Page 4 of 33
FM13.12 | Phosphorus, Iodine & Barium — SDL Guide
Learning Objectives
- Describe the sources, forms and mechanisms of toxicity for yellow/white phosphorus, iodine, and barium compounds
- Explain the characteristic post-mortem appearances and clinical signs for each agent
- Apply the treatment framework (decontamination, supportive care, specific antidote/enhanced elimination) to phosphorus, iodine and barium poisoning
- Prepare a medicolegal report for suspected poisoning by these agents
INSTRUCTIONS
Phosphorus, iodine, and barium represent three chemically distinct but forensically important corrosive/toxic agents. Yellow phosphorus (rat poison) was historically one of the most common homicidal poisons in India; barium carbonate (as rat killer) is another agent of forensic significance. Understanding the unique pathological signatures of each — from phosphorus' hepatorenal failure to barium's potassium-independent hypokalaemia-like paralysis — is essential for both accurate clinical management and forensic inference.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A farmer from a rural district is brought unconscious to the emergency department 48 hours after a family argument during which he allegedly consumed rat poison. His family cannot produce the packet but describe it as a yellow, waxy substance that smelled like garlic. On examination he is jaundiced, has right upper quadrant tenderness, and his urine output has dropped to 200 mL in the last 12 hours. In the mortuary down the corridor, a post-mortem is about to begin on a 60-year-old woman who died after suspected poisoning — her liver, when sectioned, glows faintly in the dark. These two cases share the same poison. What is it, and what does it teach you about the forensic approach to this class of agents?
WHY THIS MATTERS
Yellow phosphorus, historically used in match-head paste and rodenticides, remains a forensically significant poison in rural India where rat bait preparations are accessible. Iodine and iodides, while used therapeutically, are toxic in overdose and were historically used in criminal poisoning. Barium compounds (particularly barium carbonate, used in rat poisons) continue to cause both accidental and suicidal poisoning. Each of these agents is covered in the NMC FM13.12 competency because they require specific forensic recognition, management decisions, and medicolegal reporting that differ from the general corrosive acid framework.
RECALL
Activate your Year-1 knowledge:
- From Biochemistry: phosphorus is a central element in ATP synthesis (phosphorylation), membrane phospholipids, and DNA/RNA. Disruption of hepatic phospholipid metabolism causes fatty degeneration — a key pathological finding in phosphorus poisoning.
- From Physiology: potassium physiology — normal serum K⁺ 3.5–5.0 mEq/L; hypokalaemia (K⁺ <3.5) causes flaccid paralysis (ascending, like Guillain-Barré pattern); cardiac arrhythmia; and rhabdomyolysis. Barium poisoning affects potassium dynamics.
- From Pathology: fatty degeneration (steatosis) of the liver — accumulation of triglycerides within hepatocytes visible as cytoplasmic vacuoles on H&E; central to phosphorus hepatotoxicity.
- From Biochemistry: the thyroid's iodine biology — iodide uptake by sodium-iodide symporter (NIS), organification to form thyroid hormones; excess iodide blocks thyroid hormone synthesis (Wolff-Chaikoff effect).
Medicolegal Context: Phosphorus, Iodine and Barium as Forensic Poisons
The medicolegal significance of this group of agents arises from several converging factors. First, they are accessible — yellow/white phosphorus is found in rat poisons (though now partially regulated), barium carbonate in rodenticides, and iodine as a household antiseptic and pharmaceutical agent. Second, they produce characteristic and recognisable signs — the phosphorescent glow of phosphorus in the dark, the blue-black iodine stain, the flaccid paralysis of barium — that allow clinical and forensic identification even before analytical toxicology results are available.
Historically in India, yellow phosphorus (from match-head scrapings and rat poison paste) was one of the most notorious homicidal poisons, particularly because the method of administration was domestic — the poison was added to food. The same accessibility that made it common in homicide makes it common in suicide in agricultural communities today. The forensic doctor may encounter:
- A living patient with insidious hepatorenal failure following clandestine ingestion
- A post-mortem with characteristic glowing liver and garlic-smelling viscera
- A death certificate challenge — phosphorus poisoning can mimic viral hepatitis or acute liver failure
Barium poisoning most often occurs from barium carbonate (rat poison) mistaken for edible substances (barium carbonate resembles flour), or from industrial exposure. Forensic significance: the rapid ascending paralysis pattern may be mistaken for other neurotoxic poisonings (snake envenomation, organophosphate).
Iodine poisoning (acute high-dose ingestion) is less common but produces a distinctive clinical picture combining corrosive injury (mucosal burns, metallic taste) and systemic iodism that has forensic significance if the substance was administered without consent.
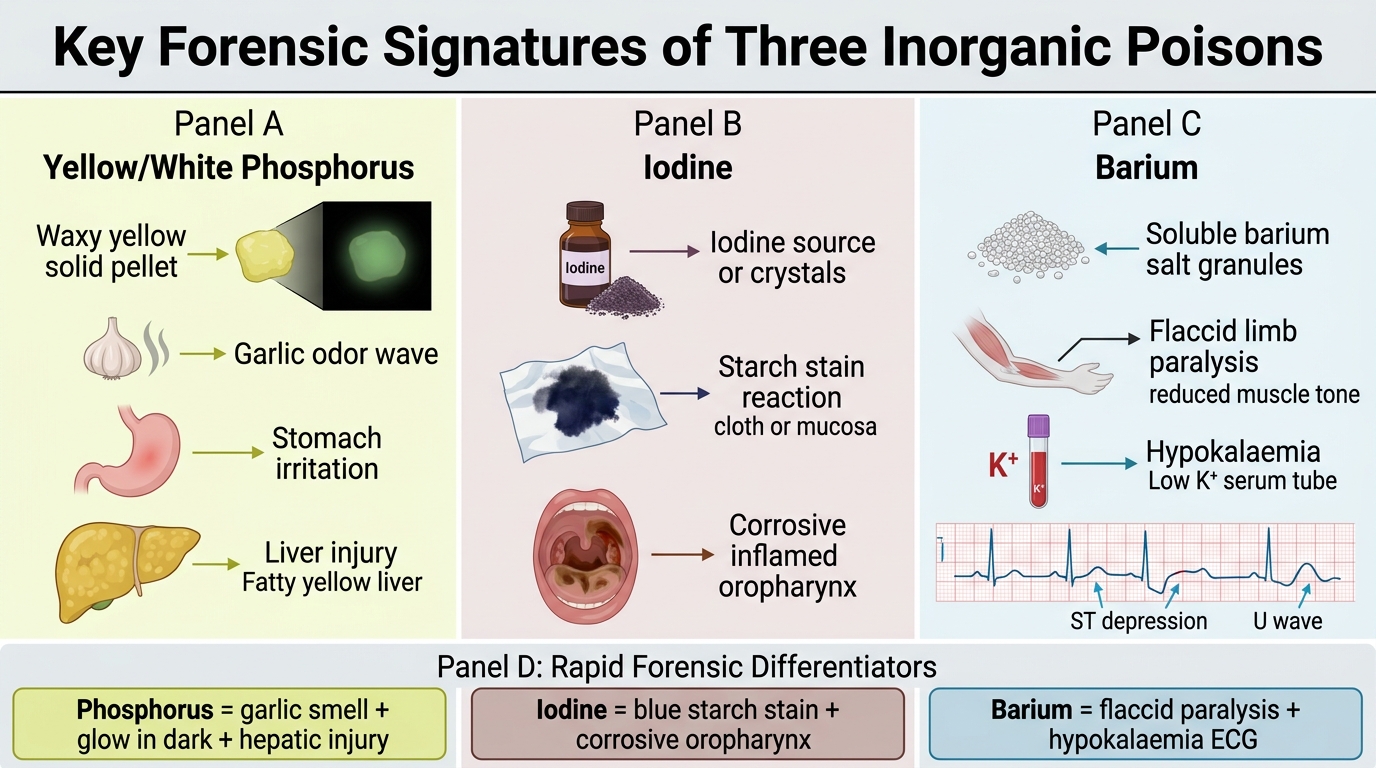
Forensic Signatures of Yellow Phosphorus, Iodine, and Barium
Yellow/White Phosphorus: Toxicokinetics and Pathological Basis
Phosphorus exists in two primary allotropes relevant to toxicology: yellow/white phosphorus (the toxic, pyrophoric form) and red phosphorus (essentially non-toxic). The terms yellow and white phosphorus refer to the same allotrope — yellow is the common name; white is its appearance in pure form. All references to 'phosphorus poisoning' in forensic toxicology mean yellow/white phosphorus, not red phosphorus.
Yellow phosphorus is a waxy, translucent-to-yellow solid that:
- Smells of garlic (characteristic odour — important clinical and forensic identifier)
- Glows in the dark (phosphorescence — self-oxidation in air produces faint greenish luminescence)
- Catches fire spontaneously in air at room temperature (pyrophoric)
- Is found in rat poisons, fireworks, and certain pesticide preparations
Toxicokinetics:
Absorbed through the gastrointestinal mucosa and skin. Hepatic first-pass metabolism is minimal — phosphorus is directly toxic to cellular organelles. It undergoes oxidation to phosphoric and hypophosphorous acids in vivo.
Mechanism of toxicity — three-phase clinical course:
Phase 1 (first 24 hours): Direct GI corrosive effect — nausea, vomiting, diarrhoea; the vomitus and faeces may be luminescent (glow in the dark). This phase may partially subside ('well period') before phase 2.
Phase 2 (latent/asymptomatic, 24–48 hours in some cases): Relative clinical improvement — dangerous because it may lead to premature discharge or delay in diagnosis.
Phase 3 (48–96 hours onwards): Systemic toxicity — hepatic fatty degeneration and necrosis (jaundice, elevated transaminases, coagulopathy), acute renal failure (tubular necrosis), cardiovascular collapse (arrhythmia, hypotension), CNS depression.
Characteristic post-mortem findings:
- Liver: enlarged, yellow, fatty (steatosis + necrosis); the classic sign is phosphorescence — when the liver is examined in a darkened room, it emits a faint greenish glow
- Garlic odour of all viscera and the body
- Yellow/waxy phosphorus deposits may be visible in the stomach
- Fatty degeneration of myocardium and kidneys
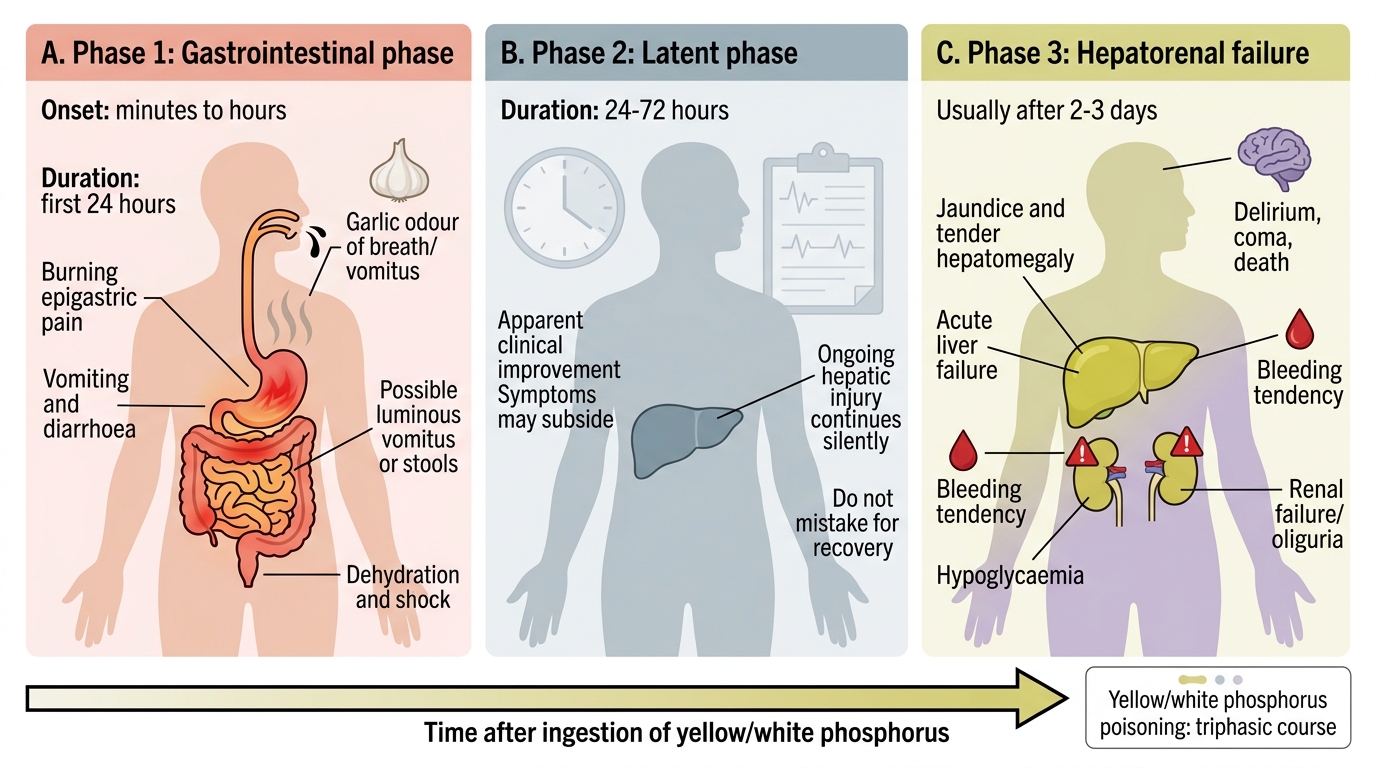
Three-Phase Clinical Course of Phosphorus Poisoning
SELF-CHECK
The post-mortem liver of a suspected poisoning case glows faintly green when examined in a darkened room. The viscera have a garlic odour. Which poison is most consistent with these findings?
A. Arsenic
B. Yellow phosphorus
C. Barium carbonate
D. Oxalic acid
Reveal Answer
Answer: B. Yellow phosphorus
Phosphorescence of the liver (faint greenish glow in the dark) and garlic odour of the viscera are pathognomonic of yellow/white phosphorus poisoning. Arsenic causes garlic odour but NO phosphorescence. Barium and oxalic acid do not produce either finding.
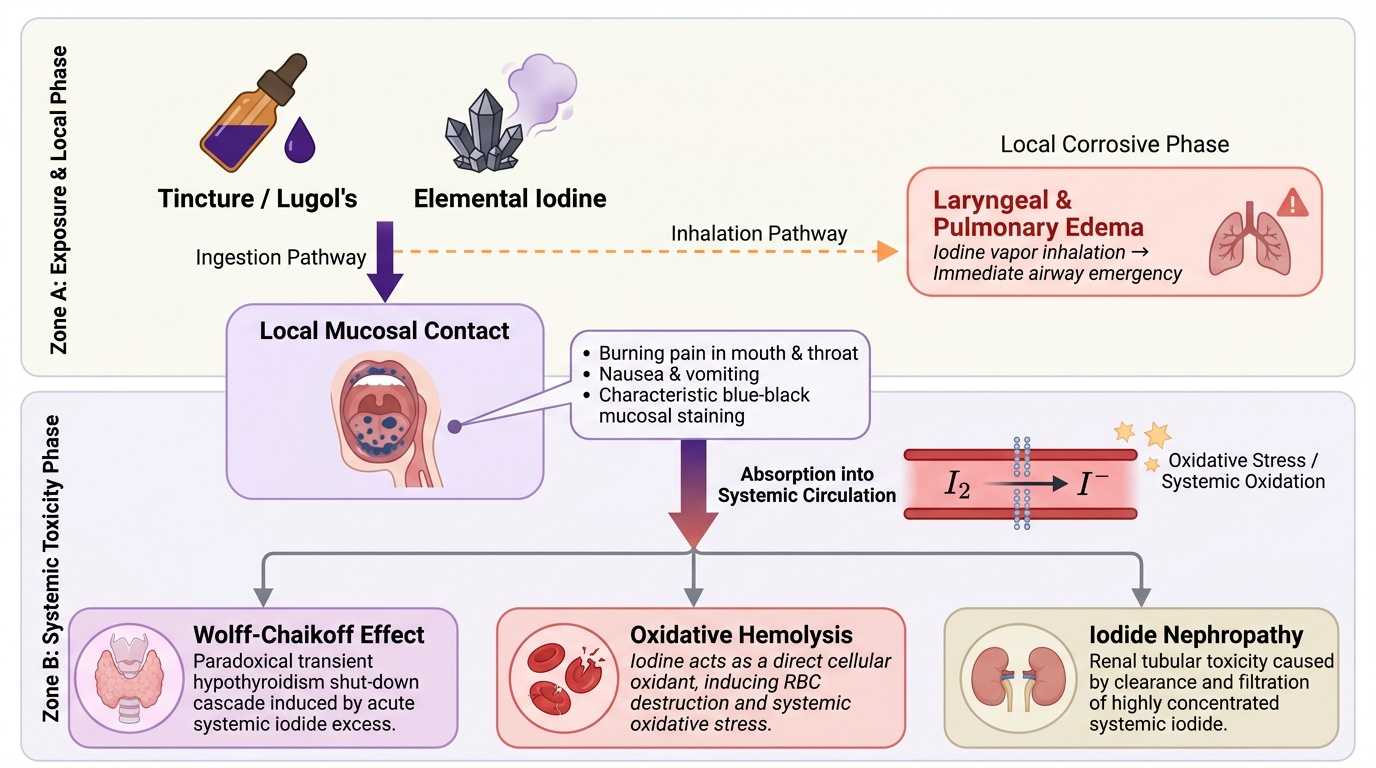
Iodine Poisoning: Mechanism and Recognition
Iodine toxicity is relevant to forensic medicine in two forms: acute ingestion of elemental iodine (corrosive-systemic syndrome) and chronic iodism (excessive medicinal iodide intake). The NMC competency focuses on the forensic recognition and management of acute iodine poisoning.
Elemental iodine (I₂) is a dark grey crystalline solid that sublimes to produce a distinctive violet-coloured vapour with a sharp, characteristic smell. Commercial preparations (tincture of iodine 2–5%, Lugol's iodine) are the most commonly ingested forms.
Mechanism of toxicity:
- Local corrosive effect: Iodine reacts with mucous membrane proteins to form the characteristic blue-black (iodo-protein) discolouration of the mouth, tongue, and lips — this staining is a valuable clinical and forensic identifier. Burning pain in mouth/throat, nausea, vomiting.
- Systemic toxicity: Absorbed iodine acts as an oxidant, causing haemolysis, renal tubular toxicity (iodide nephropathy), and — via the Wolff-Chaikoff mechanism — paradoxical transient hypothyroidism.
- Laryngeal oedema: Iodine vapour inhalation causes laryngeal/pulmonary oedema — an immediate airway emergency.
Characteristic features for forensic recognition:
- Blue-black staining of mucous membranes, tongue, and lips
- Yellow-brown staining of vomitus and faeces (iodine-starch complex on food residue)
- Characteristic smell (iodine/antiseptic odour)
- Metallic/bitter taste (patient history)
Iodism (chronic): Coryza-like syndrome (runny nose, salivation, skin rash — 'iodide rash'), hypothyroidism, metallic taste; not typically a forensic emergency but may present as unexplained chronic illness where medication history reveals high iodide intake.
Treatment:
- Starch solution or milk as antidote (starch binds iodine; milk protein precipitates it)
- Gastric lavage with sodium thiosulphate solution (converts I₂ to iodide, reducing corrosive potential)
- Supportive care; airway management if inhaled
Provided image