Page 8 of 25
IM1.15-18 | Heart Failure Investigations — SDL Guide
Learning Objectives
- Order and interpret a diagnostic work-up for heart failure including ECG, chest radiograph, BNP, and echocardiography
- Perform and interpret a standard 12-lead ECG in the context of cardiac disease
- Describe the indications and expected findings of echocardiography, BNP, exercise testing, nuclear medicine testing, and coronary angiography in heart failure
- Discuss the severity grading of valvular heart disease and the thresholds for surgical or interventional referral
INSTRUCTIONS
Accurate diagnosis and severity assessment of heart failure depend on a structured combination of clinical evaluation, biomarkers, and imaging. This module walks you through the investigation toolkit — from the bedside ECG to coronary angiography — teaching you not just what to order but how to interpret the results and integrate them into a management decision.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 252 — Heart Failure: Pathophysiology and Diagnosis (textbook)
- API Textbook of Medicine, 10th ed., Ch. 8 — Cardiac Failure: Investigation and Management (textbook)
- ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure, 2021 (guideline)
- ACC/AHA Guideline for the Management of Heart Failure, 2022 Update (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old man with known hypertension presents to casualty with a 3-day history of worsening breathlessness, bilateral ankle swelling, and orthopnoea requiring three pillows. On examination his JVP is elevated to 6 cm above the sternal angle, there is bilateral basal crackles, and peripheral oedema to the knees. The resident orders a chest X-ray, an ECG, blood tests including BNP, and arranges an echocardiogram. The ECG shows sinus rhythm with left bundle branch block (LBBB). The CXR reveals cardiomegaly with upper lobe venous diversion and bilateral Kerley B lines. The BNP returns at 820 pg/mL. The echocardiogram the next morning reports an ejection fraction of 32%, dilated left ventricle, and moderate mitral regurgitation. Now the picture is complete — not just 'heart failure' but HFrEF (HF with reduced EF, LVEF ≤40%), caused by hypertensive cardiomyopathy with secondary mitral regurgitation, with LBBB indicating ventricular dyssynchrony that may itself be amenable to device therapy. Each investigation answered a different question. This module teaches you which test answers which question, and what the answers mean.
WHY THIS MATTERS
Investigations in heart failure serve four distinct purposes: confirming the diagnosis (excluding other causes of breathlessness), classifying the type of failure (HFrEF vs HFmrEF vs HFpEF, systolic vs diastolic), identifying the aetiology (ischaemic, valvular, hypertensive, cardiomyopathic), and guiding specific therapy (device therapy for LBBB + reduced EF, surgery for severe valvular disease, revascularisation for ischaemic cardiomyopathy). At the NMC SH/KH level, you must be able to order the right tests, interpret the results at the bedside, and translate those findings into a management decision. In Indian tertiary hospitals, the 12-lead ECG, CXR, and echocardiogram together provide the majority of the diagnostic and classification information needed to initiate evidence-based therapy, even when more sophisticated tests are unavailable.
RECALL
Before proceeding, recall that heart failure is classified by ejection fraction: HFrEF (LVEF ≤40%), HFmrEF (LVEF 41–49%), and HFpEF (LVEF ≥50%). Recall also that the left ventricle receives oxygenated blood from the pulmonary veins and ejects it into the aorta — left heart failure causes pulmonary congestion (dyspnoea, orthopnoea, PND, crackles). The right ventricle receives deoxygenated blood from the systemic veins and ejects it into the pulmonary artery — right heart failure causes systemic venous congestion (elevated JVP, peripheral oedema, hepatomegaly). The ECG reflects electrical activity; the echocardiogram reflects mechanical function. Review the surface ECG lead anatomy: limb leads I, II, III, aVR, aVL, aVF; precordial leads V1–V6. This prior knowledge anchors the interpretation sections that follow.
Clinical Indication: When and Why to Investigate
The decision to investigate for heart failure is triggered by a constellation of clinical findings — no single symptom or sign is pathognomonic — making a structured investigation sequence essential. The clinician must simultaneously confirm the diagnosis, establish the aetiology, classify the severity, and identify reversible or treatable precipitants. Each investigation has a specific place in this sequence, and requesting them in the correct order avoids redundant tests and delays.
Provided image
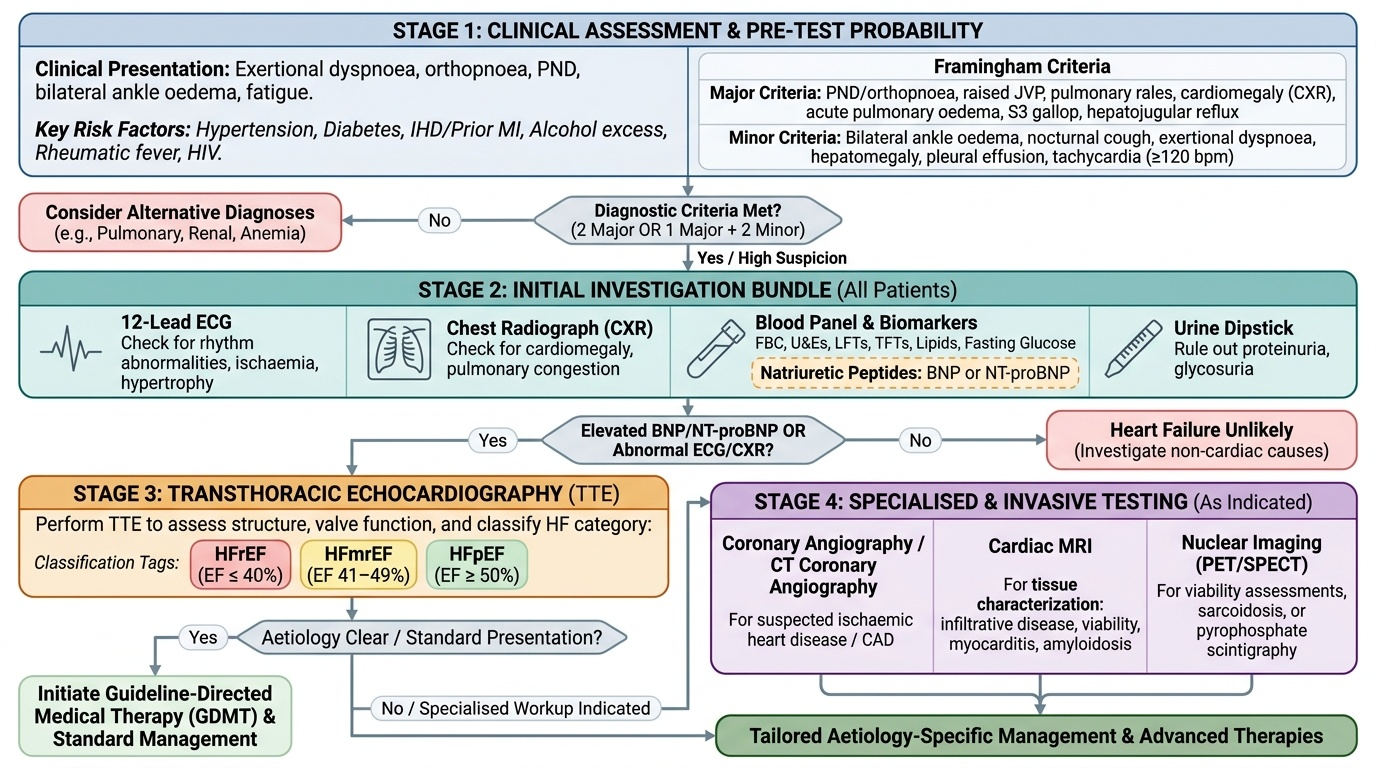
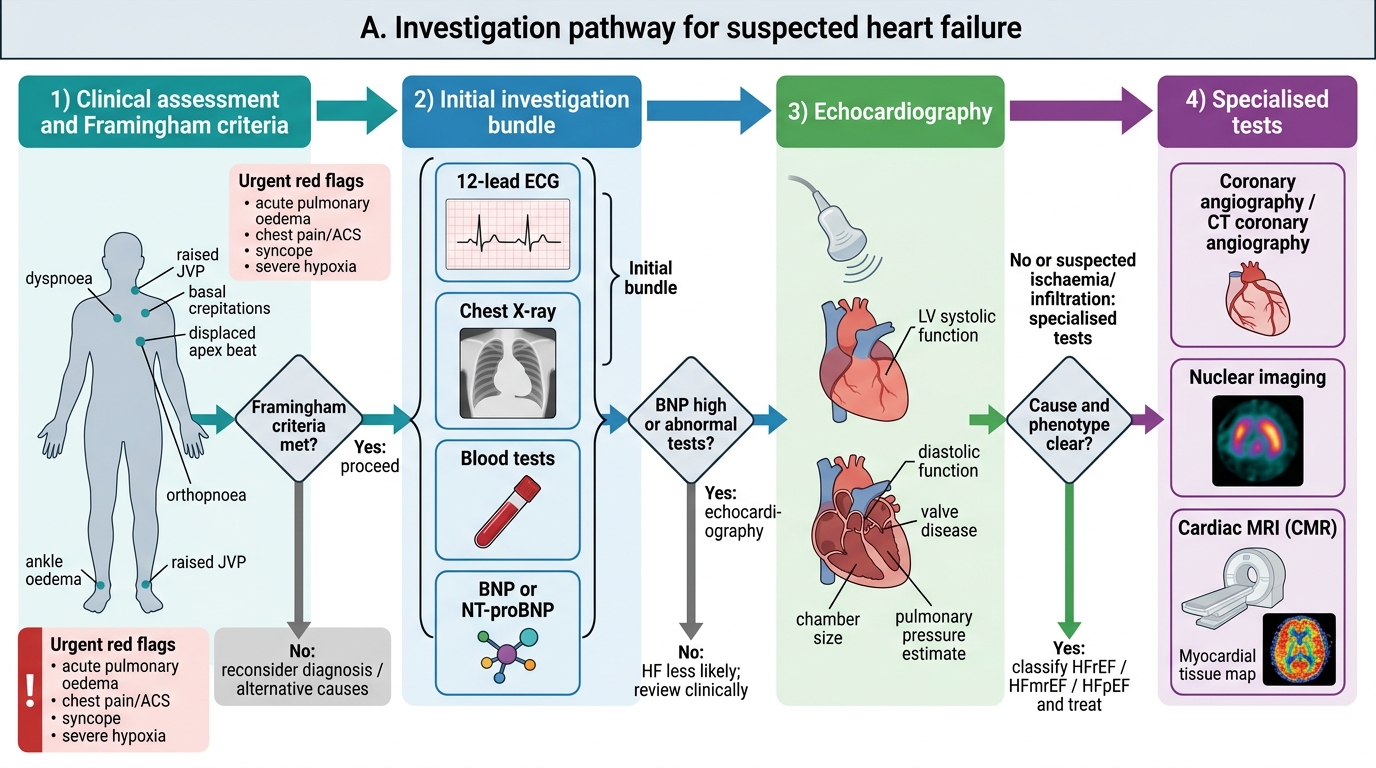
Clinical indications for investigation broadly encompass any patient presenting with exertional dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea, bilateral ankle oedema, fatigue, or reduced exercise tolerance — especially in the context of known risk factors (hypertension, diabetes, ischaemic heart disease, prior myocardial infarction, alcohol use, rheumatic fever, HIV). In acute presentations to emergency or inpatient settings, the investigation is guided by the need to confirm diagnosis rapidly and to exclude life-threatening alternatives (acute pulmonary oedema vs massive pulmonary embolism vs pneumonia). In chronic outpatient settings, the emphasis shifts to quantification of severity and tracking of progression.
The Framingham criteria remain clinically useful as a diagnostic framework: major criteria include PND or orthopnoea, raised JVP, pulmonary rales, cardiomegaly on CXR, acute pulmonary oedema, S3 gallop, and hepatojugular reflux; minor criteria include bilateral ankle oedema, nocturnal cough, dyspnoea on exertion, hepatomegaly, pleural effusion, and tachycardia >120 bpm. The diagnosis requires 2 major or 1 major + 2 minor criteria. This clinical pre-test probability assessment determines the urgency and depth of investigation.
The initial investigation bundle in all new or decompensated heart failure should always include: (1) a 12-lead ECG, (2) a chest radiograph, (3) blood tests — full blood count, renal function, electrolytes, liver function, thyroid function (TFTs), fasting glucose, lipid profile, and B-type natriuretic peptide (BNP) or NT-proBNP, and (4) urine dipstick. Echocardiography follows to classify the type of failure and define the aetiology. More invasive or specialised tests — coronary angiography, nuclear imaging, cardiac MRI — are ordered only when indicated by the findings of this initial bundle.
Investigation Algorithm for Suspected Heart Failure
The 12-Lead ECG: Principles and Interpretation in Heart Failure
The 12-lead electrocardiogram (ECG) is the single most informative and immediately available investigation in heart failure. It is not sensitive enough to diagnose heart failure directly, but it rarely shows a completely normal pattern in established heart failure, and its findings direct the next steps in the investigation cascade. A normal ECG in a patient with suspected heart failure should prompt reconsideration of the diagnosis.
Provided image
The governing principle of ECG interpretation is that the 12 leads record the same electrical event from 12 different spatial angles, providing three-dimensional information about depolarisation and repolarisation across the myocardium. The limb leads (I, II, III, aVR, aVL, aVF) record the frontal plane; the precordial leads (V1–V6) record the horizontal plane, with V1–V2 overlying the right ventricle and septum, V3–V4 the anterior wall, and V5–V6 the lateral left ventricle. The electrical axis (predominantly leftward in normal adults, −30° to +90°) shifts with ventricular hypertrophy and conduction abnormalities.
Key ECG abnormalities and their significance in heart failure:
Left ventricular hypertrophy (LVH): Caused by chronic pressure overload (hypertension, aortic stenosis). Sokolow-Lyon voltage criteria: S in V1 + R in V5 or V6 >35 mm (in adults >35 years). Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women). LVH voltage criteria have high specificity but limited sensitivity; the ECG pattern of LVH with strain (ST depression and T-wave inversion in lateral leads V5–V6, I, aVL) indicates established pressure overload.
Atrial fibrillation (AF): Recognised by absent P waves, irregular baseline (fibrillation waves at 350–600 per minute), and irregularly irregular ventricular response. AF is both a cause and consequence of heart failure; it accelerates ventricular dyssynchrony and reduces diastolic filling time, worsening haemodynamics. The CHA₂DS₂-VASc score must be calculated in all AF + HF patients to guide anticoagulation: Congestive HF, Hypertension, Age ≥75 (2 points), Diabetes, Stroke/TIA (2 points), Vascular disease, Age 65–74, Sex category female — score ≥2 in men or ≥3 in women warrants anticoagulation.
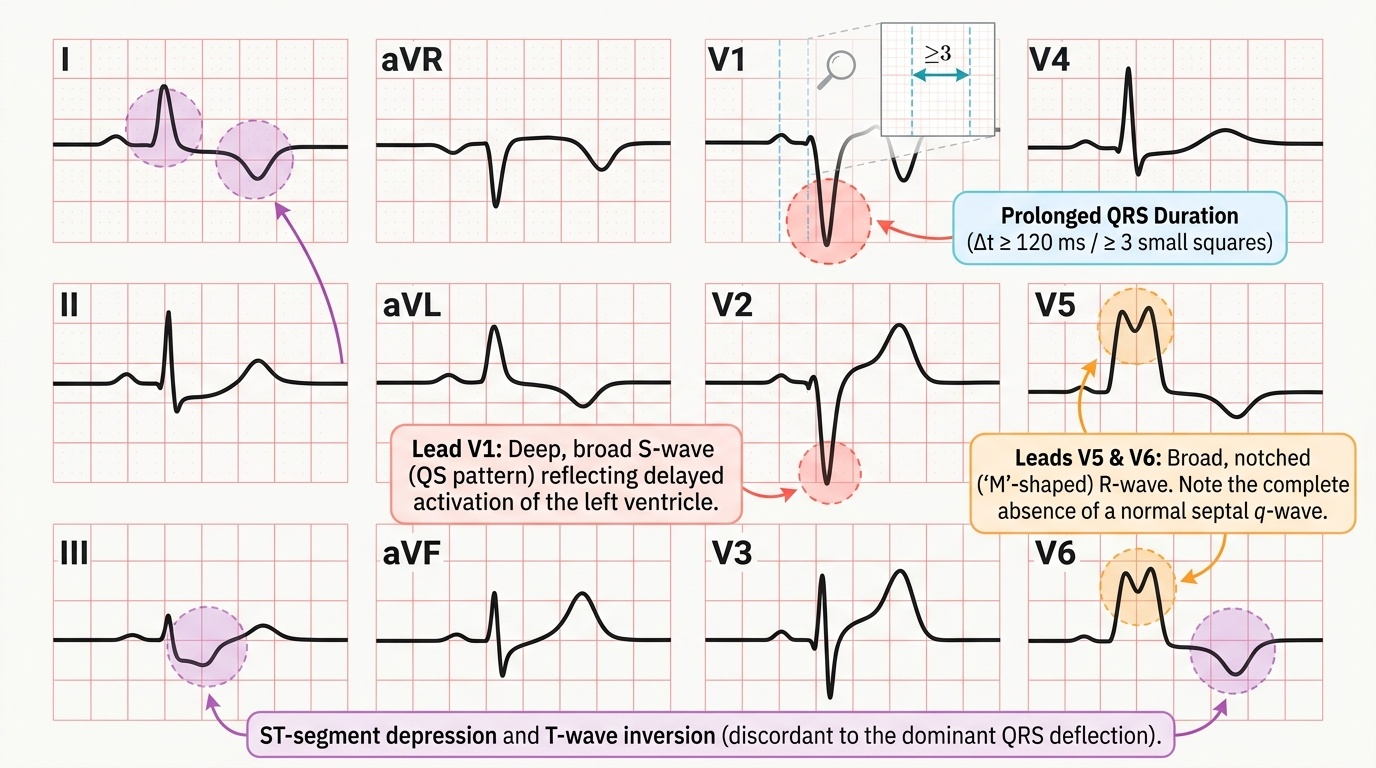
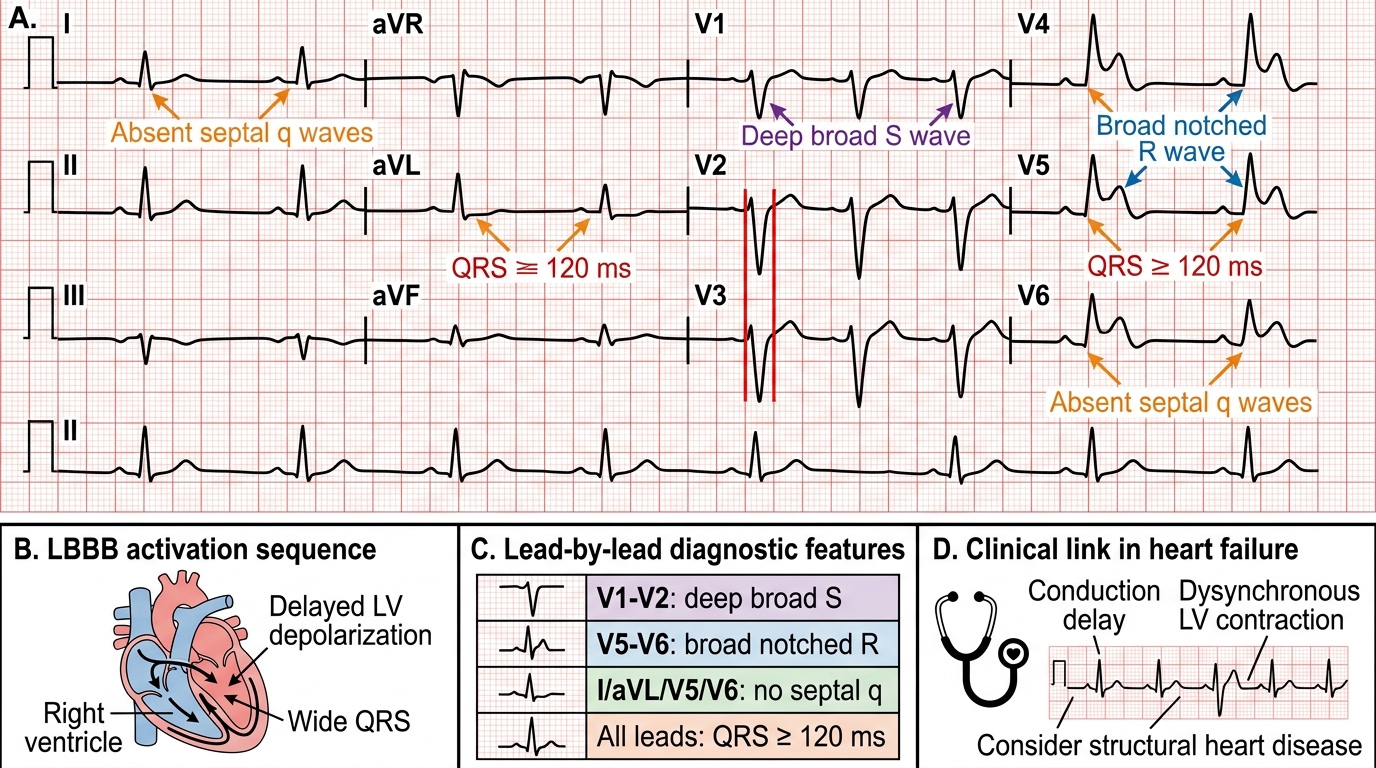
Left bundle branch block (LBBB): QRS duration ≥120 ms; broad, notched R waves in lateral leads (I, V5–V6); broad, deep S waves in V1; absence of septal Q waves in I, V5–V6. LBBB in the context of reduced LVEF indicates ventricular dyssynchrony and is the key indication for cardiac resynchronisation therapy (CRT) — specifically LBBB + LVEF ≤35% + QRS ≥150 ms on optimal medical therapy.
Previous myocardial infarction: Pathological Q waves (width ≥40 ms, depth ≥25% of R wave height) in corresponding leads indicate prior transmural infarction and suggest ischaemic aetiology for heart failure.
Right ventricular strain / cor pulmonale: Right axis deviation, tall R in V1, right bundle branch block (RBBB) pattern (rsR' in V1, broad terminal S in I and V6), P pulmonale (peaked P in II ≥2.5 mm).
Left Bundle Branch Block on 12-Lead ECG
Chest Radiograph and Biomarkers: BNP and NT-proBNP
The chest radiograph (CXR) in heart failure provides rapid, bedside-accessible information about cardiac size, pulmonary vasculature, and the degree of congestion. It is especially valuable in acute presentations and serial monitoring of decompensation and treatment response.
Cardiac findings on CXR: the cardiothoracic ratio (CTR) is measured as the widest diameter of the cardiac silhouette divided by the widest internal thoracic diameter on a PA film; a CTR >0.5 is cardiomegaly. Specific chamber enlargement can be inferred — a large left ventricle produces a leftward and downward displacement of the cardiac apex; left atrial enlargement produces straightening of the left heart border, double-shadow behind the right heart border, and elevation of the left main bronchus (the left atrial angle >70°). Right heart enlargement produces a rightward shift of the right heart border.
Pulmonary vascular findings reflect the haemodynamic severity of left heart failure:
- Upper lobe venous diversion (cephalisation): Normally, pulmonary veins in the lower zones are larger than upper zones (effect of gravity). In early left heart failure, elevated PCWP (pulmonary capillary wedge pressure) causes equalisation and then reversal — upper lobe vessels become larger. This is a sign of mild to moderate pulmonary venous hypertension (PCWP typically 12–18 mmHg).
- Kerley B lines: Horizontal, dense, short (1–2 cm) lines at the periphery of the lower lung zones, representing fluid in interlobular septa. Indicate interstitial oedema with PCWP approximately 18–25 mmHg.
- Bat-wing (butterfly) perihilar shadowing: Bilateral, symmetric, perihilar airspace opacity in acute pulmonary oedema; PCWP typically >25 mmHg.
- Pleural effusion: Blunting of costophrenic angles (more commonly right-sided or bilateral in HF).
B-type natriuretic peptide (BNP) and NT-proBNP are the primary biomarkers for heart failure diagnosis and severity assessment. BNP is a 32-amino-acid peptide released by ventricular cardiomyocytes in response to increased wall stress (i.e., increased preload and afterload — the haemodynamic hallmark of failing myocardium). The N-terminal cleavage product, NT-proBNP, is biologically inactive but measurable; it has a longer half-life and is the preferred marker in many laboratories.
Interpretation thresholds:
- BNP <35 pg/mL (or NT-proBNP <125 pg/mL in chronic HF): makes heart failure unlikely as the cause of dyspnoea — high negative predictive value.
- BNP >100 pg/mL (or NT-proBNP >300 pg/mL for any age; or age-stratified: >450 pg/mL for <50 yr, >900 for 50–75 yr, >1800 for >75 yr): consistent with heart failure; higher values correlate with worse functional class and prognosis.
- Values between these thresholds constitute a grey zone requiring clinical correlation and echocardiography.
Important limitations: BNP/NT-proBNP can be elevated in renal failure, AF, pulmonary embolism, sepsis, and advanced age (causes of false positives), and may be disproportionately lower in obesity and flash pulmonary oedema (causes of false negatives in HFpEF). They must always be interpreted in clinical context.
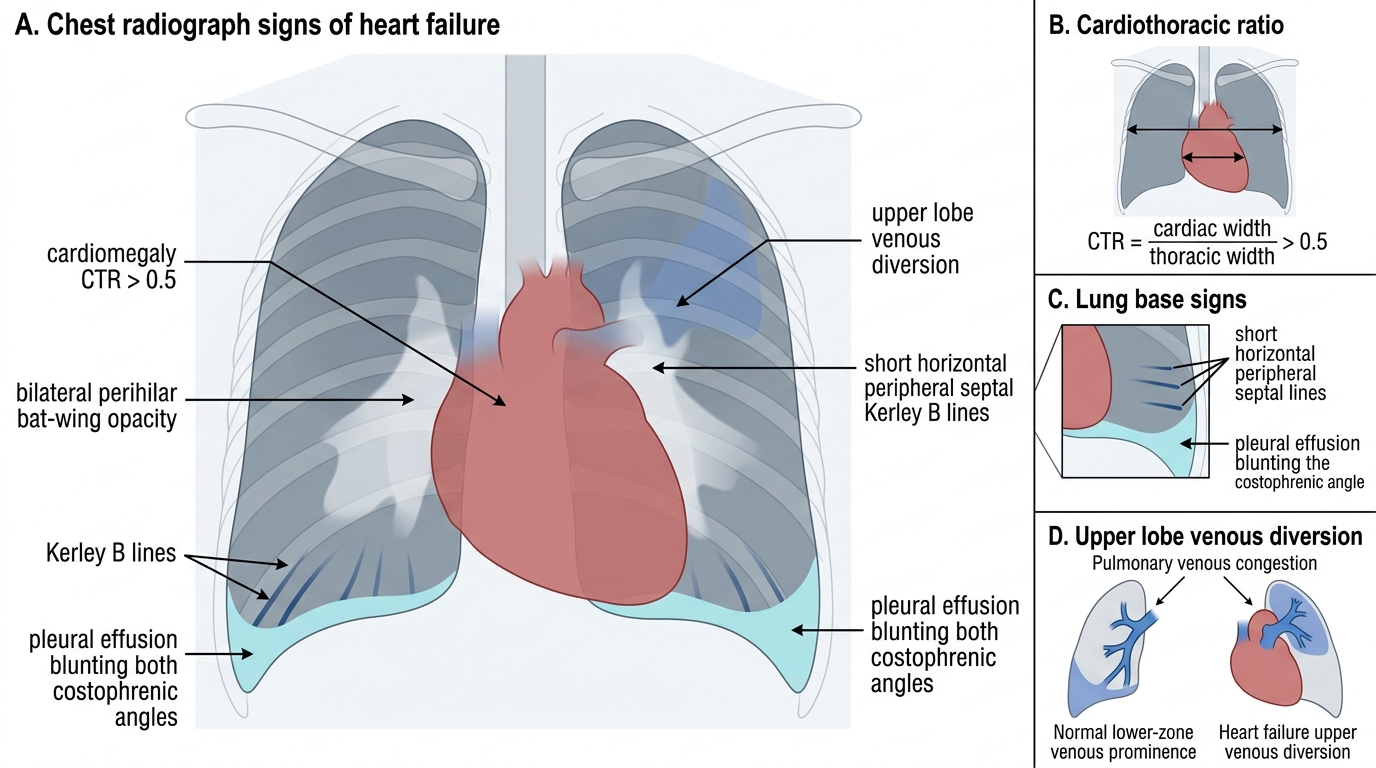
Chest Radiograph Signs of Heart Failure
SELF-CHECK
A 68-year-old woman is referred with exertional dyspnoea and ankle swelling. Her ECG shows left ventricular hypertrophy with strain and AF with a ventricular rate of 90 bpm. CXR shows cardiomegaly and upper-lobe venous diversion. Her BNP returns at 680 pg/mL. Her CHA₂DS₂-VASc score is 4 (female sex, age ≥65, hypertension, HF). Which of the following management decisions is DIRECTLY informed by the CHA₂DS₂-VASc score?
A. The decision to start a beta-blocker for rate control
B. The decision to perform an echocardiogram
C. The decision to anticoagulate for stroke prevention
D. The decision to order a coronary angiogram
Reveal Answer
Answer: C. The decision to anticoagulate for stroke prevention
The CHA₂DS₂-VASc score is specifically designed to stratify stroke risk in atrial fibrillation and guide the decision about anticoagulation. A score ≥2 in men or ≥3 in women warrants anticoagulation. This patient's score of 4 clearly indicates anticoagulation is needed. Beta-blockers are guided by rate control need and LVEF, not CHA₂DS₂-VASc. Echocardiography is ordered based on the clinical need to classify HF type. Coronary angiography is guided by ischaemic aetiology suspicion, not AF stroke score.