Page 14 of 33
FM13.16 | Toxic & War Gases — SDL Guide
Learning Objectives
- Describe the toxicokinetics and mechanisms of toxicity of ammonia, carbon monoxide, hydrogen cyanide, methyl isocyanate, and tear/riot-control gases
- Identify the characteristic post-mortem findings for CO poisoning (cherry-red lividity) and cyanide poisoning
- Apply the specific antidote protocols for CO and cyanide poisoning
- Distinguish between CO cherry-red and cyanide cherry-red using history and forensic context
- Describe the forensic significance of the Bhopal gas tragedy (MIC) in Indian forensic and public-health law
INSTRUCTIONS
Toxic gas exposures represent some of the most dramatic mass-casualty events in human history — from industrial disasters (Bhopal, 1984) to military use of war gases. In routine forensic practice, carbon monoxide is by far the most common fatal gas encountered (industrial, domestic, automotive); cyanide appears in industrial fires, metal plating, and jewellery industry accidents. Understanding the distinct mechanisms and post-mortem appearances of each gas enables confident cause-of-death determination. This SDL also provides the pharmacological basis for their specific antidotes.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A family of four is found unconscious on a winter morning in their sealed apartment. A charcoal heater was running overnight. When the paramedics open the door, all four appear 'healthy-looking' — their skin and lips are an unusual bright cherry-red colour despite being unconscious. One week later, a jewellery workshop explosion kills two workers, and the investigating police officer notes that the deceased also have cherry-red skin — yet the mechanism of death is entirely different from the apartment family. Two different gases, the same post-mortem colour. How do you distinguish them at autopsy, and why does the distinction matter for the medicolegal report?
WHY THIS MATTERS
Toxic gases occupy a special place in forensic medicine because they kill without visible trauma, may produce characteristic post-mortem signs (cherry-red discolouration), and require prompt antidote administration in survivors — but only if you recognise the correct agent. Carbon monoxide is the leading cause of accidental poisoning death in developed countries and a significant cause in India. Cyanide appears in industrial fires (burning synthetic materials release HCN), metal plating and jewellery industries, and — critically for exam purposes — produces the same cherry-red post-mortem colour as CO. Methyl isocyanate will always have forensic historical significance as the Bhopal gas. War gases represent the intersection of toxicology with international humanitarian law. Mastering this module is essential for the post-mortem opinion, the MLR, and survival-focused emergency medicine.
RECALL
Recall from Year 1:
- Biochemistry: haemoglobin and oxygen binding — haem iron (Fe²⁺) in each of the four subunits binds one O₂; cooperative binding; the oxygen-haemoglobin dissociation curve. CO has 200–300× greater affinity for haemoglobin than O₂ → carboxyhaemoglobin (HbCO) formation.
- Biochemistry: the mitochondrial electron transport chain (ETC) — Complex I through IV; Complex IV (cytochrome c oxidase) is the terminal electron acceptor that reduces O₂ to H₂O. Both CO and cyanide inhibit Complex IV.
- Biochemistry: the methaemoglobin trick in cyanide antidote — Fe²⁺ in normal haemoglobin can be oxidised to Fe³⁺ (methaemoglobin) by nitrites; cyanide preferentially binds Fe³⁺ in methaemoglobin over Fe³⁺ in cytochrome oxidase — this is the mechanism of the nitrite antidote.
- Physiology: asphyxia spectrum — inadequate O₂ delivery to tissues (anoxia) vs inability to use O₂ despite adequate delivery (histotoxic anoxia — cyanide, CO at cytochrome level).
Medicolegal Context: Toxic Gases in Indian and Global Forensic Practice
The forensic medicine encounter with toxic gas poisoning spans civilian accidents, industrial disasters, occupational exposure, homicide, suicide, and — at the extreme end — use of chemical agents in warfare or terrorism. In India, the most important categories are:
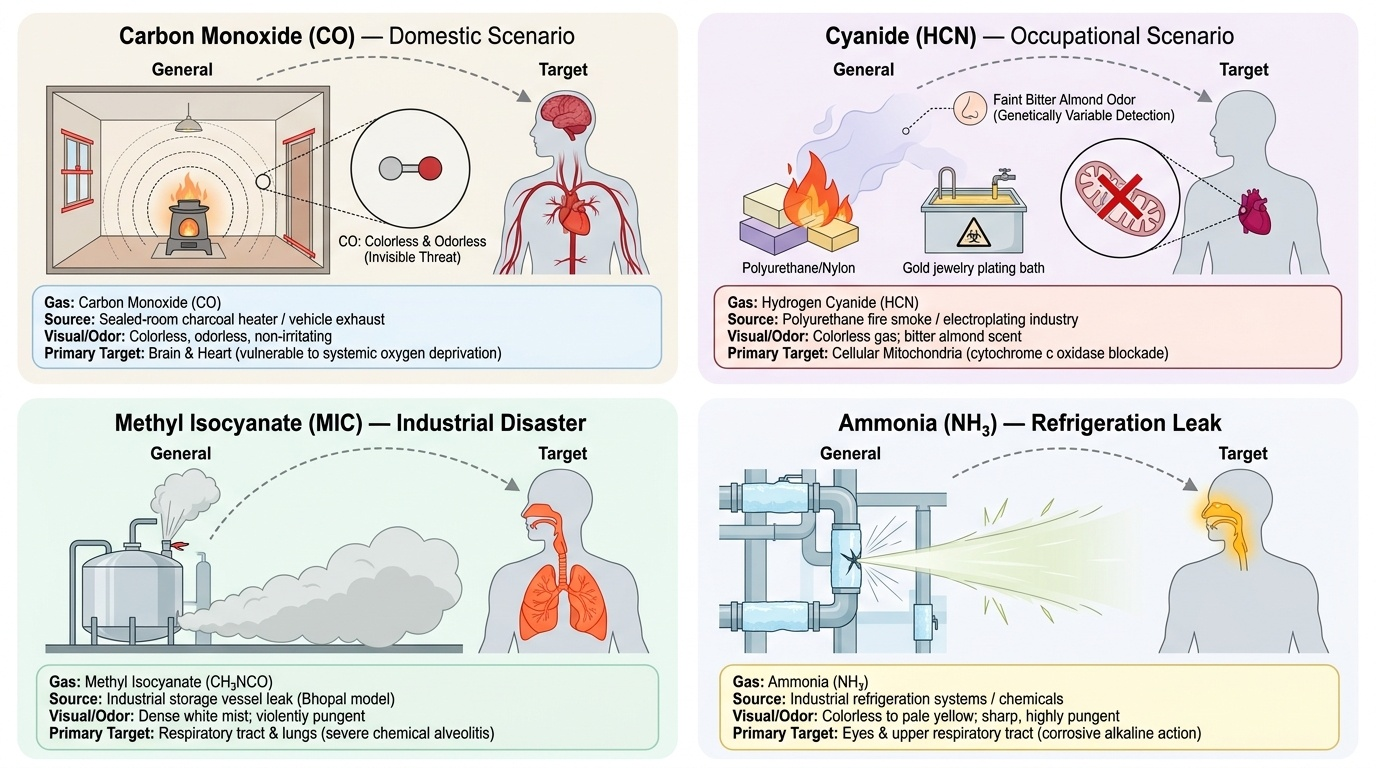
Carbon monoxide (CO) — the silent killer: CO is produced by incomplete combustion of any carbon-containing fuel (charcoal, wood, petrol, gas, kerosene). Common sources: domestic charcoal heaters in winter (sealed rooms), running vehicle engines in enclosed garages, industrial furnaces. Deaths are predominantly accidental, occasionally suicidal (deliberate exposure in a sealed space), and rarely homicidal. Because CO is colourless and odourless, victims have no warning. The medicolegal challenge is distinguishing CO death from other causes of sudden unconsciousness (cardiac arrest, epilepsy) when no witness is available.
Cyanide — industrial and fire hazard: Hydrogen cyanide (HCN) is used in metal plating, gold extraction (gold jewellery industry, relevant in India), and chemical synthesis. HCN is released when synthetic materials (polyurethane foam, wool, silk, nylon) burn — a significant occupational and building-fire hazard. Suicidal cyanide poisoning occurs among industrial chemists and mine workers with access. The forensic importance: bitter almond smell (specific but not always detectable — the ability to detect HCN odour is genetically variable) and cherry-red PM findings.
Methyl isocyanate (MIC) — the Bhopal legacy: The Bhopal gas tragedy (2–3 December 1984) — accidental release of 40 tonnes of MIC from Union Carbide India plant — killed an estimated 2,000–15,000 people (estimates vary) and injured 500,000. It remains the world's worst industrial disaster. Forensic significance: established the legal framework for corporate liability in industrial disasters; MIC is a highly reactive chemical asphyxiant/irritant with no antidote.
War gases and riot-control agents: Under the Chemical Weapons Convention (CWC) 1993, chemical warfare agents are prohibited in armed conflict. Tear gases (CS, CN) are classified as riot-control agents (legal under CWC for domestic law enforcement); India is a signatory. The forensic doctor may encounter casualties from their use in civil unrest.
Ammonia — industrial refrigerant, fertiliser production, cleaning agents; an upper respiratory tract/lung irritant with direct chemical burn mechanism; corrosive at high concentrations.
Provided image
Carbon Monoxide: Mechanism, Features and Post-Mortem Signs
Carbon monoxide (CO) is the most important toxic gas in routine forensic practice. Understanding its dual mechanism of toxicity is essential for both clinical management and post-mortem interpretation.
Mechanism of toxicity — two distinct components:
1. Carboxyhaemoglobin (HbCO) formation:
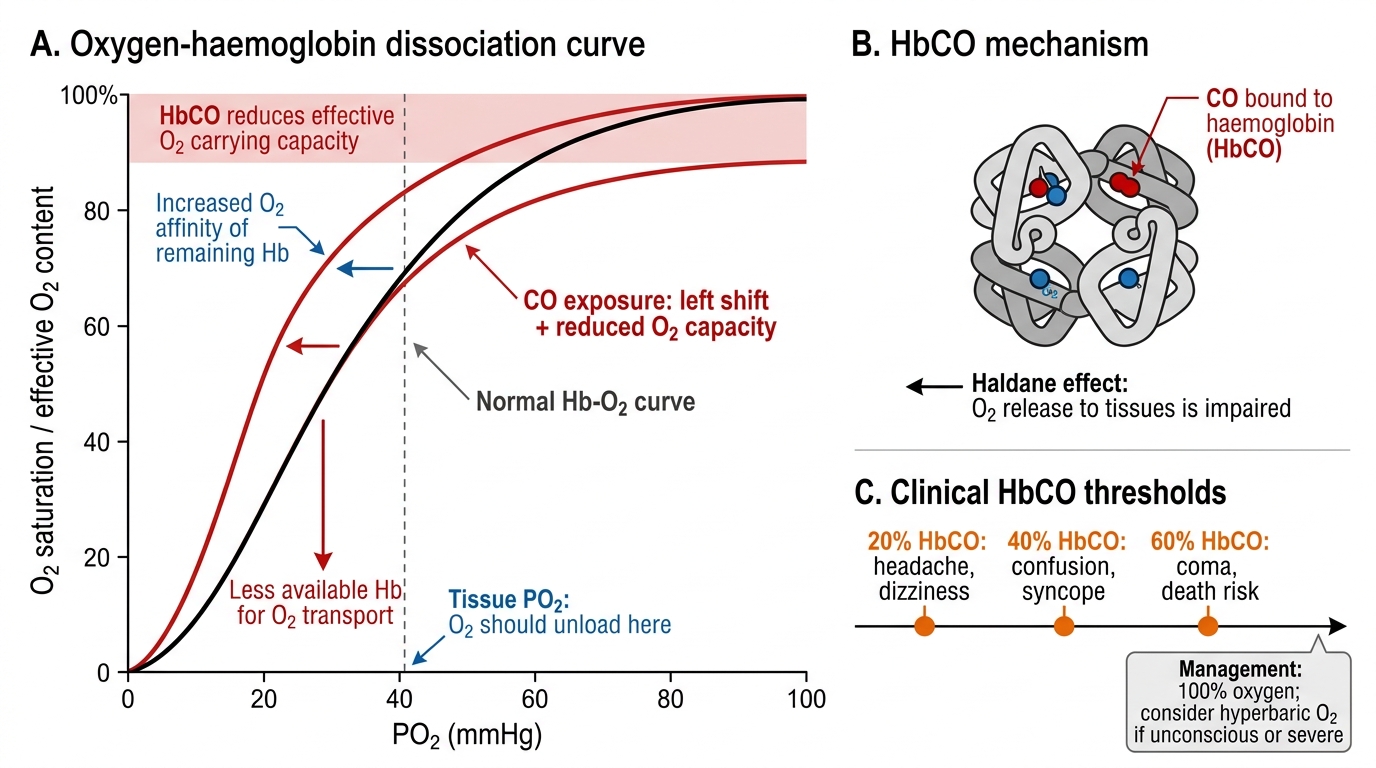
CO binds to the haem iron (Fe²⁺) of haemoglobin with an affinity 200–300 times greater than O₂. The resulting carboxyhaemoglobin (HbCO) cannot carry O₂ — it causes a functional anaemia ('histotoxic hypoxia'). Additionally, CO binding to one subunit of haemoglobin increases the affinity of the remaining subunits for O₂ (Haldane effect/left shift of the oxygen dissociation curve), meaning the O₂ that IS carried is not released to tissues — compounding the hypoxia.
2. Cytochrome c oxidase inhibition:
At high CO concentrations, CO also binds to the iron in cytochrome c oxidase (Complex IV, mitochondrial ETC), further impairing cellular O₂ utilisation independent of HbCO levels. This explains why the clinical severity of CO poisoning is not fully predicted by HbCO level alone.
Clinical features — correlation with HbCO levels:
- HbCO 10–20%: headache, dizziness, nausea
- HbCO 20–40%: confusion, visual disturbance, tachycardia
- HbCO 40–50%: confusion, hallucinations, syncope
- HbCO >50–60%: coma, seizures, cardiovascular collapse, death
The 'cherry-red' phenomenon:
HbCO is bright cherry-red — unlike the dark-brown-red of deoxyhaemoglobin. This produces the characteristic bright cherry-red skin, mucous membranes, and blood in CO poisoning. The cherry-red colour is most striking at post-mortem in cold weather (cold slows HbCO dissociation). At PM:
- Cherry-red lividity (hypostasis — the post-mortem staining)
- Cherry-red blood (liquid, non-clotting in early PM)
- Cherry-red viscera (liver, lung, muscle)
Antidote: 100% oxygen (high-flow).
Normobaric O₂ at 100% shortens HbCO half-life from ~5 hours (on room air) to ~60–90 minutes. Hyperbaric oxygen (HBO) at 2.5 atm shortens HbCO half-life to ~20 minutes and additionally reverses cytochrome oxidase binding. HBO is indicated for: HbCO >25%, loss of consciousness, neurological symptoms, pregnancy, or cardiac arrhythmia.
Carbon Monoxide Poisoning: HbCO and the Oxygen-Haemoglobin Curve
SELF-CHECK
A patient is rescued from a car fire and found unconscious. On examination, her skin is cherry-red. HbCO is 55%. Which of the following is the MOST appropriate treatment?
A. Sodium nitrite 300 mg IV followed by sodium thiosulphate 12.5 g IV
B. 100% oxygen via tight-fitting non-rebreather mask; consider hyperbaric oxygen
C. IV hydroxocobalamin 5 g IV
D. Activated charcoal 50 g orally
Reveal Answer
Answer: B. 100% oxygen via tight-fitting non-rebreather mask; consider hyperbaric oxygen
CO poisoning — HbCO 55%, unconscious. The antidote for CO is 100% oxygen (displaces CO from haemoglobin and cytochrome oxidase). Hyperbaric oxygen (HBO) is specifically indicated here: loss of consciousness qualifies as a criterion for HBO. Sodium nitrite + thiosulphate and hydroxocobalamin are the antidotes for CYANIDE poisoning. Activated charcoal has no role in gas inhalation poisoning.
Cyanide, MIC, Ammonia and War Gases
HYDROGEN CYANIDE (HCN) and CYANIDE SALTS:
Cyanide is among the most rapidly lethal substances known. In industry, it appears as hydrogen cyanide gas (prussic acid), potassium cyanide (KCN), and sodium cyanide (NaCN). HCN is also produced in fires involving burning synthetic materials.
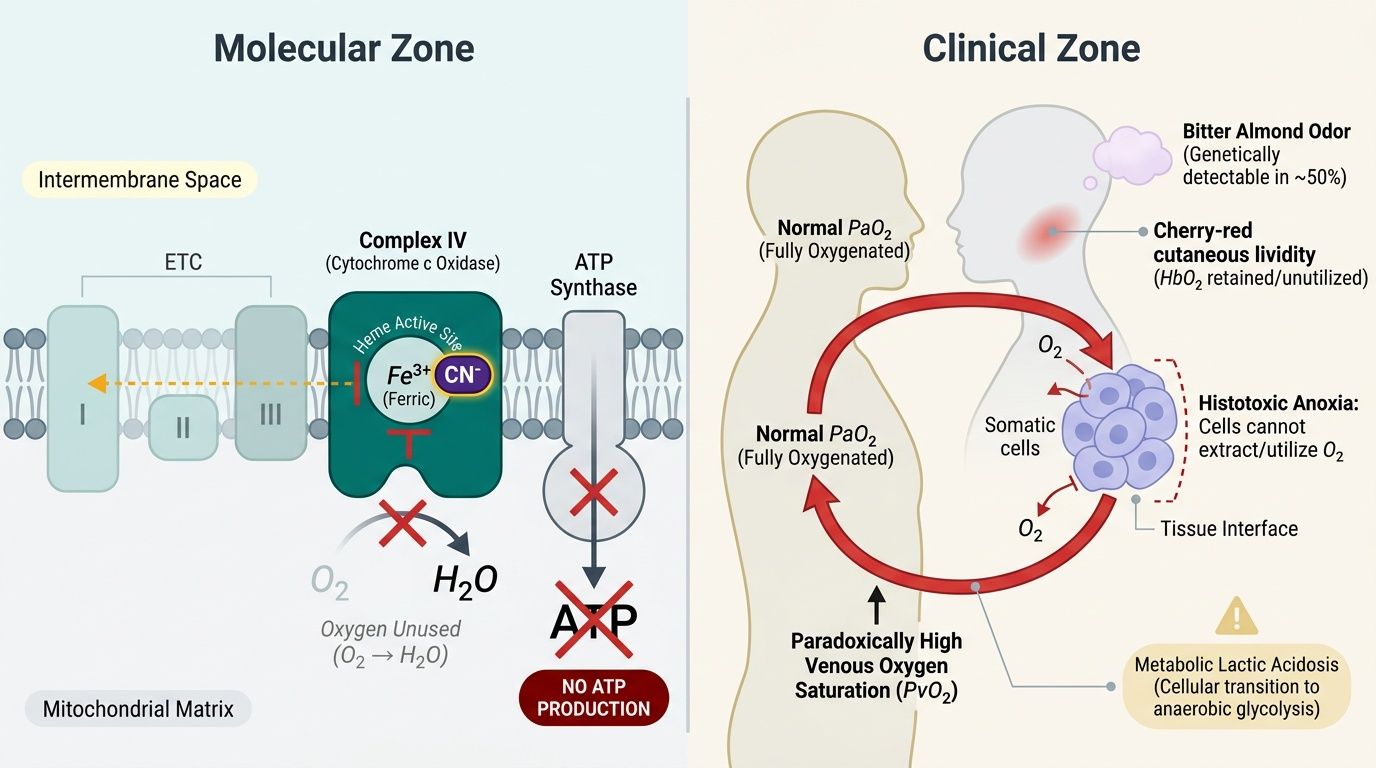
Mechanism: CN⁻ binds to the Fe³⁺ (ferric) form of cytochrome c oxidase (Complex IV), inhibiting electron transport chain → no ATP production → histotoxic anoxia — cells cannot utilise O₂ even when it is available in abundance (hence venous O₂ saturation is PARADOXICALLY HIGH in cyanide poisoning — tissues cannot extract O₂).
Clinical features:
- Bitter almond smell on the breath (specific but only ~50% of people can detect HCN by smell — genetically variable, so absence of the smell does NOT exclude HCN)
- Rapid loss of consciousness, convulsions, metabolic acidosis (lactic acidosis — cells default to anaerobic metabolism)
- Venous PO₂ is paradoxically high (tissue O₂ extraction is blocked)
Post-mortem findings (cyanide):
- Cherry-red lividity and viscera — SAME colour as CO; caused by the same principle: blood and tissues are well-oxygenated (HbO₂ retained because cells cannot extract O₂)
- Bitter almond smell of viscera and body cavities — reliable PM finding if detectable
- The key PM distinction from CO: history (industrial/fire context for CN; enclosed combustion source for CO), blood HbCO level (absent in CN), and analytical toxicology (blood/liver cyanide level)
Antidotes for cyanide — three-step protocol:
Step 1 — Inhaled amyl nitrite (first aid): Causes methaemoglobin formation (Fe²⁺ → Fe³⁺); CN⁻ preferentially binds Fe³⁺ in methaemoglobin rather than cytochrome oxidase.
Step 2 — IV sodium nitrite (3%) 300 mg: Generates more methaemoglobin, converting more HbFe²⁺ to HbFe³⁺ (metHb) that acts as a CN⁻ 'sponge'.
Step 3 — IV sodium thiosulphate (25%) 12.5 g: Provides a sulfur donor for rhodanese enzyme (thiosulphate + CN⁻ → thiocyanate + sulphite), which converts toxic cyanide to non-toxic thiocyanate excreted in urine.
Alternative: IV hydroxocobalamin (5 g) — binds directly to CN⁻ (cobalt in hydroxocobalamin forms cobaltocyanide, which is renally excreted); now preferred in many countries as it does not cause methaemoglobinaemia (unlike nitrites); indicated when CO + HCN co-exposure is suspected (fire victims) because nitrites in a CO-poisoned patient worsen O₂ delivery.
METHYL ISOCYANATE (MIC) — Bhopal context:
MIC (CH₃NCO) is an extremely reactive, highly volatile chemical intermediate used in carbamate pesticide synthesis. Mechanism: MIC reacts with and alkylates biological molecules (proteins, DNA), causing direct cellular damage in the respiratory epithelium. Direct toxic effects: severe bronchospasm, pulmonary oedema, ARDS, chemical burns to eyes (blindness), skin sensitisation.
No specific antidote. Bhopal victims received supportive respiratory care. Long-term sequelae include chronic obstructive pulmonary disease, neurological damage (ophthalmic damage, peripheral neuropathy), and reproductive effects. The Bhopal disaster established legal precedent for corporate environmental and tort liability in India.
AMMONIA (NH₃):
Highly water-soluble → primarily upper airway/mucous membrane corrosive effect (laryngeal oedema, bronchospasm). High-concentration inhalation causes chemical pneumonitis/pulmonary oedema. Characteristic pungent smell. No systemic antidote — supportive respiratory care; decontaminate with water.
TEAR GASES / RIOT CONTROL AGENTS:
- CS gas (2-chlorobenzalmalononitrile): the most widely used; mechanism involves alkylation of TRPA1 pain receptors on sensory nerves → lacrimation, burning pain in eyes/skin/upper airways, coughing, temporary visual incapacitation. Effects are reversible on exposure cessation.
- CN gas (chloroacetophenone): older agent; more toxic than CS; similar mechanism.
- MACE, pepper spray (OC — oleoresin capsicum): capsaicin-based TRPV1 agonist; similar immediate effects.
- Forensic significance: rare deaths from riot-control agents have been reported at high concentrations in enclosed spaces; these would be investigated as potential criminal misuse.
Provided image
SELF-CHECK
Two victims are found dead in a jewellery factory fire. Post-mortem examination of both shows cherry-red lividity and viscera. One victim has HbCO of 48%; the other has normal HbCO but extremely high venous PO₂ on post-mortem blood gas. Which of the following correctly explains the venous PO₂ finding in victim 2?
A. Victim 2 died of CO poisoning but the HbCO test was a false negative
B. Victim 2 died of cyanide poisoning — cells could not extract O₂ from blood, leaving venous blood well-oxygenated
C. Victim 2 died of methanol poisoning — methanol causes histotoxic anoxia and high venous O₂
D. Victim 2 has normal findings — cherry-red lividity with high venous PO₂ is a normal post-mortem artefact
Reveal Answer
Answer: B. Victim 2 died of cyanide poisoning — cells could not extract O₂ from blood, leaving venous blood well-oxygenated
Cyanide poisoning causes histotoxic anoxia — CN⁻ blocks cytochrome c oxidase so cells cannot extract O₂ from blood. Consequently venous blood retains its oxygenation (high venous PO₂), and tissues remain red/cherry-red as HbO₂ is not extracted. This paradoxical high venous O₂ in a dead patient is pathognomonic of a histotoxic mechanism (CN or CO at cytochrome level). CO poisoning (victim 1) produces HbCO, which is also cherry-red but is explained by HbCO formation, not tissue O₂ extraction failure. Methanol is not associated with cherry-red findings.