Page 9 of 25
IM1.15-18 | Heart Failure Investigations — SDL Guide (Part 2)
Echocardiography, BNP, Exercise Testing, Nuclear Medicine, and Coronary Angiography
2D Echocardiography with Doppler is the cornerstone investigation for the definitive classification and aetiological assessment of heart failure. It provides non-invasive, real-time information about cardiac structure and function that cannot be obtained from any other single modality. In Indian practice, where the burden of rheumatic valvular disease and hypertensive cardiomyopathy is high, echocardiography is essential for every patient with confirmed or suspected heart failure.
Key echocardiographic parameters and their interpretation:
Left ventricular ejection fraction (LVEF): The primary parameter for classifying heart failure. LVEF is calculated from LV end-diastolic volume (EDV) and end-systolic volume (ESV): LVEF = (EDV − ESV) / EDV × 100. By the 2021 ESC classification: HFrEF ≤40% (systolic dysfunction, the ventricle fails to eject adequately); HFmrEF 41–49% (mildly reduced, previously termed 'borderline' or 'mid-range'); HFpEF ≥50% (diastolic dysfunction, the ventricle fails to fill adequately despite preserved ejection). This classification directly drives pharmacological management — neurohormonal agents (ACE inhibitors, beta-blockers, MRA) have strong evidence only in HFrEF.
Diastolic function assessment: In HFpEF, the LVEF is preserved but diastolic filling is impaired. Doppler indices include: E/A ratio (early-to-late diastolic mitral inflow velocity ratio; E/A <1 indicates impaired relaxation = grade I diastolic dysfunction), E/e' ratio (E = early mitral inflow, e' = early diastolic mitral annular velocity by tissue Doppler; E/e' >14 suggests elevated filling pressures = grade II or III diastolic dysfunction), and left atrial volume index (LAVi >34 mL/m² indicates chronically elevated LA pressures).
Valvular assessment: Doppler echocardiography quantifies valvular stenosis (peak gradient, mean gradient, valve area) and regurgitation (regurgitant volume, regurgitant fraction, vena contracta). In rheumatic mitral stenosis, mitral valve area (MVA) by planimetry or pressure half-time: mild >1.5 cm², moderate 1.0–1.5 cm², severe <1.0 cm². Severe aortic stenosis: peak gradient >40 mmHg, mean gradient >20–25 mmHg, aortic valve area (AVA) <1.0 cm².
Brain natriuretic peptide (BNP) revisited: In addition to its diagnostic role, serial BNP/NT-proBNP measurements guide the intensity of treatment and predict prognosis. A 30–50% reduction in NT-proBNP during hospitalisation predicts lower 30-day readmission risk. Persistent elevation despite treatment signals need for escalation.
Exercise testing in heart failure serves two purposes. (1) Assessment of exercise capacity: A formal cardiopulmonary exercise test (CPET) measures peak VO₂ (oxygen consumption per unit time at maximum effort) — the gold standard for functional capacity assessment, used in HF with reduced EF to determine transplant candidacy (peak VO₂ <12–14 mL/kg/min = high priority for transplant listing). (2) Detection of inducible ischaemia: A standard treadmill exercise test with ECG monitoring (Bruce protocol) assesses for ST-segment changes, symptoms, and haemodynamic response that suggest underlying coronary artery disease as the cause of cardiomyopathy.
Nuclear medicine testing (radionuclide ventriculography, myocardial perfusion imaging): Radionuclide angiography (MUGA scan) provides highly reproducible LVEF measurements without the image-quality limitations of echocardiography in patients with poor acoustic windows (obesity, emphysema). Myocardial perfusion imaging (MPI) using Tc-99m sestamibi or thallium-201 with exercise or pharmacological stress (adenosine, dobutamine) identifies areas of reversible perfusion defect (ischaemia — viable myocardium that is underperfused at stress but perfused at rest) versus fixed defects (infarcted, non-viable myocardium). This guides the decision for revascularisation — reversible defects respond to revascularisation; fixed defects do not.
Coronary angiography (cardiac catheterisation): The invasive gold standard for anatomical assessment of coronary artery disease. Indicated when: (1) ischaemic cardiomyopathy is suspected (new heart failure with risk factors for CAD, or regional wall motion abnormalities on echo suggesting ischaemia), (2) evaluation for possible revascularisation before surgery or device therapy, (3) chest pain with heart failure where non-invasive tests are inconclusive. CT coronary angiography (CTCA) is a non-invasive alternative with high negative predictive value for excluding significant CAD, appropriate in low-to-intermediate pre-test probability patients.
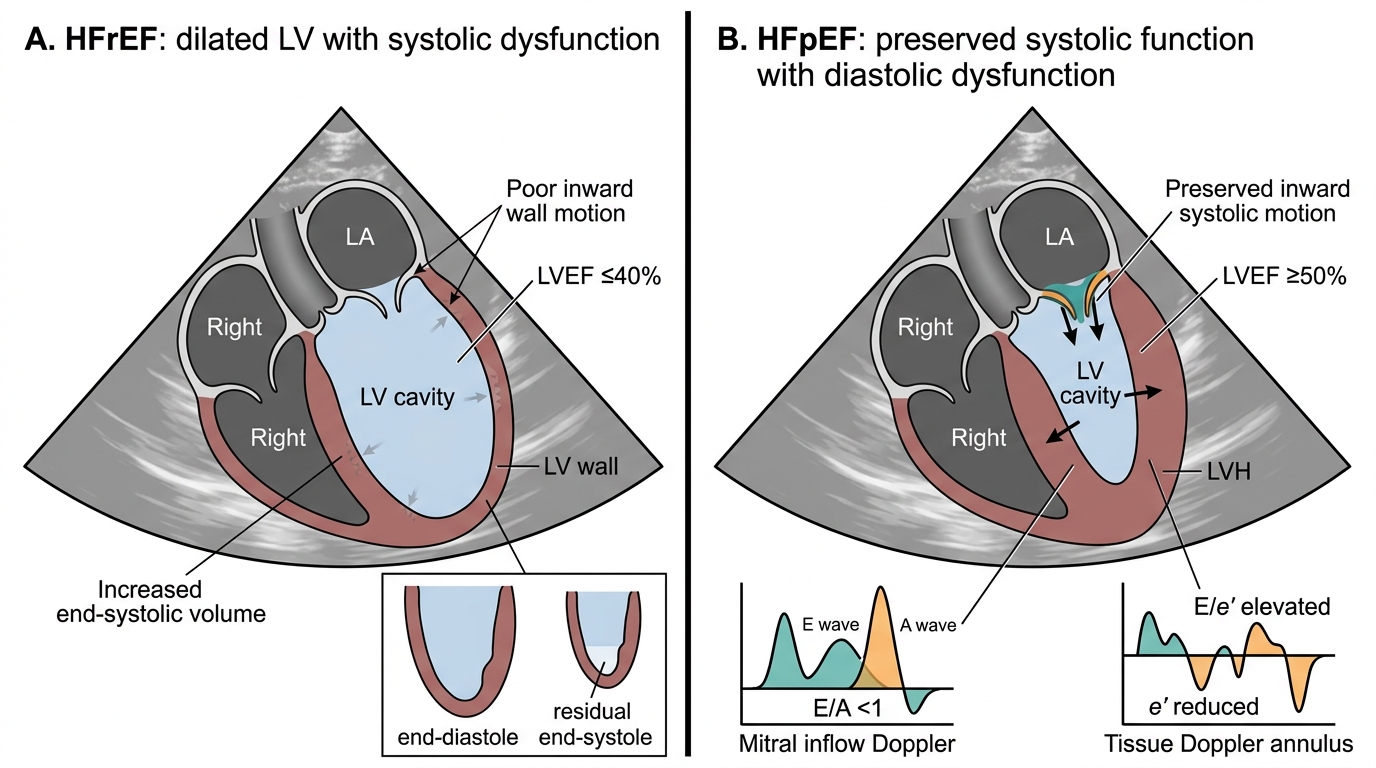
Echocardiographic Differences Between HFrEF and HFpEF
Valvular Heart Disease Severity Assessment and Intervention Thresholds
The assessment of valvular heart disease severity is a core skill that directly determines management decisions, particularly the threshold for surgical or catheter-based intervention. Valvular disease is both a major cause of heart failure (rheumatic mitral stenosis, aortic stenosis, chronic mitral regurgitation) and a common complication of it (functional mitral regurgitation from LV dilatation). The severity of valvular dysfunction must be interpreted in the context of symptoms, ventricular function, and haemodynamics — a valve lesion that appears moderate on echo may warrant intervention if the patient has significant symptoms or LV dysfunction. In India, rheumatic heart disease remains the dominant cause of valvular heart disease affecting young adults, in contrast to the degenerative calcific aortic stenosis that predominates in elderly Western populations. This epidemiological reality means that a final-year Indian MBBS graduate must be proficient in recognising, quantifying, and managing both rheumatic and degenerative patterns. The echocardiographic parameters for severity grading, the staging system, and the specific intervention thresholds that follow represent the evidence-based framework that governs modern valvular disease management.
Provided image
The ACC/AHA 2021 Guidelines classify valvular heart disease into four stages:
- Stage A: At risk for VHD (risk factors present, no haemodynamic change).
- Stage B: Progressive VHD (mild to moderate VHD, asymptomatic, LVEF preserved).
- Stage C: Severe VHD, asymptomatic — subdivided as C1 (LVEF preserved and compensated) and C2 (LVEF reduced, ≤55–60% for AR or MR, or ≤50% for AS).
- Stage D: Severe VHD, symptomatic.
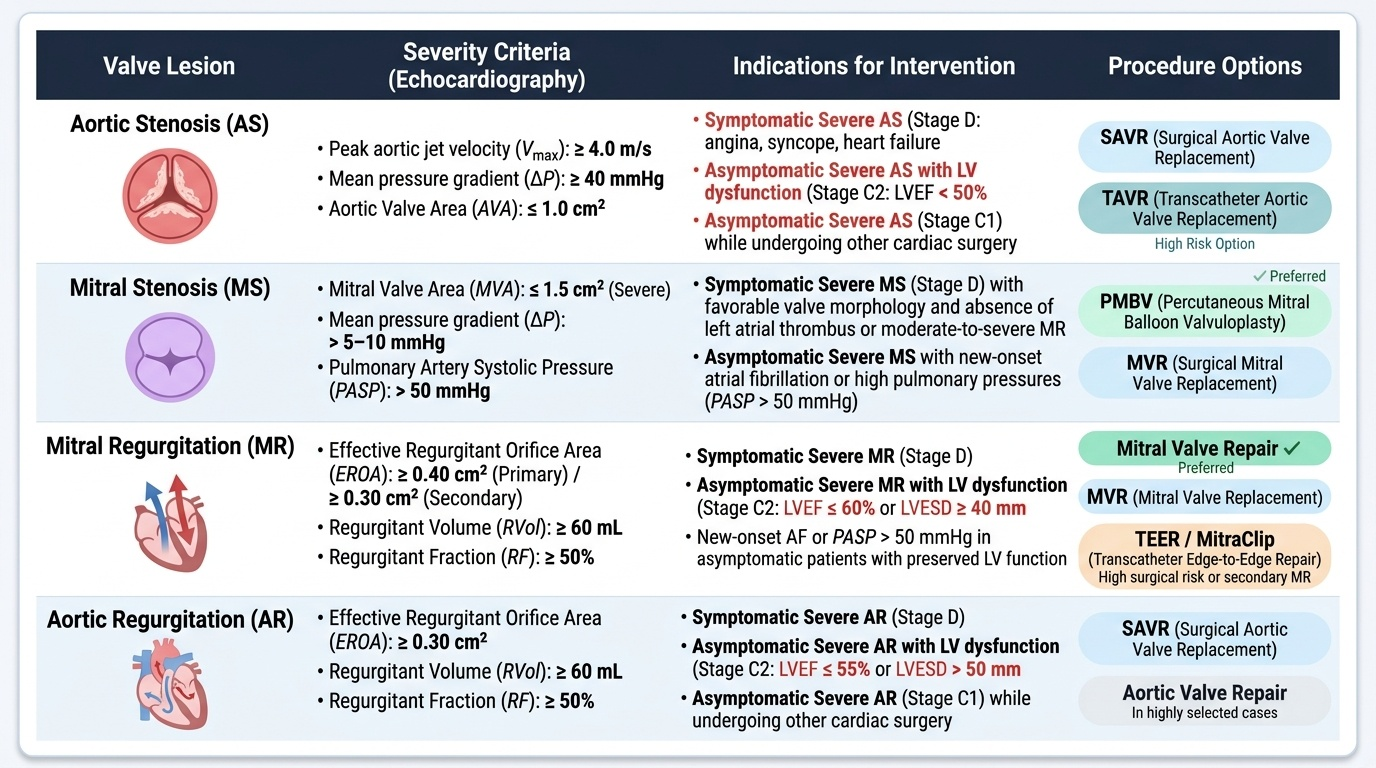
Aortic stenosis (AS): Severe AS is defined by: peak aortic jet velocity ≥4.0 m/s, mean pressure gradient ≥40 mmHg, and AVA ≤1.0 cm². Intervention is recommended in: (1) symptomatic severe AS (Stage D — symptoms of angina, syncope, or HF; the classic triad has a survival implication: mean survival after symptom onset is 2–5 years for angina, 3 years for syncope, and <2 years for heart failure without intervention), (2) asymptomatic severe AS (Stage C2) with LVEF <50%, (3) asymptomatic severe AS (Stage C1) undergoing other cardiac surgery. Transcatheter aortic valve replacement (TAVR) is the procedure of choice in high-surgical-risk patients; surgical aortic valve replacement (SAVR) in lower-risk patients <65 years.
Mitral stenosis (MS): Rheumatic MS remains prevalent in India, the Middle East, and South Asia. Severe MS: MVA <1.0 cm². Intervention options: (1) Percutaneous mitral balloon valvotomy (PMBV/PMV) — the preferred technique in suitable anatomy (pliable, non-calcified, non-thickened valve leaflets; minimal subvalvular disease; no MR >2+; no left atrial thrombus). The Wilkins score quantifies mitral valve morphology (each component — leaflet mobility, thickening, calcification, subvalvular apparatus — scored 1–4; total ≤8 predicts good outcome from PMBV). A Wilkins score >8 predicts worse balloon valvotomy outcomes and may favour surgical intervention. (2) Surgical mitral valve replacement (MVR) for unfavourable anatomy or significant MR.
Mitral regurgitation (MR): Severe MR: regurgitant volume ≥60 mL per beat, regurgitant fraction ≥50%, effective regurgitant orifice (ERO) ≥0.40 cm², vena contracta ≥0.7 cm. Intervention is recommended for: (1) symptomatic severe MR (Stage D), (2) asymptomatic severe MR (Stage C2) with LVEF 30–60% or LV end-systolic diameter ≥40 mm. Surgical MR repair is preferred over replacement when feasible (preserves LV function). MitraClip (transcatheter edge-to-edge repair) is an option for high-risk surgical candidates, particularly in secondary (functional) MR.
Aortic regurgitation (AR): Severe AR: regurgitant volume ≥60 mL, regurgitant fraction ≥50%, ERO ≥0.30 cm². Intervention recommended for: (1) symptomatic severe AR (Stage D), (2) asymptomatic severe AR (Stage C2) with LVEF ≤55%.
The clinical principle to emphasise: surgical or interventional therapy for valvular disease should be considered before irreversible LV dysfunction occurs — because once LVEF falls below the critical threshold (~50% for MR/AR, ~50% even in AS), the ventricle may not recover fully after valve correction, and prognosis is worse. The window between severe asymptomatic VHD and symptom onset is the optimal time for elective intervention.
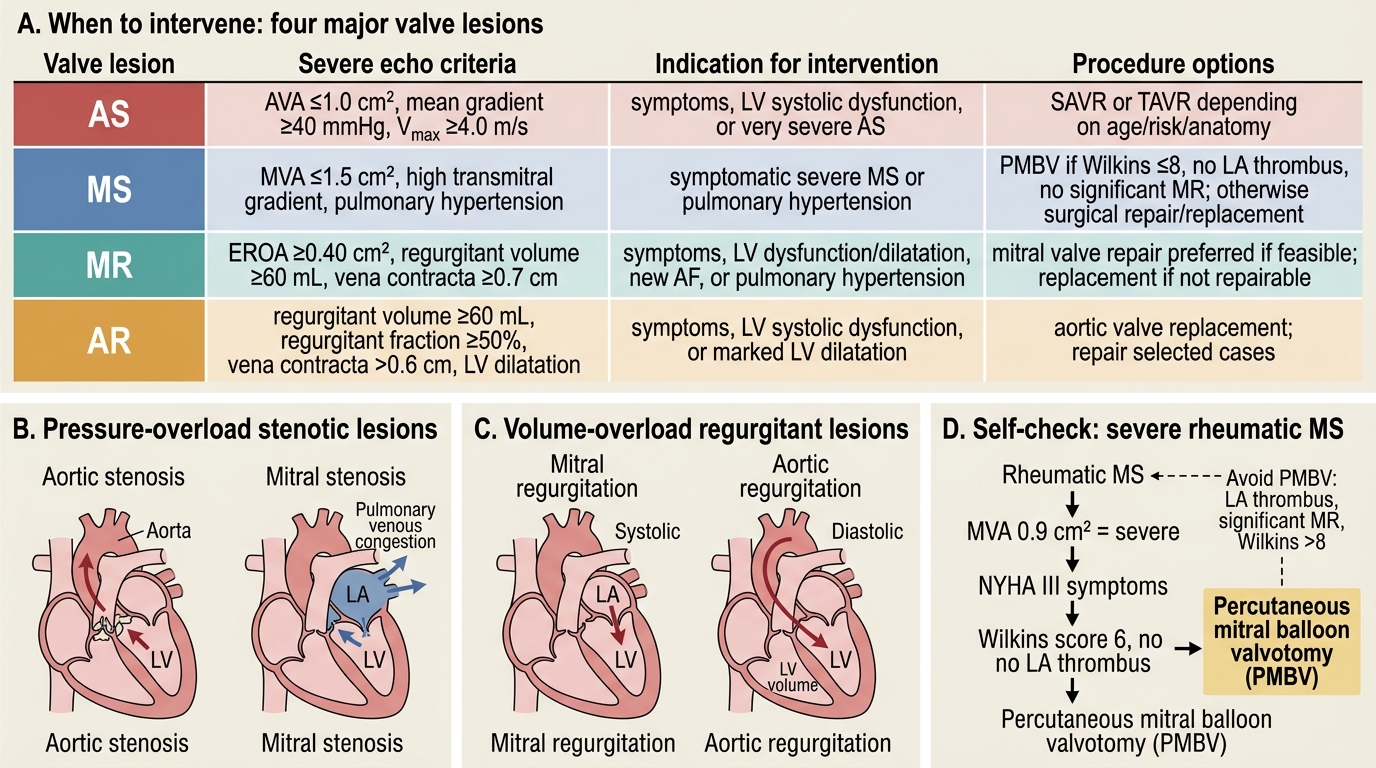
Indications for Intervention in Major Valve Lesions
SELF-CHECK
A 45-year-old woman with rheumatic mitral stenosis has a mitral valve area of 0.9 cm² on echocardiography. She reports NYHA class III symptoms (dyspnoea on minimal exertion). Her echocardiogram also shows a Wilkins score of 6, no mitral regurgitation, and no left atrial thrombus on TOE. What is the most appropriate next intervention?
A. Surgical mitral valve replacement
B. Percutaneous mitral balloon valvotomy (PMBV)
C. Increase diuretic dose and reassess in 3 months
D. Refer for cardiac transplantation listing
Reveal Answer
Answer: B. Percutaneous mitral balloon valvotomy (PMBV)
This patient has severe MS (MVA 0.9 cm²) with NYHA class III symptoms — a clear indication for intervention. The Wilkins score of 6 (≤8) with pliable, non-calcified valve, no significant MR, and no LA thrombus indicates favourable anatomy for PMBV — the preferred, less invasive option before considering surgical replacement. A score ≤8 predicts good outcome from balloon valvotomy. Surgical MVR is reserved for unfavourable anatomy (Wilkins >8) or significant MR. Medical therapy alone in a symptomatic patient with severe MS is inadequate. Transplantation is not indicated for correctable valvular disease.
Interpretation of Findings and Their Integration
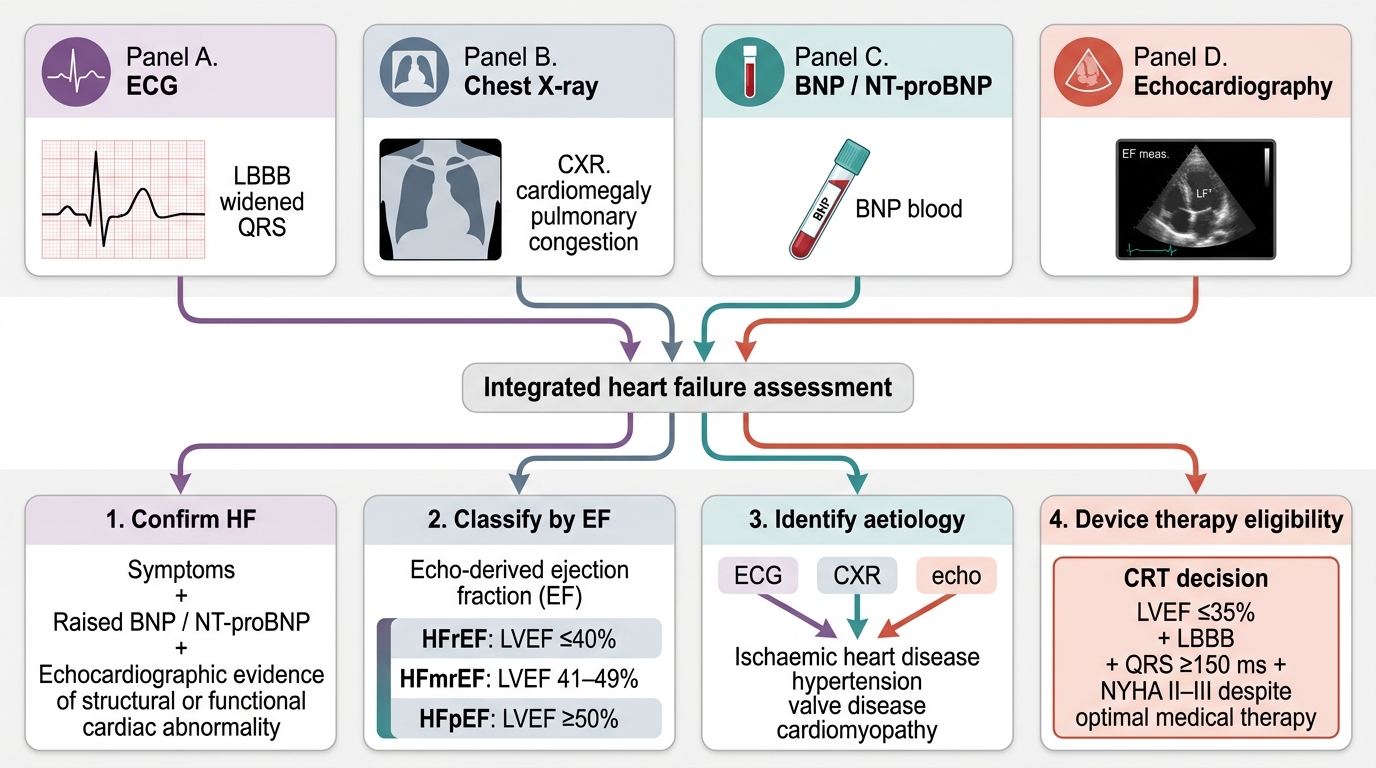
Integrating multiple investigation findings into a coherent clinical picture is the highest-order skill in heart failure assessment. No investigation should be interpreted in isolation — the ECG, CXR, biomarkers, and echocardiogram together provide a far richer assessment than any single test. The following synthesis framework guides integration of findings.
The first question is always: does this patient have heart failure? The combination of elevated BNP (>35–100 pg/mL) with relevant ECG and CXR findings confirms that further investigation — specifically echocardiography — is warranted. A completely normal ECG and a BNP <35 pg/mL make heart failure very unlikely (negative predictive value >90%), prompting reconsideration of alternative diagnoses (COPD, deconditioning, anaemia, pulmonary embolism).
The second question: what type of heart failure? Echocardiography answers this definitively via LVEF: HFrEF ≤40%, HFmrEF 41–49%, HFpEF ≥50%. This classification has direct pharmacological implications — ACE inhibitors/ARBs, beta-blockers, and mineralocorticoid receptor antagonists have proven mortality benefit only in HFrEF. SGLT2 inhibitors (empagliflozin, dapagliflozin) have now shown benefit across the entire EF spectrum, including HFpEF.
The third question: what is the aetiology? ECG Q waves and regional wall motion abnormalities on echo suggest ischaemic cardiomyopathy → coronary angiography. LVH on ECG plus concentric LV hypertrophy with preserved EF and diastolic dysfunction on echo → hypertensive heart disease. Valvular disease on echo (rheumatic MS or AR, degenerative AS, functional MR) → severity grading and intervention threshold assessment. Mildly dilated LV with global dysfunction and no CAD → dilated cardiomyopathy (investigate for viral causes, familial DCM, alcohol, thyroid, haemochromatosis).
The fourth question: are there device therapy indications? LBBB with QRS ≥150 ms + LVEF ≤35% + NYHA II–III on optimal medical therapy → CRT consideration. LVEF ≤35% + NYHA II–III despite 3+ months of optimal therapy → ICD consideration for sudden cardiac death prevention.
Serial monitoring: After treatment initiation, investigations are repeated to assess response. ECG for rhythm control and QRS duration. Repeat echocardiogram at 3–6 months to assess LVEF recovery (some patients with newly diagnosed cardiomyopathy may improve to HFmrEF or even HFpEF range with treatment). Serial BNP/NT-proBNP tracks congestion burden and guides diuretic titration.
Integrated Diagnostic Flow in Heart Failure
SELF-CHECK
A 55-year-old man with a known 3-year history of heart failure has an LVEF of 30% on his latest echocardiogram despite being on optimised doses of an ACE inhibitor, beta-blocker, and spironolactone for 6 months. His ECG shows sinus rhythm with LBBB, QRS duration 158 ms. He has NYHA class III symptoms. Which investigation finding MOST directly indicates eligibility for cardiac resynchronisation therapy (CRT)?
A. LVEF 30% on echocardiogram
B. NYHA class III symptoms
C. LBBB with QRS duration 158 ms on ECG combined with LVEF ≤35%
D. Elevated NT-proBNP despite optimal medical therapy
Reveal Answer
Answer: C. LBBB with QRS duration 158 ms on ECG combined with LVEF ≤35%
CRT (biventricular pacing) is indicated for patients with: LVEF ≤35%, NYHA class II–III on optimal medical therapy, and LBBB morphology with QRS duration ≥150 ms (Class I indication, ESC/ACC/AHA guidelines). While all four findings are present in this patient, it is the specific combination of LBBB with QRS ≥150 ms on the ECG and LVEF ≤35% on the echocardiogram that constitutes the evidence-based threshold for CRT eligibility. NYHA class and elevated BNP support the need for intervention but are not the defining criteria for CRT specifically.