Page 8 of 33
FM13.13 | Metallic Poisons (Arsenic, Lead, Mercury, Copper, Iron) — SDL Guide (Part 2)
Clinical Examination, Documentation and Analytical Methods
The forensic examination of a patient with suspected metallic poisoning must systematically search for the pathognomonic signs described above and document them contemporaneously for medicolegal purposes.
Clinical examination priorities:
- Nails: inspect for Mees' lines (arsenic) — use hand lens if available; document distance from nail fold and width of each band
- Gingiva: Burton's line (lead — blue-black gingival margin); mercury gingivostomatitis
- Skin: rain-drop pigmentation, arsenical keratosis of palms/soles (arsenic); pallor from anaemia (lead, arsenic, copper)
- Neurological: wrist drop/foot drop (lead); tremor/erethism (mercury); peripheral numbness/stockings-gloves pattern (arsenic, mercury)
- Urine: colour (haemoglobinuria in copper — port-wine; vin rosé in deferoxamine-treated iron; dark in mercury nephritis)
- Blood film (if available): basophilic stippling (lead)
Investigations to order and document:
- Blood metal levels (whole blood for lead; serum for arsenic, mercury, copper)
- Urine metal levels (arsenic — 24-h urine; mercury — spot urine creatinine ratio)
- Hair and nail analysis (arsenic — historical exposure; Mees' lines are clinical but nail clippings for AAS are the forensic standard)
- Blood count and film (basophilic stippling, haemolytic anaemia)
- LFT, RFT, ABG (multi-organ assessment)
- Nerve conduction studies (if available, for lead/arsenic neuropathy)
Forensic sampling:
For post-mortem: blood (femoral), liver, kidney, stomach contents (if undigested), hair, and nail clippings should all be collected and preserved separately in clean, sealed containers. Arsenic distributes to all tissues; hair and nail archiving allows temporal reconstruction of exposure episodes.
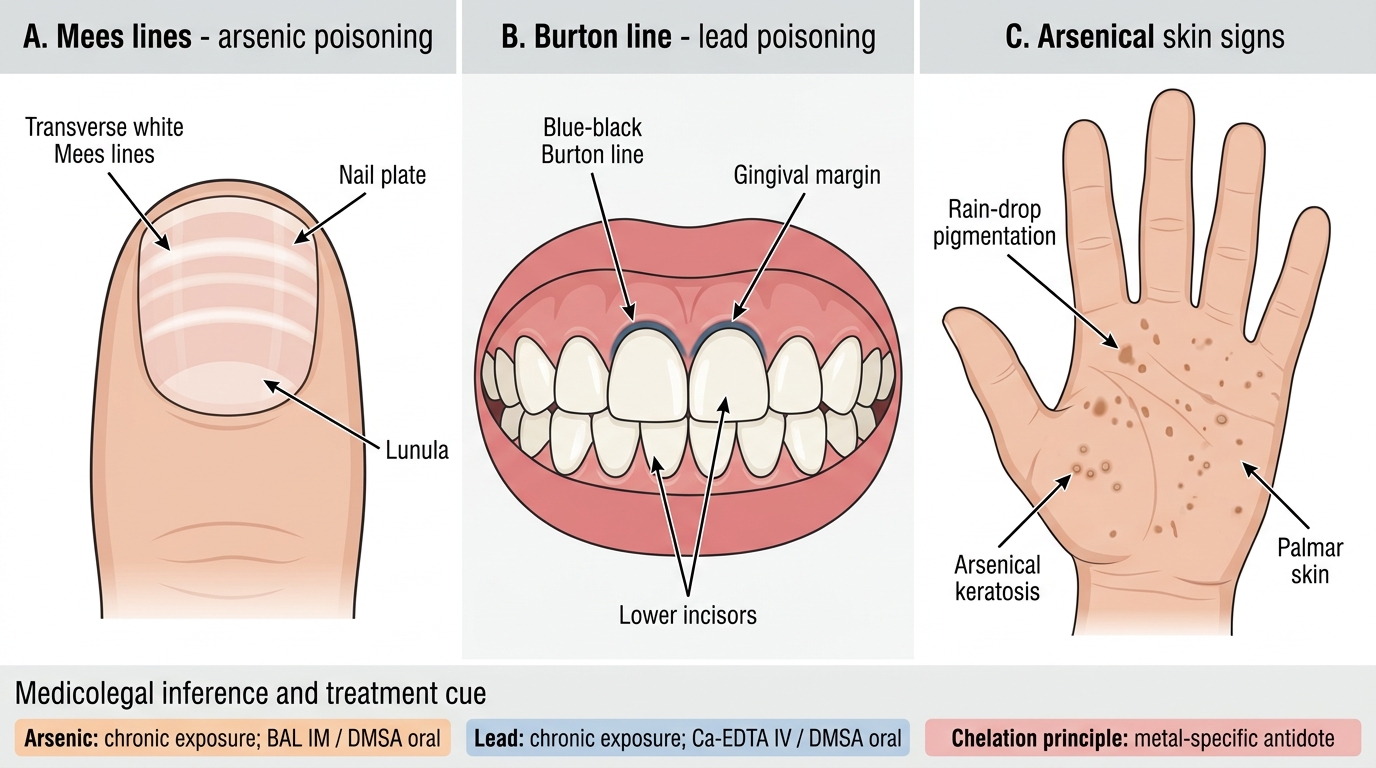
Pathognomonic Signs of Metallic Poisoning
Medicolegal Inference and Treatment Framework
The treatment framework for metallic poisons is unified by the principle of chelation, but with metal-specific modifications:
| Metal | First-line chelator | Route | Key note |
|---|---|---|---|
| Arsenic | Dimercaprol (BAL) | IM | DMSA (oral) for mild/chronic |
| Lead | Ca-EDTA | IV | DMSA (oral) for blood lead 25–44 µg/dL |
| Mercury | Dimercaprol (BAL) | IM | DMSA for organic mercury; support renal |
| Copper | D-penicillamine | Oral | Gastric potassium ferrocyanide lavage |
| Iron | Deferoxamine | IV/IM | Vin rosé urine confirms working |
General principles across all metals:
- Decontamination first (gastric lavage if early ingestion, within 1–2 hours)
- Supportive care (fluids, cardiac monitoring, renal support)
- Chelation (metal-specific as above)
- Enhanced elimination: haemodialysis for severe arsenic, lead, mercury nephrotoxicity; aids removal of small metal-chelate complexes; forced diuresis for iron-deferoxamine
Medicolegal inference:
For chronic arsenic poisoning: key questions for the MLR — who had access to the food/drink? Was the source identifiable (well water, pesticide, herbal product)? Can the Mees' lines timing be correlated with the victim's social history?
For occupational lead/mercury: report must distinguish occupational disease (a civil/compensation matter) from criminal exposure. Document workplace, duration of exposure, PPE use, and employer compliance with occupational safety regulations.
Relevant statutes:
- IPC §328: causing hurt by poison — administering a poison with intent to hurt
- IPC §302/304: if death results
- Factories Act 1948 and occupational safety regulations (relevant to lead/mercury workplace exposure)
- Environmental Protection Act 1986 (arsenic/mercury contamination of water supplies)
Analytical confirmation — key tests:
- Marsh test (arsenic): classic qualitative test; now supplemented by AAS/ICP-MS
- Reinsch test (arsenic, mercury, antimony): metal deposits on copper strip from acidified solution
- Spectrometric analysis (all metals): AAS and ICP-MS are the current gold standard for quantitative metal levels in biological specimens
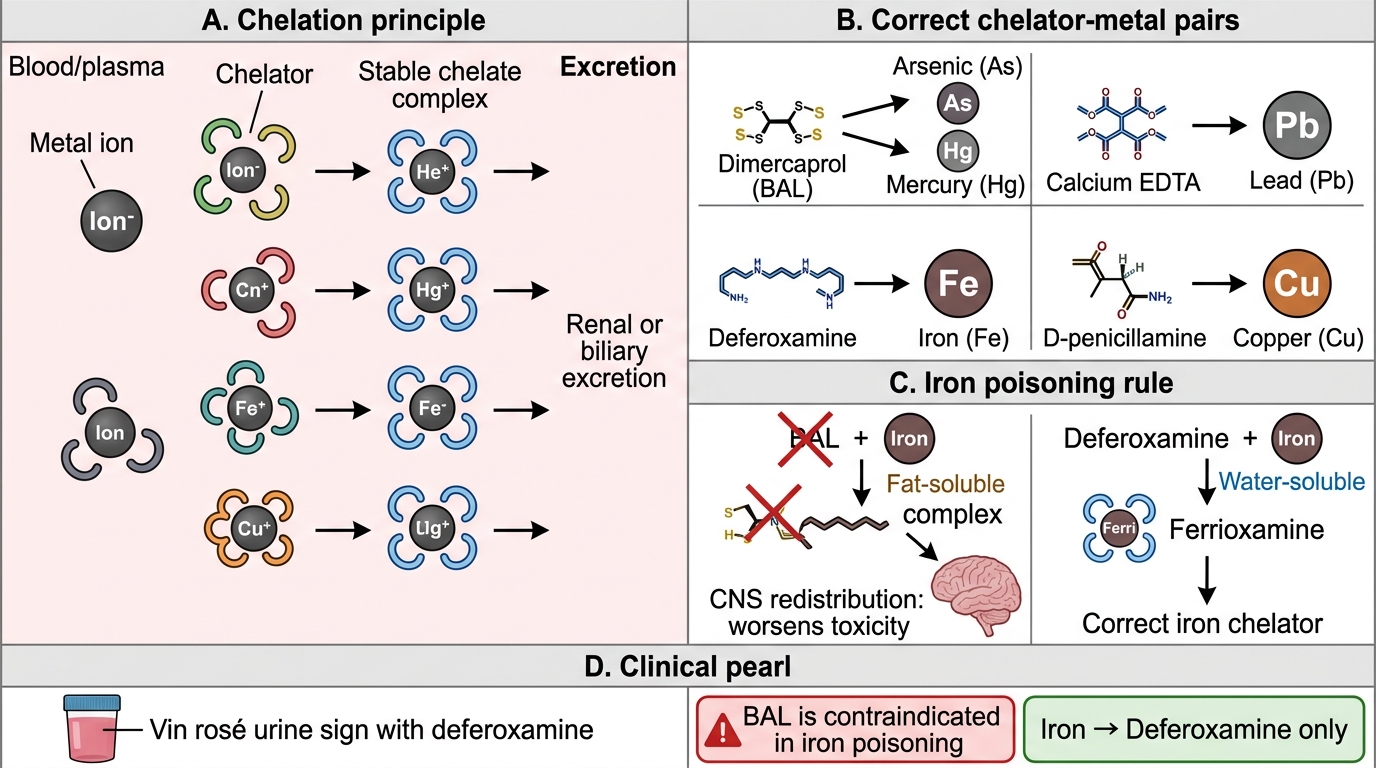
Chelation Therapy for Metallic Poisons
CLINICAL PEARL
Dimercaprol (BAL) is contraindicated in iron poisoning. This is a critical and counter-intuitive fact: BAL is the go-to chelator for arsenic, lead, and mercury — but for iron, BAL actually redistributes iron to sensitive tissues (particularly the CNS), worsening toxicity. Deferoxamine is the specific and only appropriate chelator for iron. This distinction is a classic examination question, and the pharmacological reason (BAL forms a fat-soluble iron complex that penetrates cell membranes, unlike the water-soluble ferrioxamine formed by deferoxamine) is the basis for understanding the rule.
SELF-CHECK
Which of the following chelation pairs is CORRECT?
A. Iron — dimercaprol (BAL); Arsenic — deferoxamine
B. Lead — calcium EDTA; Copper — D-penicillamine; Arsenic — dimercaprol (BAL)
C. Mercury — deferoxamine; Lead — DMSA; Iron — EDTA
D. Arsenic — D-penicillamine; Iron — calcium EDTA; Lead — BAL
Reveal Answer
Answer: B. Lead — calcium EDTA; Copper — D-penicillamine; Arsenic — dimercaprol (BAL)
The correct assignments are: Lead → Ca-EDTA (IV) or DMSA (oral); Copper → D-penicillamine (oral); Arsenic → dimercaprol/BAL (with DMSA as oral alternative). Iron → deferoxamine ONLY (BAL is contraindicated for iron). Mercury → BAL or DMSA. Option B is the only one fully correct.