Page 12 of 33
FM13.15 | Agrochemical & Pesticide Poisoning — SDL Guide (Part 2)
Clinical Examination, Post-Mortem Findings and Medicolegal Documentation
Clinical examination approach in pesticide poisoning:
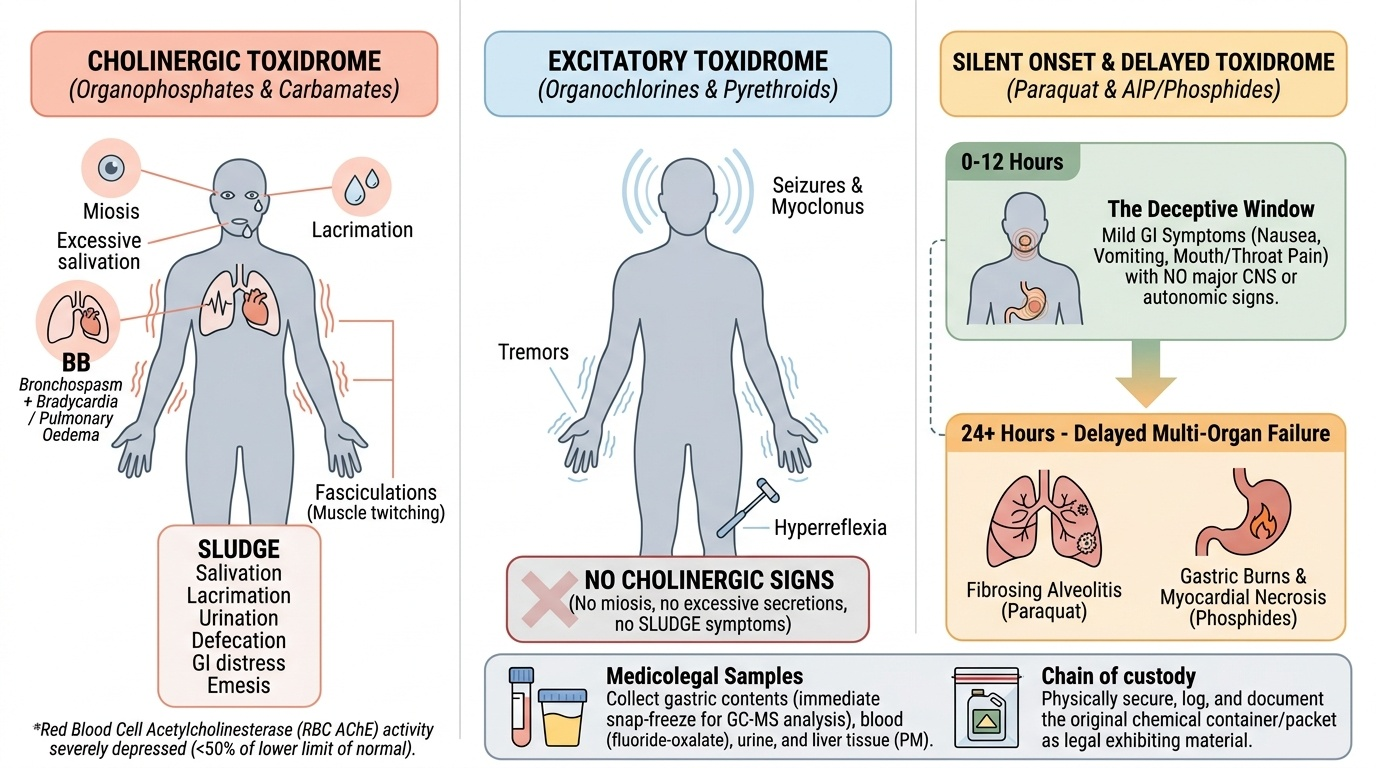
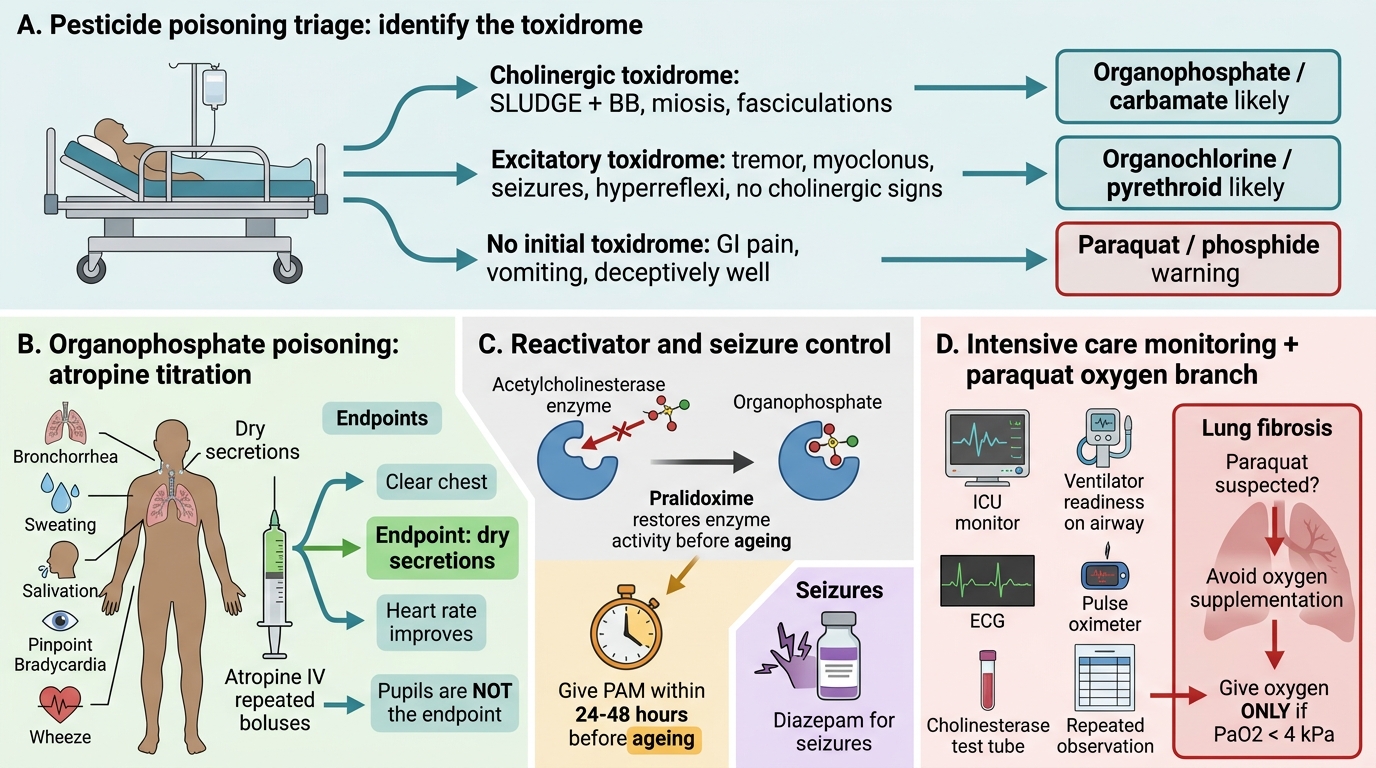
The clinical examination must serve two functions: emergency triage and medicolegal documentation. The first step is to identify the toxidrome — the constellation of signs that points to a pesticide class.
Cholinergic toxidrome (OP/carbamate): SLUDGE + BB + miosis + fasciculations. No other toxidrome produces this combination.
Excitatory toxidrome (organochlorine/pyrethroid): tremor, myoclonus, seizures; hyperreflexia; NO cholinergic signs.
No initial toxidrome (paraquat, phosphide): patient may appear deceptively well initially — this is the most dangerous pattern. GI symptoms (nausea, vomiting, mouth/throat pain) without major CNS or autonomic signs in the first hours.
History documentation:
- Time of exposure/ingestion
- Product name (ask family to bring the container — the label specifies the active ingredient class)
- Route (ingestion/inhalation/skin)
- Quantity ingested
- Any first aid given
- Circumstances (occupational, suicidal, accidental, homicidal)
Key investigations to document:
- RBC AChE activity (cholinesterase level) — confirms OP/carbamate exposure; depressed AChE (<50% of baseline) = significant exposure. Important: baseline varies between labs — compare with the lower limit of normal, not an individual baseline.
- ECG (QTc prolongation in OP/carbamate and phosphide; arrhythmia)
- ABG (metabolic acidosis in phosphide, paraquat)
- Chest X-ray (OP pulmonary oedema; paraquat alveolitis on serial films)
Post-mortem findings:
- OP/carbamate: cholinergic excess — pulmonary oedema (most consistent finding), bronchial hypersecretion, petechial haemorrhages; garlic odour (organophosphates); reduced AChE in PM blood
- Paraquat: fibrosing alveolitis — honeycombing, consolidation on X-ray; PM lung shows typical proliferative fibrosis histologically
- AlP: gastric burns, pericardial haemorrhage, myocardial necrosis; phosphine detected by Drager tube/chemical test in headspace gas
Medicolegal documentation:
Samples: gastric contents (most important — snap-freeze for organophosphate/pyrethroid GC-MS), blood (fluoride-oxalate), urine, liver (PM). The empty bottle/packet should be seized and documented as exhibiting material.
Provided image
Medicolegal Inference and Statutory Framework
The vast majority of pesticide poisoning deaths in India are suicides, but homicidal administration is documented — particularly organophosphate added to food or drink, and paraquat ingestion after domestic disputes (its presence in food is not easily detected by taste). The forensic medicine specialist's MLR must:
- State the cause of death (e.g., 'Acute organophosphate poisoning causing respiratory failure and multi-organ failure')
- Describe the route and manner (ingestion; suicidal/accidental/homicidal — based on circumstances)
- Confirm the diagnosis (analytical toxicology findings, AChE activity)
- Document the exhibit chain of custody
Treatment summary for examination recall:
| Agent | Antidote/key treatment | CONTRAINDICATION |
|---|---|---|
| Organophosphate | Atropine (no dose limit) + PAM within 24–48 h | PAM after ageing (>48 h — of no benefit) |
| Carbamate | Atropine only | PAM (not needed; may worsen in some carbamates) |
| Paraquat | Supportive only; avoid O₂ | OXYGEN — contraindicated |
| AlP/ZnP | Supportive only | No antidote exists |
| Organochlorine | Benzodiazepines for seizures | — |
| Pyrethroid | Benzodiazepines, supportive | — |
Statutory context:
- IPC §302/304 (murder/culpable homicide) if homicidal
- IPC §304A (negligence) if occupational health breach
- Insecticides Act 1968: regulates manufacture, sale, and use of pesticides in India; violation of storage/labelling norms by employers may constitute criminal negligence
- Environment Protection Act 1986: regulates organochlorine use; relevant if environmental contamination caused exposure
Emergency Management Flowchart for Organophosphate Poisoning
CLINICAL PEARL
Two absolute rules for pesticide poisoning management that override clinical intuition:
- Paraquat: NEVER give oxygen. Even SpO₂ of 85–90% should be tolerated unless the patient cannot maintain any oxygenation — supplemental oxygen accelerates fatal pulmonary fibrosis. This is counter to every other emergency medicine reflex of 'give oxygen first'.
- PAM in OP poisoning: the 24–48 hour window is absolute. After the OP-AChE complex ages (irreversible phosphorylation), pralidoxime is not only ineffective but potentially harmful in some experimental models. Atropine, however, has no time limit — it treats receptor-level muscarinic excess regardless of enzyme ageing.
SELF-CHECK
Which of the following statements about aluminium phosphide (AlP) poisoning is CORRECT?
A. IV atropine is the specific antidote for phosphine gas toxicity
B. AlP poisoning has NO specific antidote; management is entirely supportive
C. Phosphine is odourless, making clinical detection impossible
D. PAM (pralidoxime) reverses phosphine's inhibition of cytochrome oxidase
Reveal Answer
Answer: B. AlP poisoning has NO specific antidote; management is entirely supportive
Aluminium phosphide (AlP) and zinc phosphide (ZnP) release phosphine (PH₃), which inhibits cytochrome c oxidase causing cellular hypoxia and direct cardiac toxicity. There is NO specific antidote — management is entirely supportive (haemodynamic support, cardiac monitoring, mechanical ventilation). Atropine addresses cholinergic excess (it is used in OP poisoning, not phosphide). Phosphine has a distinctive garlic-like/rotten fish smell, NOT odourless. PAM is an AChE reactivator (for OP poisoning), not a cytochrome oxidase reverser.