning deaths in India. They are used as suicidal agents overwhelmingly more than in homicide. The availability of OPs in rural India is near-universal. Their forensic recognition is relatively straightforward due to the classic SLUDGE/cholinergic toxidrome.
Organochlorines (DDT, lindane, endosulfan) are largely restricted/banned in India, but legacy exposure and illegal trade mean they continue to appear in forensic practice — particularly in chronic poisoning in farmers and in cases of food contamination.
Paraquat is forensically distinctive because of its high lethality even in small doses and the absence of any effective treatment once systemic distribution has occurred. Cases of deliberate paraquat poisoning (occasionally in murder) and accidental herbicide exposure both require careful documentation.
Aluminium phosphide (AlP) and zinc phosphide (ZnP) — tablet-form rodenticides ('Celphos', 'Quickphos') — are among the most lethally toxic substances accessible in rural India. They are the second most common cause of pesticide suicide after OPs in some regions. The forensic doctor must know the mechanism (phosphine gas from gastric acid hydrolysis) and the absolute absence of any specific antidote.
Pesticide Poisoning in India: Frequency and Forensic Significance
Organophosphates and Carbamates: Mechanism, Features and Antidote Protocol
Mechanism of toxicity:
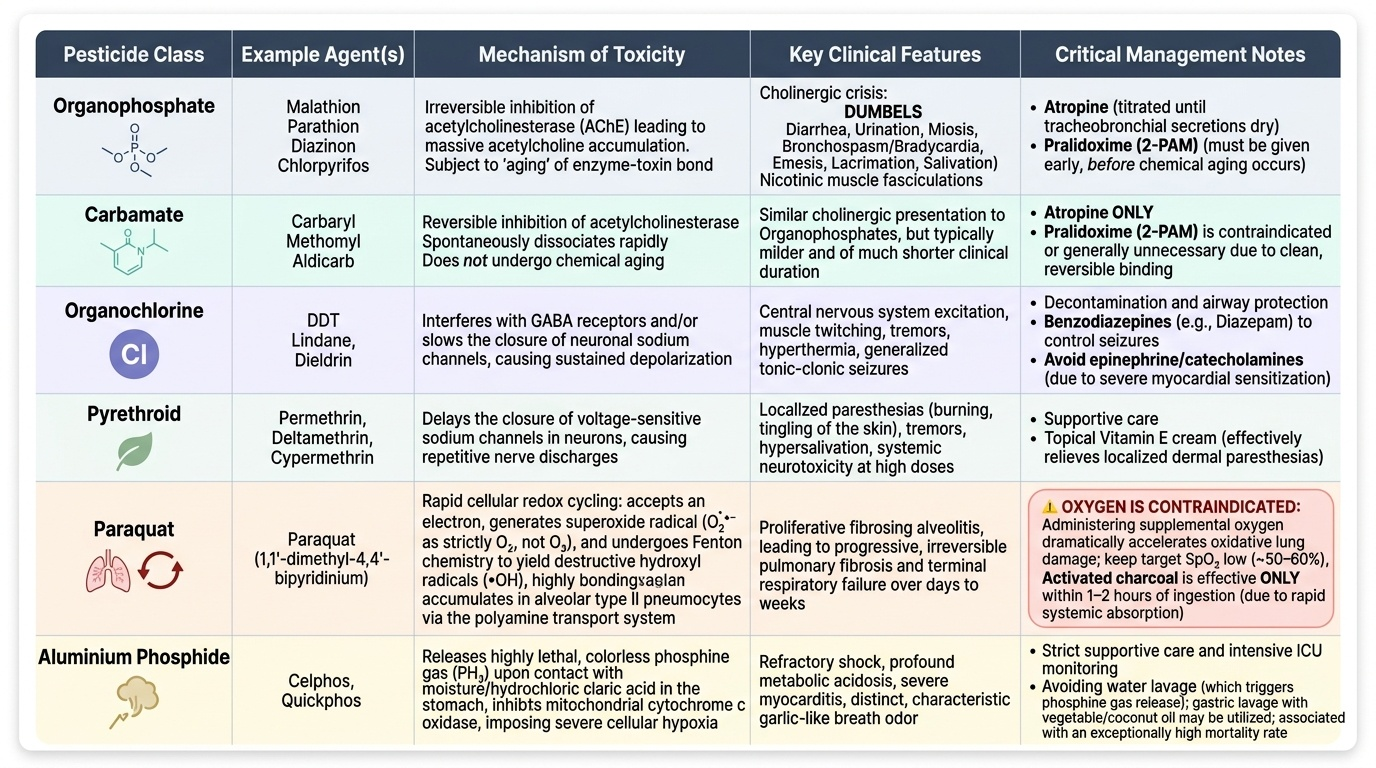
Organophosphates (OPs) — examples include malathion, parathion, chlorpyrifos, methyl bromide, sarin (nerve agents are also OPs). They inhibit acetylcholinesterase (AChE) by forming a covalent phosphoryl bond with the serine residue at the enzyme's active site. The OP-AChE complex initially can be reversed by an oxime (such as pralidoxime/PAM) — but over hours to days, the complex undergoes a process called ageing (dealkylation), after which it is irreversible and PAM becomes ineffective.
Critical time window for pralidoxime: PAM must be administered within 24–48 hours of exposure to be effective. After ageing of the OP-AChE complex, PAM administration is of no benefit. There is NO time limit for atropine.
Carbamates — examples include carbaryl, aldicarb, carbofuran — also inhibit AChE but form a carbamyl-AChE complex that spontaneously hydrolyses (reverses) within hours. Carbamate poisoning does not age, so PAM is not needed. The clinical picture is similar to OP but shorter-duration.
Clinical features of cholinergic toxidrome:
Muscarinic (SLUDGE + BB):
- Salivation (drooling), Lacrimation, Urination (incontinence), Defaecation/diarrhoea, GI cramps, Emesis
- Bradycardia, Bronchospasm + bronchorrhoea (excess secretions)
- Miosis (pupillary constriction — bilaterally, often pin-point)
Nicotinic (NMJ):
- Muscle fasciculations (spontaneous random muscle twitching — a key bedside sign)
- Weakness → flaccid paralysis (including intercostal/diaphragmatic → respiratory failure)
CNS:
- Anxiety, confusion, seizures, coma
The Intermediate Syndrome: A specific delayed OP complication — respiratory muscle weakness, proximal limb weakness, and cranial nerve palsies occurring 24–96 hours after cholinergic crisis has been treated. Not responsive to atropine or PAM — only supportive ventilation.
Antidote protocol (OP poisoning):
1. Atropine — muscarinic antagonist — competes with accumulated ACh at muscarinic receptors. Titrate to secretion-drying endpoint (dry secretions, HR >80 bpm, BP stable) — NOT to pupil size. Large doses may be needed (2–4 mg IV every 5–10 min, then repeat as needed — no upper dose limit if patient is genuinely atropinised). Atropine has NO effect on nicotinic (NMJ) features — will not stop fasciculations.
2. Pralidoxime (PAM/2-PAM) — oxime that reactivates AChE by displacing the OP from the active site. Must be given within 24–48 hours before ageing. 1–2 g IV over 15–30 min, then infusion. Treats BOTH muscarinic AND nicotinic features (unlike atropine).
3. Benzodiazepines: for seizures.
4. Supportive: airway (mechanical ventilation if paralysis), decontamination (remove clothing, skin wash), gastric lavage if early.
Organophosphate Poisoning at the Cholinergic Synapse
SELF-CHECK
A patient with organophosphate poisoning is brought in 36 hours after exposure. He has been treated with atropine and is now haemodynamically stable but still has marked muscle fasciculations and proximal weakness. Should pralidoxime (PAM) be given?
A. Yes — PAM should always be given regardless of time of exposure
B. No — at 36 hours the OP-AChE complex may have begun ageing; PAM may still have partial benefit but the window is closing; give atropine to maintain secretion control and support ventilation
C. No — PAM has no role in OP poisoning; it is used only for carbamate poisoning
D. Yes — PAM reverses the nicotinic effects and is always indicated regardless of timing
Reveal Answer
Answer: B. No — at 36 hours the OP-AChE complex may have begun ageing; PAM may still have partial benefit but the window is closing; give atropine to maintain secretion control and support ventilation
The critical window for PAM efficacy is 24–48 hours after OP exposure, before ageing (irreversible modification) of the OP-AChE complex. At 36 hours, some ageing may have occurred, making PAM less effective, but partial benefit is possible if given promptly. After 48 hours, PAM is ineffective. Atropine remains effective at any time (it acts on receptors, not on the enzyme). PAM is NOT used for carbamate poisoning (carbamates spontaneously reverse and PAM can paradoxically worsen the complex in some carbamates). The clinical decision at 36 hours: give PAM early (within the possible remaining window) while maximising atropine and respiratory support.
Paraquat, Phosphide Rodenticides, Organochlorines and Pyrethroids
PARAQUAT (1,1'-dimethyl-4,4'-bipyridinium):
Paraquat is a bipyridinium herbicide (weedkiller) with extraordinary lethality — ingestion of as little as 10–15 mL of the 20% concentrate can be fatal. Its mechanism is via redox cycling: paraquat accepts an electron (is reduced to a radical) then donates it to O₂, generating superoxide radical (O₂•⁻), which undergoes Fenton chemistry to produce hydroxyl radical (•OH). This cycle repeats indefinitely, generating massive oxidative stress.
The lung is the primary target — alveolar type II pneumocytes actively accumulate paraquat via the polyamine transport system (which normally transports spermine/spermidine). Consequence: proliferative fibrosing alveolitis — initial alveolar exudate followed by progressive fibrosis → irreversible respiratory failure (days to weeks).
CRITICAL: Oxygen is CONTRAINDICATED in paraquat poisoning. Supplemental oxygen dramatically accelerates paraquat-mediated oxidative lung injury (more O₂ → more superoxide generation → faster fibrosis). Keep SpO₂ at the minimum compatible with life (~50–60% in guidelines). This is the lethal treatment error illustrated in the hook scenario (the nurse putting the patient on oxygen).
Activated charcoal is effective ONLY within 1–2 hours of ingestion (paraquat is rapidly absorbed). After 2 hours, charcoal does not prevent systemic toxicity.
No specific antidote. Treatment is supportive: gastric lavage (early), charcoal (if early), antioxidants (N-acetylcysteine, vitamin C, vitamin E) as adjuncts, transplant (theoretical for lung), haemodialysis (removes paraquat before distribution — must be very early).
ALUMINIUM PHOSPHIDE (AlP) and ZINC PHOSPHIDE (ZnP):
These solid tablet/granule rodenticides react with moisture (gastric acid, atmospheric water) to release phosphine gas (PH₃) — a highly toxic cellular poison.
- AlP (brand names: Celphos, Quickphos, Phostoxin) — the most common cause of phosphide suicide in India
- Characteristic smell of phosphine: garlic-like (similar to yellow phosphorus) and rotten fish — a recognisable and important identifier
- Mechanism: phosphine inhibits cytochrome c oxidase (as does cyanide) → cellular hypoxia; also causes direct myocardial toxicity
- Clinical: nausea, vomiting, hypotension, cardiovascular collapse, multi-organ failure
- No specific antidote — this is absolute. Atropine, N-acetylcysteine, and magnesium have been studied but none proven effective. Treatment is entirely supportive.
ORGANOCHLORINES (DDT, BHC/lindane, endosulfan, chlordane):
Organochlorines act by prolonging sodium channel opening in neural membranes, causing sustained depolarisation → excitatory CNS toxicity. Clinical: tremor, hyperexcitability, convulsions. They are highly lipophilic and bioaccumulate. Most have been banned for agricultural use in India (DDT still used in malaria vector control). PM: no characteristic gross findings; analytical toxicology (GC-MS) required.
Treatment: benzodiazepines for seizures; gastric decontamination; NO specific antidote.
PYRETHROIDS (permethrin, cypermethrin, deltamethrin):
Synthetic pyrethroids also act on voltage-gated sodium channels (delay closing → prolonged depolarisation), producing a similar but generally milder excitatory syndrome than organochlorines. Also cause type I and type II toxicity (type I = tremor; type II = salivation, choreoathetosis, seizures). Much less toxic than organochlorines. Treatment: supportive; benzodiazepines for convulsions.
Provided image
SELF-CHECK
A 25-year-old presents having swallowed 15 mL of paraquat herbicide 3 hours ago. She is alert, SpO₂ 97% on room air. Which of the following management decisions is MOST important to prevent her death?
A. Start high-flow oxygen immediately to maintain SpO₂ >98%
B. Give activated charcoal — 3 hours is within the effective window
C. Maintain SpO₂ at minimum acceptable levels and avoid supplemental oxygen; give N-acetylcysteine and consider early haemodialysis
D. Give atropine 2 mg IV and repeat as needed
Reveal Answer
Answer: C. Maintain SpO₂ at minimum acceptable levels and avoid supplemental oxygen; give N-acetylcysteine and consider early haemodialysis
Paraquat poisoning — oxygen must be withheld or kept to an absolute minimum because supplemental O₂ dramatically accelerates paraquat's superoxide-generating redox cycle in lung tissue, accelerating fatal alveolitis. At 3 hours, activated charcoal is BEYOND its effective window (useful only within 1–2 hours of ingestion). Early haemodialysis may remove some paraquat before full distribution. N-acetylcysteine is an adjuvant antioxidant. Atropine is for organophosphate (cholinergic) poisoning — irrelevant here.