Page 7 of 33
FM13.13 | Metallic Poisons (Arsenic, Lead, Mercury, Copper, Iron) — SDL Guide
Learning Objectives
- Describe the sources, routes of exposure, and mechanisms of toxicity for arsenic, lead, mercury, copper, and iron
- Identify the characteristic clinical features and post-mortem findings for each metallic poison
- Apply the treatment framework — decontamination, supportive care, chelation therapy, and enhanced elimination — appropriate to each metal
- Recognise the forensic significance of chronic metallic poisoning (Mees' lines, lead lines) and the analytical methods used to confirm metal poisoning
INSTRUCTIONS
Heavy metal poisoning occupies a distinctive position in forensic medicine because it spans the entire spectrum from acute homicidal poisoning (arsenic) to occupational disease (lead, mercury) to iatrogenic overdose (iron in children). Each metal has specific clinical signatures, diagnostic tests, and chelation strategies. This SDL builds competency to both clinically manage and forensically investigate metallic poisoning.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old man with no known illness presents with a six-month history of progressive fatigue, abdominal cramps, peripheral numbness, and darkening of his skin in a 'raindrop' pattern. His nails show transverse white lines. His wife says a neighbour has been giving him herbal tonics. Blood arsenic level comes back at 180 µg/L (normal <20 µg/L). The police want your opinion: is this occupational exposure, accidental, or deliberate long-term poisoning? In the same week, a 3-year-old is brought in obtunded after chewing an iron supplement tablet. And down the road, workers from a battery recycling plant are presenting with wrist drop and anaemia. Three different metals. Three different forensic contexts. One systematic framework.
WHY THIS MATTERS
Metallic poisons are among the oldest and most forensically significant toxins known to medicine. Arsenic was historically the 'inheritance powder' of Europe — used in family homicides because it was odourless, tasteless, and mimicked gastrointestinal disease. Lead, mercury, and copper remain critically important in India because of widespread occupational exposure, traditional/herbal medicine contamination (heavy metals in Ayurvedic formulations), and environmental exposure in mining and industrial communities. Iron is the most common childhood poisoning from unintentional tablet ingestion. Forensic medicine graduates must recognise the clinical and post-mortem signatures of each and understand the chelation strategies that drive both treatment and, in survivors, the collection of evidence.
RECALL
Retrieve relevant Year-1 knowledge:
- Biochemistry: sulfhydryl (–SH) groups on enzymes — many metalloenzymes contain cysteine residues with –SH groups that are essential for catalytic activity. Heavy metals (arsenic, lead, mercury) bind –SH groups, inactivating enzymes. This is the central mechanism of heavy metal toxicity.
- Physiology: haem synthesis pathway — the series of enzymatic steps from succinyl-CoA + glycine → porphobilinogen → haem. Lead inhibits two key enzymes in this pathway (ALA dehydratase and ferrochelatase), causing hypochromic microcytic anaemia and accumulation of precursors (basophilic stippling).
- Biochemistry: the concept of chelation — formation of a ring-structured complex between a chelating agent and a metal ion, sequestering the metal and allowing renal excretion.
- Pathology: tubular necrosis — the proximal renal tubule is highly metabolically active and is selectively damaged by heavy metals (arsenic, lead, mercury, iron); recognise the pattern of proximal tubular dysfunction (Fanconi syndrome in lead, mercury).
Medicolegal Significance of Metallic Poisons
Heavy metal poisoning presents the forensic medicine specialist with a unique challenge: the same metal can appear in criminal, occupational, environmental, and iatrogenic contexts, and distinguishing between them requires integration of clinical findings, exposure history, and analytical toxicology. The medicolegal significance varies by metal:
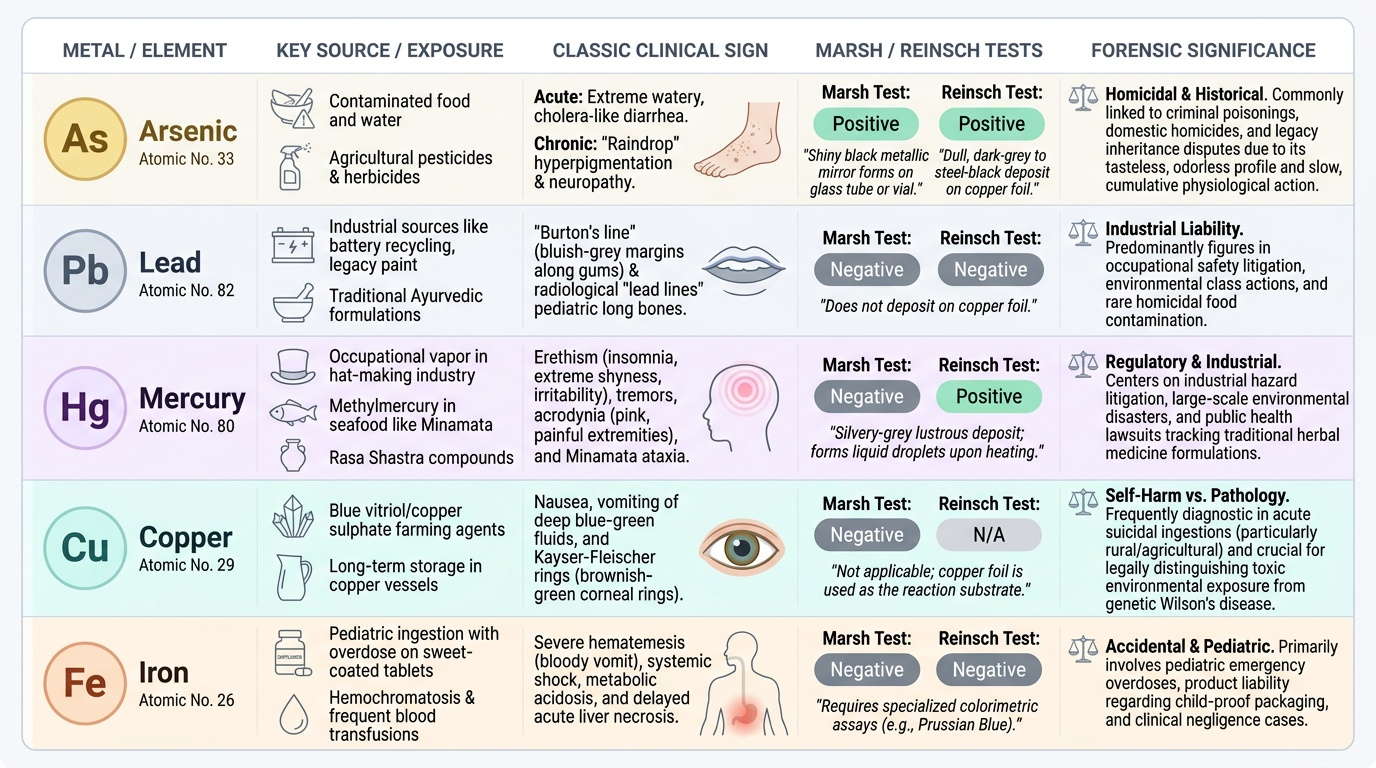
Arsenic — historically and currently the most important forensic metal because it can be administered chronically without detection (no colour, no distinctive smell in food), mimics infectious gastroenteritis in the acute form, and mimics nutritional deficiency or peripheral neuropathy in the chronic form. The famous Marsh test (1836) was the first modern analytical toxicology technique developed specifically to detect arsenic in forensic cases. Arsenic poisoning has been used in insurance fraud, inheritance disputes, and domestic homicide in India.
Lead — primarily occupational and environmental today (battery recycling, paint removal, leaded petrol legacy, Ayurvedic medicines) but may constitute a homicide by contamination of food with lead compounds. The Burton's line and radiological metaphyseal 'lead lines' in children provide forensic markers.
Mercury — both elemental and organic mercury (methylmercury — Minamata disease) are forensically significant. Mad Hatter's disease (occupational inorganic mercury in hat-making) is a historical example. Mercury in traditional/herbal preparations (rasa shastra compounds in Ayurveda) is a current concern.
Copper — copper sulphate (vitriol) is used in India as a pesticide and has been involved in homicidal and suicidal poisoning. Copper toxicity also occurs in Wilson's disease (genetic) and from copper vessel water storage — forensic distinction from endogenous copper disease is important.
Iron — predominantly a paediatric poisoning concern (iron tablet ingestion in children), but iron overload from transfusions and haemochromatosis may also produce medically and legally significant toxicity.
Provided image
Arsenic: Toxicokinetics, Features and Forensic Recognition
Arsenic is the most forensically important heavy metal in Indian practice. It exists in multiple chemical forms — arsenic trioxide (As₂O₃, white arsenic) is the classic homicidal poison; arsenite (As³⁺) and arsenate (As⁵⁺) are the biologically active forms; organic arsenicals are used in medications and pesticides (sodium arsenate, calcium arsenate).
Mechanism of toxicity:
Arsenic (especially arsenite, As³⁺) binds tightly to sulfhydryl (–SH) groups on cellular enzymes, inhibiting a wide range of metabolic enzymes. Key targets include:
- Pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase (Krebs cycle inhibition → impaired ATP production)
- Lipoic acid (a cofactor with two –SH groups — arsenic cross-links them, inactivating many enzymes)
- Endothelial damage → vascular permeability → the 'rice-water' stools of acute arsenism
Characteristic clinical features:
Acute arsenic poisoning:
- Garlic odour on breath (volatile arsines formed in vivo)
- Burning pain in mouth, throat, GI tract; profuse watery 'rice-water' diarrhoea (resembles cholera)
- Haemorrhagic gastroenteritis
- Cardiovascular collapse (peripheral vasodilatation)
Chronic arsenic poisoning (arsenicosis):
- Mees' lines — transverse white bands in fingernails (transverse white striae running across the full width of the nail); each line represents a period of arsenic exposure. Multiple lines = multiple exposures. The lines grow out distally with the nail — their distance from the nail bed indicates how long ago the exposure occurred (nail grows ~3 mm/month).
- Rain-drop pigmentation — areas of hyperpigmentation alternating with hypopigmentation on the trunk and extremities, giving a 'drops of rain on dusty ground' appearance
- Arsenical keratosis — hyperkeratosis of the palms and soles
- Peripheral neuropathy (predominantly sensory)
- Mees' lines may be the only clinical sign if the poisoning was intermittent
Post-mortem findings (acute):
- Garlic odour of all viscera
- Haemorrhagic gastroenteritis; erosion of gastric mucosa
- Fatty degeneration of liver and kidney
- Marsh test (classic): arsenite converted to arsine gas by Zn + H₂SO₄ → arsine passes over heated tube → black mirror deposit of elemental arsenic. Reinsch test: copper strip placed in acidic solution of body fluid — arsenic deposits as silver-grey coating. Modern analysis: atomic absorption spectroscopy (AAS) or ICP-MS (inductively coupled plasma–mass spectrometry) on blood, urine, hair, and nails.
Treatment — arsenic:
- Gastric lavage (if early)
- Chelation: dimercaprol (BAL — British Anti-Lewisite) — first-line parenteral chelator; forms stable water-soluble complex with As³⁺ excreted in urine. Alternatively DMSA (succimer) — oral chelator for mild-moderate cases. D-penicillamine — third option
- Supportive: IV fluids, electrolyte replacement, cardiac monitoring
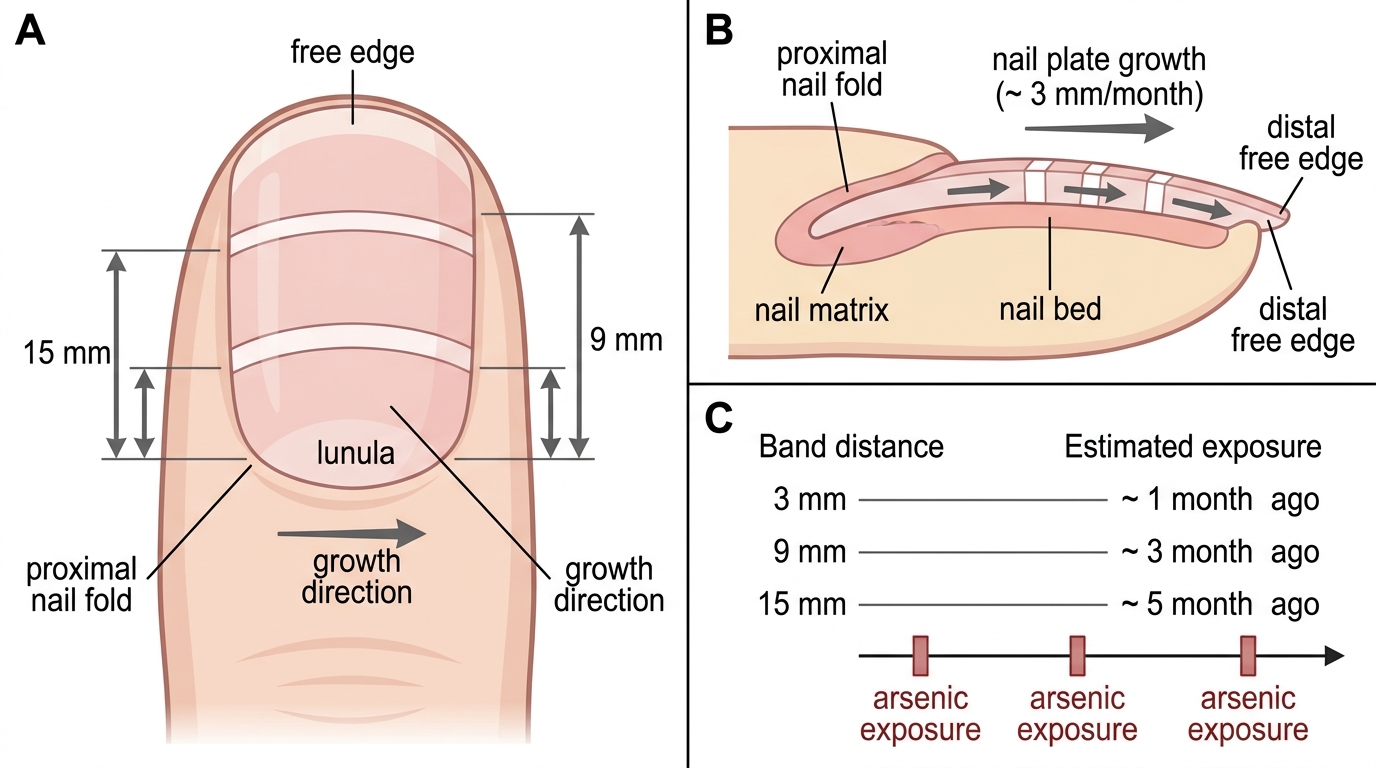
Mees' Lines and Chronological Dating of Arsenic Exposure
SELF-CHECK
A patient with chronic arsenic poisoning shows three transverse white bands across all fingernails at distances of 3 mm, 9 mm, and 15 mm from the nail fold. If nail grows at approximately 3 mm/month, what is the most accurate interpretation?
A. One episode of arsenic exposure occurring 5 months ago
B. Three separate episodes of arsenic exposure at approximately 1, 3, and 5 months ago
C. Continuous arsenic exposure for 5 months producing three bands
D. Mees' lines indicate a single massive arsenic dose; multiple bands indicate chronic liver disease
Reveal Answer
Answer: B. Three separate episodes of arsenic exposure at approximately 1, 3, and 5 months ago
Mees' lines (transverse white bands) each represent a discrete episode of arsenic exposure. The nail grows at approximately 3 mm/month, so a band at 3 mm = 1 month ago, at 9 mm = 3 months ago, at 15 mm = 5 months ago — three separate poisoning events. Continuous exposure would not typically produce three discrete bands; it would produce broader or diffuse nail changes. Mees' lines are specific to arsenic (and occasionally other heavy metal) exposure, not liver disease (Muehrcke's lines — double white bands — are associated with hypoalbuminaemia/liver disease but are structurally distinct).
Lead, Mercury, Copper and Iron: Key Features
The remaining four metals each have distinct toxicokinetic profiles, characteristic clinical markers, and specific chelation strategies. For FM13.13, the forensic medicine graduate must recognise their clinical and post-mortem signatures and apply the appropriate treatment framework.
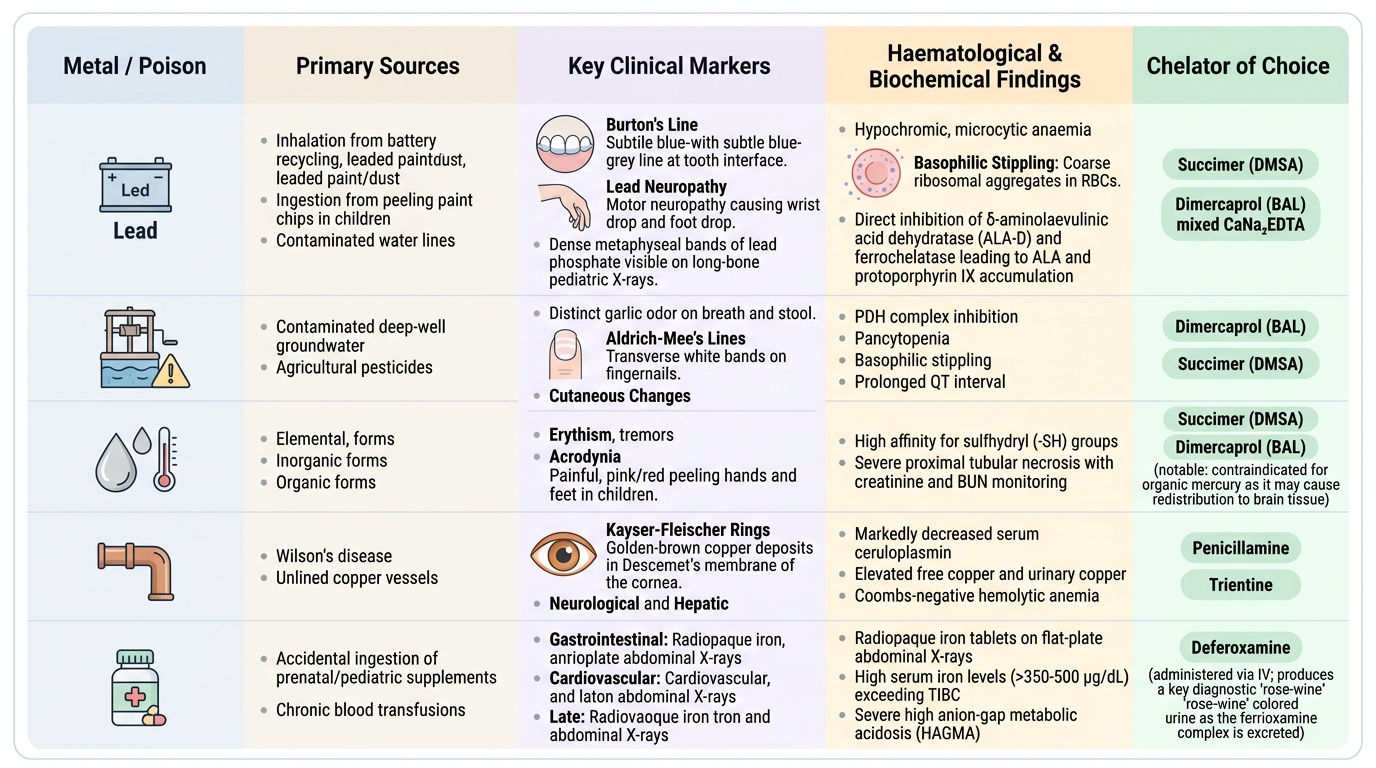
LEAD (Plumbism):
Lead is absorbed via inhalation (fumes from battery recycling, painting), ingestion (leaded paint chips in children, contaminated water), and occasionally skin. It distributes to blood → soft tissue → bone (where 90% of lead is stored as lead phosphate in the metaphyses — the 'lead lines' on X-ray in children). Lead has a very long biological half-life in bone (~27 years).
Mechanism: inhibits ALA dehydratase (delta-aminolaevulinic acid dehydratase, ALA-D) and ferrochelatase — two key enzymes of haem synthesis — producing accumulation of ALA and protoporphyrin IX; results in hypochromic, microcytic anaemia with basophilic stippling (coarse basophilic granules in red blood cells = aggregated RNA from ribosomal inhibition).
Characteristic features:
- Burton's line — a blue-black line along the gingival margin (precipitated lead sulphide; only in people with poor dental hygiene who have enough oral bacteria to convert absorbed lead to lead sulphide)
- Wrist drop and foot drop (lead neuropathy — motor-predominant, due to segmental demyelination of radial/common peroneal nerves)
- Basophilic stippling on peripheral blood film (pathognomonic for heavy metal interference with erythropoiesis)
- Encephalopathy in children (cerebral oedema; lead crosses BBB in children more than adults)
- Radiological lead lines — dense metaphyseal bands visible on X-ray of long bones in children (due to lead phosphate deposition at the growth plate)
Treatment: EDTA (ethylene diamine tetraacetic acid, calcium disodium EDTA) — first-line chelator for lead; IV for encephalopathy; if blood lead >45 µg/dL in children. DMSA (succimer) — oral chelator, preferred for blood lead 25–44 µg/dL.
MERCURY:
Mercury exists in three forms with different toxicity profiles:
- Elemental mercury (Hg⁰): vapour inhaled → pulmonary absorption → CNS (tremor, erethism — 'mad as a hatter')
- Inorganic mercury salts (HgCl₂, mercuric chloride): highly corrosive on ingestion; nephrotoxic (proximal tubular necrosis — 'mercuric nephritis')
- Organic mercury (methylmercury): most neurotoxic — crosses BBB and placenta; causes cortical atrophy, cerebellar degeneration, peripheral neuropathy (Minamata disease, Japan, 1950s)
Characteristic features:
- Erethism — mercury encephalopathy: excessive shyness, social withdrawal, memory impairment, insomnia (in occupational exposure to elemental mercury vapour)
- Tremor (mercurial tremor — intention tremor)
- Gingivostomatitis — spongy, bleeding gums with blue-black discolouration (mercury deposits in gum tissue)
- Hunter-Russell syndrome — organic mercury neurotoxicity: ataxia, dysarthria, constricted visual fields, paraesthesia
Treatment: dimercaprol (BAL) for inorganic mercury; DMSA for organic; sodium thiosulphate; supportive renal support.
COPPER:
Copper sulphate (CuSO₄, blue vitriol) is the forensically relevant form — available as fungicide/pesticide, historically used in homicide and suicide in India. Mechanism: Cu²⁺ inhibits –SH enzymes; direct GI corrosion; causes haemolysis (RBC membrane damage → haemolytic anaemia → haemoglobinuria → renal failure).
Characteristic features: blue-green vomitus (copper sulphate colour); metallic taste; jaundice (haemolysis); haemoglobinuria (port-wine urine).
Treatment: gastric lavage with potassium ferrocyanide (precipitates copper); D-penicillamine (chelator of choice for copper); BAL as second-line.
IRON (acute overdose — paediatric primarily):
Acute iron overdose follows a four-phase course similar to phosphorus:
- Phase 1 (0–6 h): direct GI corrosion — haemorrhagic vomiting, diarrhoea, haematemesis
- Phase 2 (6–24 h): latent (apparent improvement)
- Phase 3 (12–48 h): systemic toxicity — metabolic acidosis, hepatic failure, cardiovascular shock (free iron catalyses free radical production via Fenton reaction)
- Phase 4 (2–8 weeks): GI stricture formation from healing necrosis
Characteristic: haemorrhagic GI symptoms; serum iron >500 µg/dL = severe toxicity.
Treatment: deferoxamine (desferrioxamine) — specific chelator for iron; IV in severe cases; forms ferrioxamine excreted in urine (gives urine a 'vin rosé'/pink-orange colour — confirms chelation is working). Gastric lavage if early; whole-bowel irrigation with polyethylene glycol.
Provided image
SELF-CHECK
A 5-year-old child is brought with obtundation and haemorrhagic vomiting after ingesting iron tablets. Serum iron is 650 µg/dL. Which chelator and which monitoring endpoint (to confirm chelation is working) is correct?
A. Dimercaprol (BAL); monitor for decrease in blood pressure
B. Deferoxamine; urine turns pink-orange (vin rosé colour) indicating active chelation
C. EDTA; urine contains lead-EDTA complex (dark deposits)
D. D-penicillamine; copper-penicillamine complex in serum
Reveal Answer
Answer: B. Deferoxamine; urine turns pink-orange (vin rosé colour) indicating active chelation
Deferoxamine (desferrioxamine) is the specific chelator for acute iron toxicity. When deferoxamine binds free iron it forms ferrioxamine, which is renally excreted and turns the urine a distinctive pink-orange ('vin rosé') colour — this is the clinically useful monitoring endpoint confirming active chelation. EDTA is for lead; BAL for arsenic/mercury; D-penicillamine for copper/lead (oral, second-line).