Page 15 of 33
FM13.16 | Toxic & War Gases — SDL Guide (Part 2)
Clinical Examination, Sampling and Post-Mortem Protocol
The clinical and forensic examination of a suspected toxic gas casualty requires rapid identification of the toxidrome and collection of time-sensitive specimens before the gas is metabolised or dissipated.
Provided image
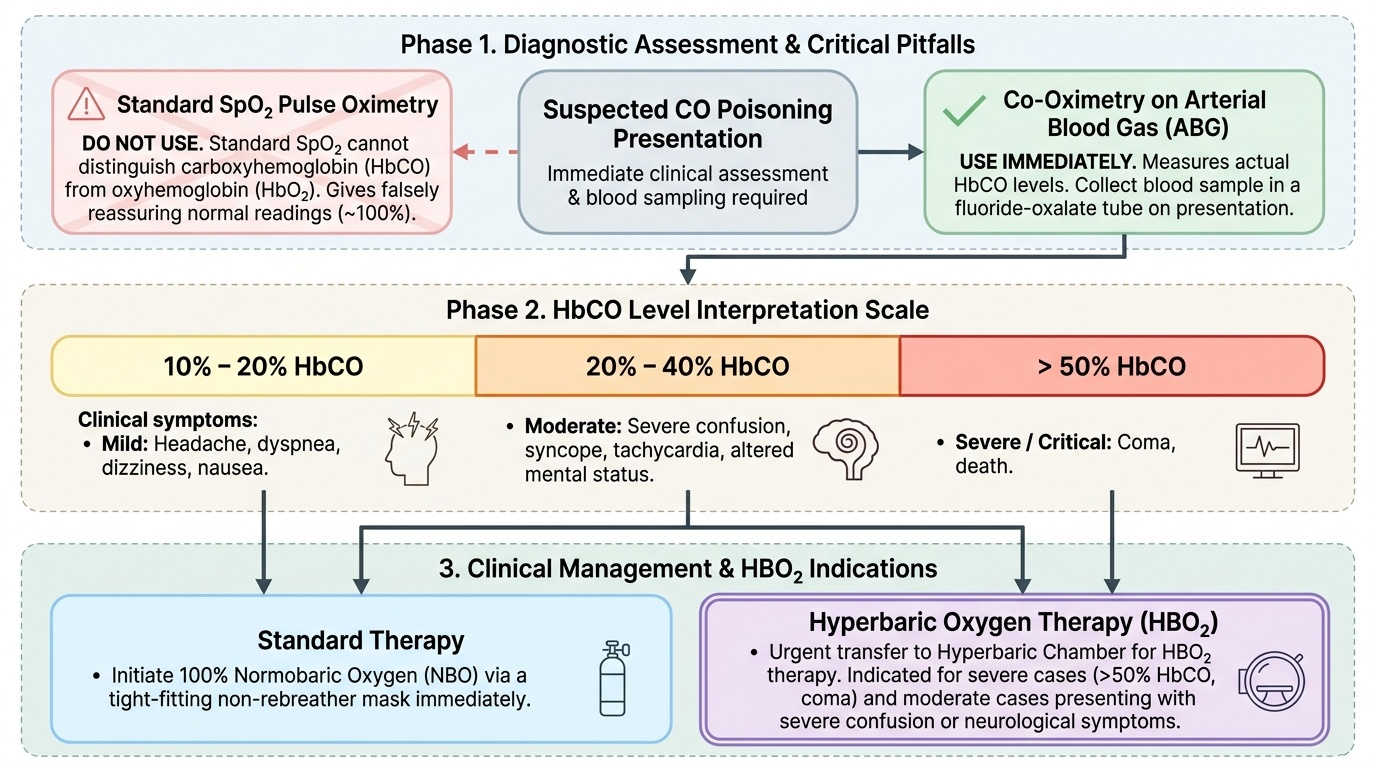
CO poisoning — examination and sampling:
- Assess HbCO immediately (co-oximeter on ABG machine — standard SpO₂ pulse oximetry CANNOT distinguish HbCO from HbO₂ and will give falsely reassuring readings)
- Document neurological status (GCS, delayed neurological syndrome develops 2–4 weeks after apparent recovery in 10–30% of patients)
- Collect blood in fluoride-oxalate tube immediately on presentation (HbCO level — the only definitive test)
- At PM: blood from femoral vein (sealed tube for HbCO spectrophotometry), vitreous humour (CO-resistant to post-mortem decomposition)
Cyanide poisoning — examination and sampling:
- Note bitter almond smell (if detectable)
- Blood for cyanide level (immediately, in sealed glass tube — CN⁻ is volatile)
- Note venous PO₂ on ABG (high venous O₂ tension is a pointer)
- At PM: blood (sealed), liver, gastric contents; chemical test — Prussian blue test (adds ferrous sulfate + ferric chloride to acidified tissue → blue colour if CN⁻ present)
Documentation of scene findings:
For CO: document the combustion source, ventilation of the room, number of victims, position of victims, and whether all were found together (pattern of simultaneous CO deaths in a sealed space). For industrial gas (cyanide, MIC, ammonia): document the industrial process, ventilation failure, safety equipment availability, and employer compliance with occupational safety standards.
Distinguishing CO from cyanide at PM:
| Feature | CO | Cyanide |
|---|---|---|
| PM colour | Cherry-red | Cherry-red |
| Smell | Odourless | Bitter almond |
| HbCO | Elevated (>50% fatal) | Normal |
| Venous PO₂ | Normal or low | HIGH |
| Source | Combustion | Industrial/fire/suicide |
| Analytical test | HbCO spectrophotometry | CN blood level; Prussian blue test |
Medicolegal Inference, Treatment Summary and Statutory Framework
The management of toxic gas poisoning is agent-specific, but the underlying principle is always the same — remove the source of exposure, provide supportive ventilation, and administer the specific antidote where one exists.
Treatment summary:
CO:
- Remove from exposure
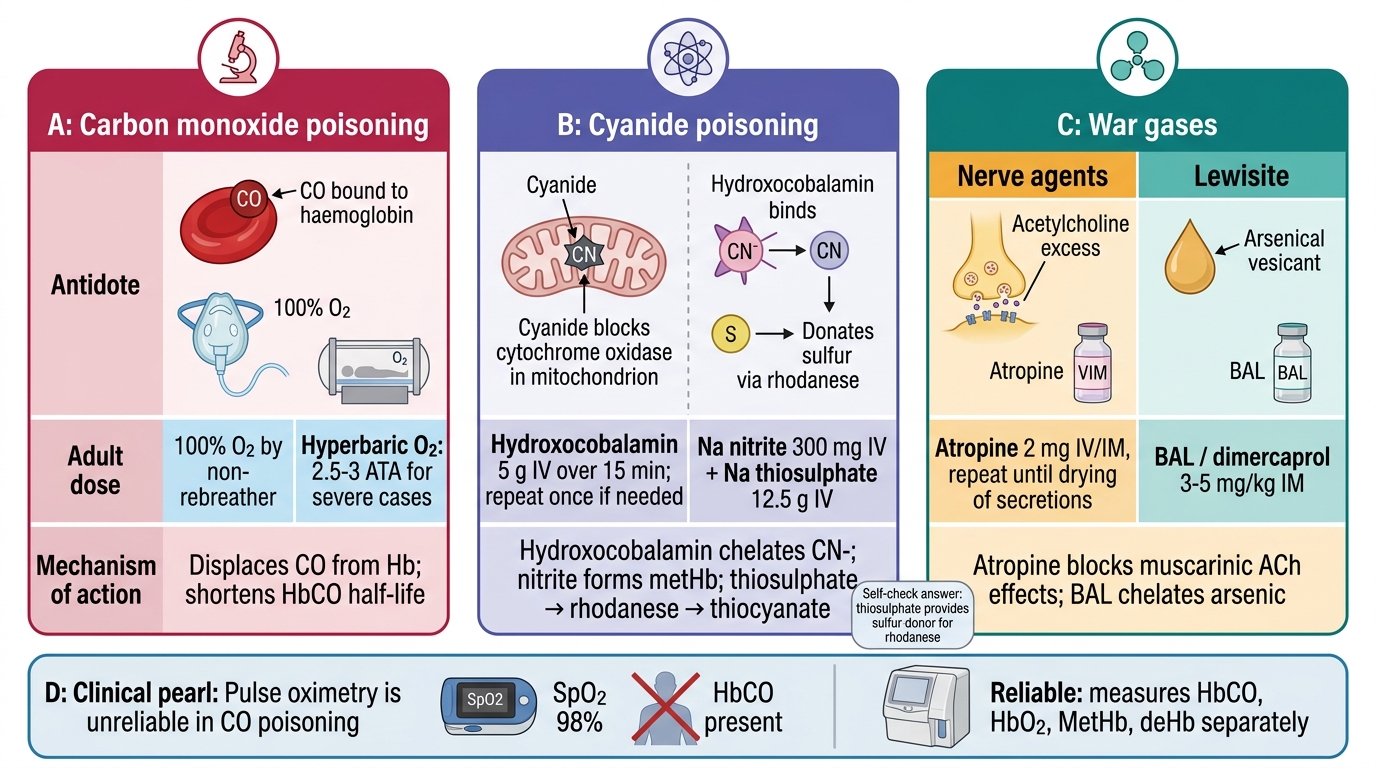
- 100% O₂ via tight-fitting non-rebreather mask (reduces HbCO half-life from 5 h to 60–90 min)
- Hyperbaric oxygen (2.5 atm) — indications: HbCO >25%, LOC, pregnancy, cardiac arrhythmia, neurological symptoms (reduces HbCO half-life to ~20 min and reverses cytochrome oxidase binding)
- Supportive: cardiac monitoring, benzodiazepines for seizures
Cyanide:
- Remove from exposure (decontaminate skin if liquid HCN exposure)
- Antidote sequence: amyl nitrite (inhaled) → sodium nitrite 300 mg IV → sodium thiosulphate 12.5 g IV
- OR hydroxocobalamin 5 g IV (preferred in fire victims with co-exposure to CO, as it avoids methaemoglobinaemia worsening CO toxicity)
- 100% O₂ (adjunct; does not displace CN from cytochrome oxidase but supports oxygenation)
MIC/ammonia/riot gases:
- Remove from exposure
- Eye irrigation (water, copious)
- Respiratory support; bronchodilators
- No specific antidote
Medicolegal and statutory framework:
CO deaths:
- Accidental domestic: no criminal liability unless negligence (e.g., landlord's failure to maintain boiler — IPC §304A or Consumer Protection Act)
- Suicidal: confirm intention evidence (sealed room, notes, history)
- Homicidal CO: documented (victim sealed in vehicle/room with running engine); IPC §302/302
Bhopal/MIC precedent:
- Bhopal Gas Leak Disaster (Processing of Claims) Act 1985
- Union Carbide India Limited (UCIL) criminal case — corporate liability for industrial negligence; established that corporations can be held criminally liable for industrial disasters
- Environment Protection Act 1986 (enacted partly in response to Bhopal)
Chemical Weapons Convention (CWC) 1993:
- India ratified CWC 1996
- Schedules 1–3 chemicals (Schedule 1 = most restricted, including nerve agents/mustard gas)
- CS/CN tear gases are 'riot control agents' — permitted under CWC for domestic law enforcement; not permitted as a weapon of war
Antidote Comparison for CO, Cyanide, and War Gas Poisoning
CLINICAL PEARL
Pulse oximetry is unreliable in CO poisoning. Standard pulse oximeters measure light absorbance at two wavelengths (660 nm and 940 nm) and interpret any red-absorbing species as oxyhaemoglobin. HbCO absorbs similarly to HbO₂ at these wavelengths, so the pulse oximeter reads HbCO as if it were HbO₂ — producing falsely normal SpO₂ readings. A patient dying of CO poisoning may have an SpO₂ reading of 98%. The only reliable test is co-oximetry (a multi-wavelength ABG analyser that directly measures HbCO, HbO₂, metHb, and deHb separately). This distinction is critical — a normal SpO₂ does NOT exclude CO poisoning.
SELF-CHECK
In cyanide poisoning, sodium thiosulphate is given as part of the antidote protocol. The mechanism by which sodium thiosulphate helps is:
A. It oxidises Fe²⁺ to Fe³⁺ in haemoglobin, creating methaemoglobin that binds cyanide
B. It provides a sulfur donor for the enzyme rhodanese, which converts CN⁻ to non-toxic thiocyanate
C. It directly chelates CN⁻ ions in a ring-structure complex that is renally excreted
D. It inhibits ADH to prevent cyanide's metabolism to more toxic products
Reveal Answer
Answer: B. It provides a sulfur donor for the enzyme rhodanese, which converts CN⁻ to non-toxic thiocyanate
Rhodanese (thiosulfate sulfurtransferase) is an endogenous detoxification enzyme that uses sulfur (from thiosulphate) to convert cyanide (CN⁻) to thiocyanate (SCN⁻), which is non-toxic and renally excreted. The reaction is: CN⁻ + S₂O₃²⁻ → SCN⁻ + SO₃²⁻. Step 1 (methaemoglobin formation) is accomplished by sodium NITRITE. Hydroxocobalamin directly chelates CN⁻ via its cobalt centre, not thiosulphate.