Page 5 of 33
FM13.12 | Phosphorus, Iodine & Barium — SDL Guide (Part 2)
Barium Poisoning: Mechanism, Clinical Features and Forensic Significance
Barium compounds vary widely in toxicity. Barium sulphate (BaSO₄) is completely insoluble and non-toxic — hence its safe use as a radiological contrast medium. Barium carbonate (BaCO₃) and barium chloride (BaCl₂), however, are water-soluble and highly toxic. Barium carbonate has forensic significance as a rodenticide (rat poison) that is easily confused with flour or cornstarch in appearance, making accidental (and deliberate) contamination of food a documented forensic pattern.
Mechanism of toxicity:
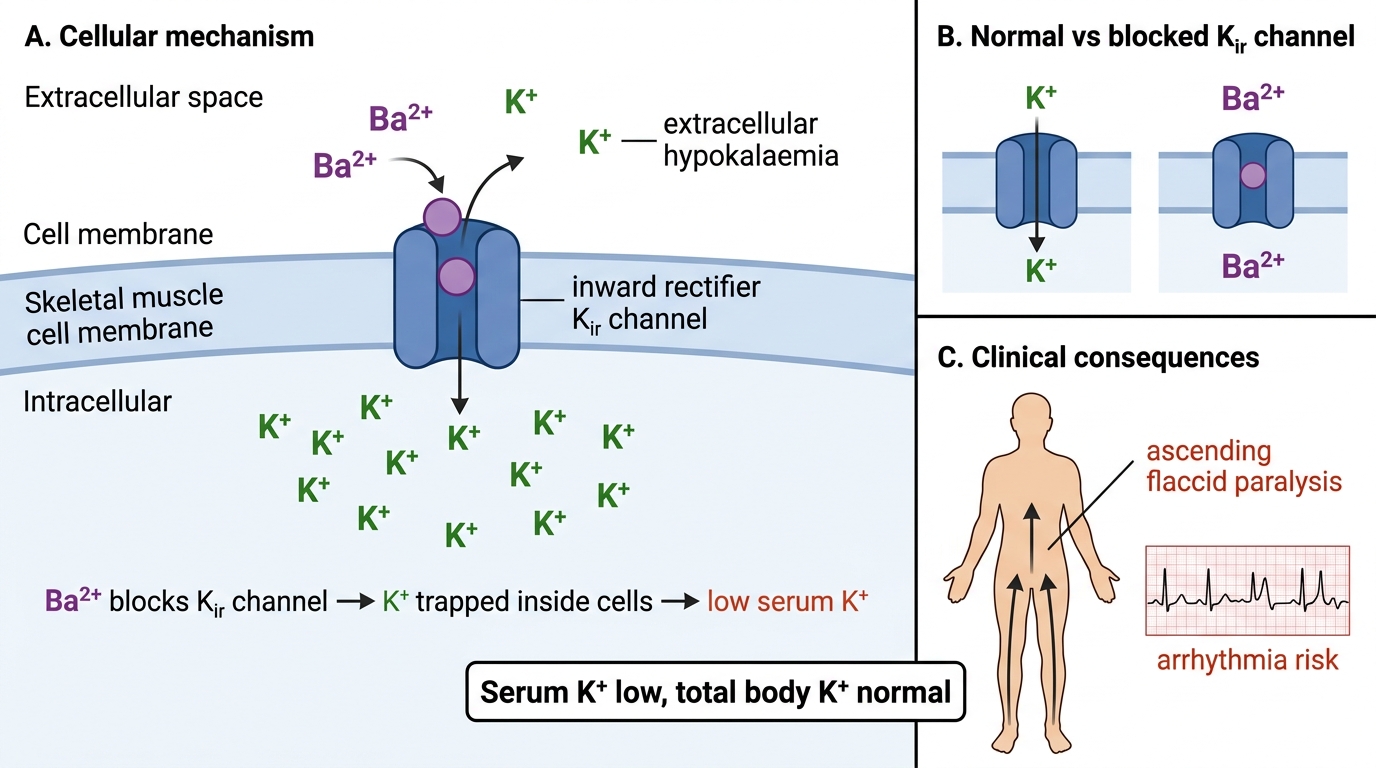
Barium ions (Ba²⁺) are taken up into cells via calcium channels and potassium-sensitive membrane pumps. The primary toxic mechanism is blockade of potassium channels (specifically K_ir channels — inwardly rectifying K⁺ channels), preventing K⁺ efflux from cells. This traps K⁺ inside cells, producing a dramatic hypokalaemia (decreased extracellular K⁺), even though total body potassium is NORMAL. This is a critical forensic-pharmacological distinction: the hypokalaemia of barium poisoning is NOT due to K⁺ loss but to intracellular shift.
Clinical features — the barium poisoning triad:
1. Ascending flaccid paralysis (from profound hypokalaemia — muscle weakness beginning in legs, ascending to trunk, intercostals, diaphragm → respiratory failure)
2. Cardiac arrhythmias (hypokalaemia → prolonged QT, ventricular fibrillation)
3. GI symptoms (early — nausea, vomiting, diarrhoea, colicky abdominal pain)
The paralysis can be so rapid and severe that respiratory arrest may occur within hours of ingestion. This pattern can clinically resemble ascending neurotoxic snake envenomation or Guillain-Barré syndrome — the serum potassium result (very low despite no obvious K⁺ loss) distinguishes barium poisoning.
Post-mortem findings:
No pathognomonic gross PM finding — diagnosis depends on analytical toxicology (stomach content analysis, blood/urine barium levels). Histology may show myocardial and skeletal muscle changes from hypokalaemia-related injury.
Treatment:
- IV potassium chloride (urgent — correct hypokalaemia to reverse paralysis)
- Oral/gastric sodium or magnesium sulphate (forms insoluble barium sulphate in GI tract, preventing further absorption — decontamination by precipitation)
- Cardiac monitoring and supportive care; mechanical ventilation if respiratory failure
- Enhanced elimination: IV fluids with forced diuresis
Mechanism of Barium Poisoning
SELF-CHECK
A patient brought in unconscious with a history of consuming food that 'tasted like flour' develops ascending flaccid paralysis and serum K⁺ of 1.8 mEq/L despite no history of vomiting or diarrhoea. The most appropriate immediate treatment is:
A. IV calcium gluconate
B. IV potassium chloride with cardiac monitoring
C. Atropine 1–2 mg IV
D. Activated charcoal 50 g orally
Reveal Answer
Answer: B. IV potassium chloride with cardiac monitoring
Barium carbonate (rat poison) blocks K_ir channels, causing intracellular K⁺ trapping → severe extracellular hypokalaemia (here 1.8 mEq/L). The ascending paralysis and history of flour-like contaminated food are characteristic. Immediate IV potassium chloride is life-saving (reverses paralysis and prevents fatal arrhythmia). Calcium gluconate is for hypocalcaemia/calcium channel-related toxicity; atropine is for organophosphate poisoning; activated charcoal would have only minor benefit at this stage after symptom onset.
Clinical Examination, Documentation and Treatment
Examining a patient with suspected phosphorus, iodine, or barium poisoning requires integration of the specific clinical signatures described above with the general approach to poisoning documentation.
History taking: Time of ingestion, substance description (waxy yellow/garlic smell for phosphorus; blue-staining antiseptic for iodine; white powder/flour-like for barium), quantity, mode (accidental/deliberate/witnessed), treatment already given.
Examination priorities by agent:
Phosphorus: Focus on hepatic examination (tender, enlarged liver; jaundice; coagulopathy signs — bleeding gums, ecchymoses); renal (oliguria, anuria); and examine vomitus/faeces for luminescence (perform in darkened room). Document all findings with timing.
Iodine: Examine mucous membranes for the blue-black staining; assess airway (iodine vapour → stridor, laryngeal oedema); document the characteristic smell on breath/clothing.
Barium: Neurological examination with focus on muscle power (ascending pattern); respiratory assessment (intercostal/diaphragmatic weakness = emergency); cardiac rhythm (bedside ECG — prolonged QT, ventricular arrhythmia pattern).
Investigations to order and document:
- All three: blood for toxicological analysis (to analytical lab with proper chain of custody)
- Phosphorus: LFT, PT/INR, serum creatinine, urinalysis
- Barium: serum electrolytes (K⁺ critical), ABG, 12-lead ECG, chest X-ray
- Iodine: serum iodine (if available); urinary iodine; TFT if chronic
Sampling for forensic analysis:
Collect and preserve as per standard procedure — gastric aspirate (first priority), blood (10 mL in fluoride-oxalate tube), urine (50 mL), vomitus with proper labelling and signed chain-of-custody documentation.
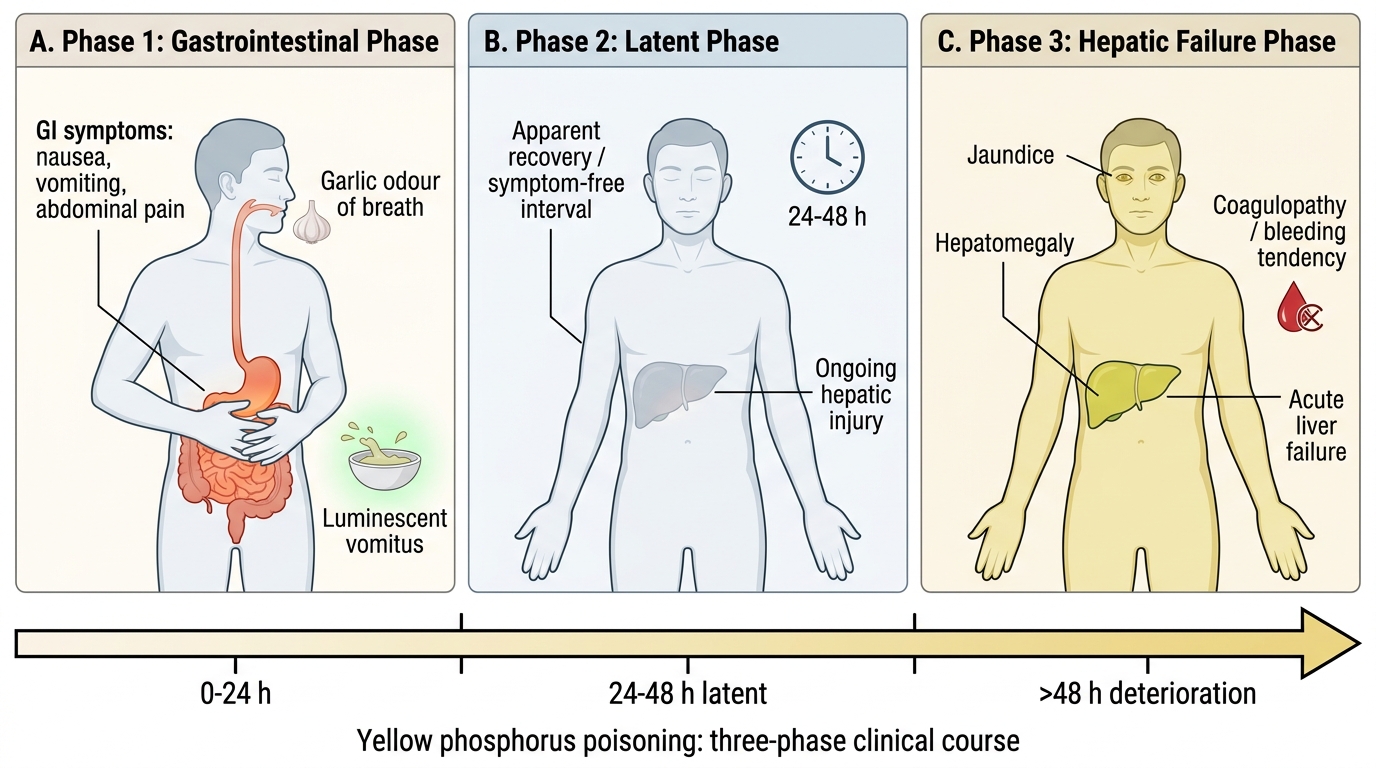
Three-Phase Course of Yellow Phosphorus Poisoning
Medicolegal Inference, Treatment Summary and Statutory Framework
The management framework — decontamination, supportive care, specific antidote, enhanced elimination — applies with agent-specific modifications.
Phosphorus:
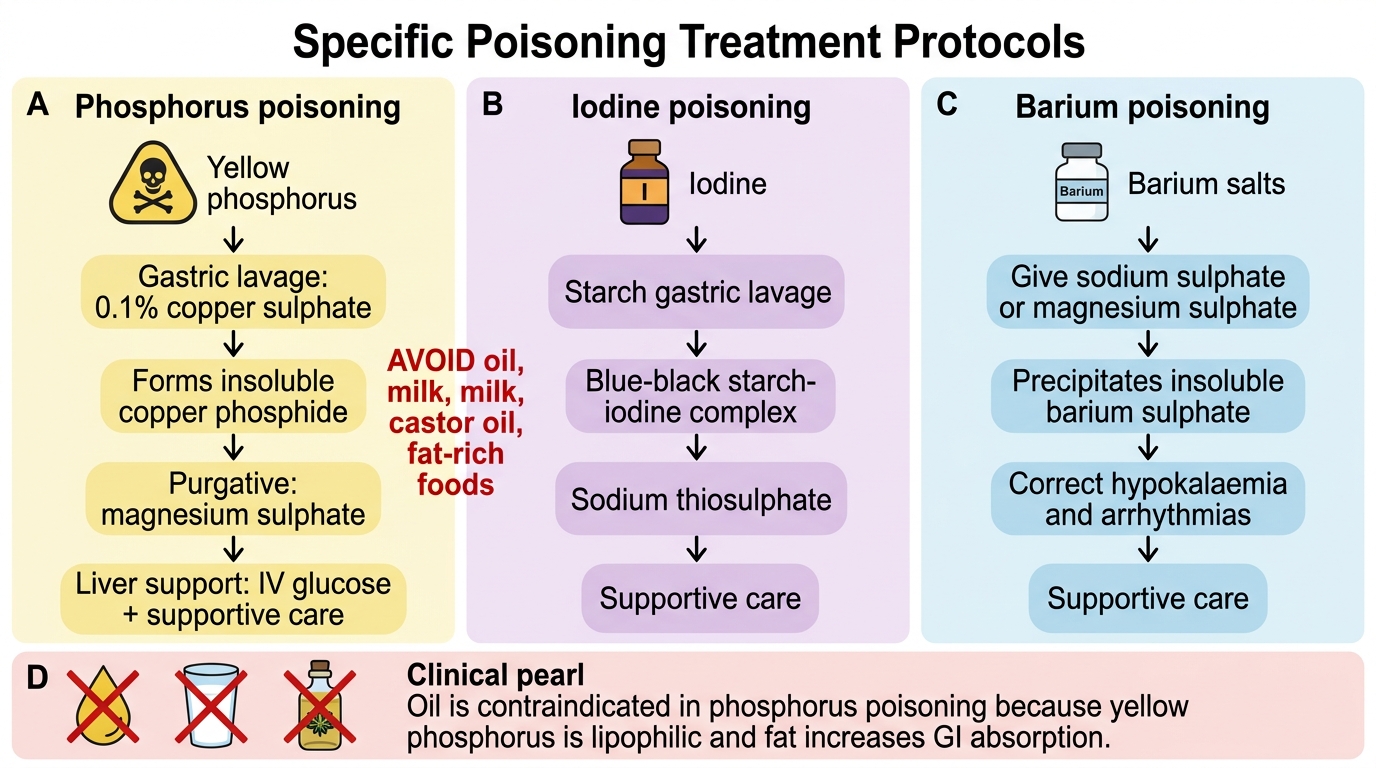
- Decontamination: gastric lavage with 0.1% copper sulphate solution (forms insoluble copper phosphide; also helpful for identification — produces a dark precipitate confirming phosphorus). Magnesium sulphate as a purgative to hasten elimination of unabsorbed phosphorus.
- Supportive: liver support (IV fluids, glucose, vitamin K; N-acetylcysteine as hepatoprotectant)
- No specific antidote for absorbed phosphorus
- Enhanced elimination: haemodialysis for acute renal failure (supportive)
- Avoid: oil (fat/oil enhances phosphorus absorption — no oil-based laxatives, no milk fat)
Iodine:
- Decontamination: starch solution (rice water, wheat paste) or milk by mouth — these precipitate/bind iodine
- Gastric lavage with 1% sodium thiosulphate (converts I₂ to sodium iodide, reducing corrosive effect)
- Supportive: airway management, IV fluids
- No specific antidote for systemic iodine
Barium:
- Decontamination: oral sodium sulphate or magnesium sulphate (forms insoluble barium sulphate in the gut)
- Specific antidote: IV potassium chloride (corrects the K⁺ channel block effect — not a true antidote but the definitive reversal strategy)
- Enhanced elimination: IV saline diuresis with monitoring
Medicolegal inference and report:
In homicidal phosphorus poisoning, key questions for the MLR:
- Was the phosphorus accessible to the deceased independently (suicide) or required another party's agency?
- Three-phase timeline — could the deceased have sought help during the latent phase?
- Was the characteristic garlic smell/luminescence documented by any witness before death?
For barium: the rapidity of paralysis onset (sometimes within 1–2 hours of ingestion) may be raised as evidence of intentional administration vs accidental contamination.
IPC relevance:
- Homicidal poisoning: IPC §302 (murder) or IPC §304 (culpable homicide not amounting to murder) depending on intent
- Culpable negligence (food contamination): IPC §304A (causing death by negligence)
- Section 174 CrPC: mandatory post-mortem in cases of unnatural death, which includes all homicidal/suspicious poisoning deaths
Treatment Protocols for Phosphorus, Iodine, and Barium Poisoning
CLINICAL PEARL
Oil is contraindicated in phosphorus poisoning. Yellow phosphorus is highly lipophilic — fat and oil dramatically enhance its GI absorption. This means milk (fat content), castor oil (traditionally used as a purgative), and oil-based preparations must be avoided in phosphorus poisoning management. Magnesium sulphate (Epsom salt) is the appropriate purgative. Similarly, avoid fat-rich foods in recovery. This contraindication is a classic examination question and a genuine clinical trap.
SELF-CHECK
In phosphorus poisoning, which of the following is CONTRAINDICATED in management?
A. Copper sulphate gastric lavage
B. Magnesium sulphate purgative
C. Castor oil or any oil-based purgative
D. IV glucose infusion
Reveal Answer
Answer: C. Castor oil or any oil-based purgative
Yellow phosphorus is highly lipophilic, and oil/fat (including castor oil) significantly enhances its GI absorption — administering any oil-based preparation can worsen toxicity. The appropriate purgative is magnesium sulphate (not oil-based). Copper sulphate lavage (0.1%) is the specific gastric lavage agent as it forms insoluble copper phosphide. IV glucose supports the liver. Castor oil is a classic contraindication trap in FM toxicology examinations.