Page 10 of 25
IM1.15-18 | Heart Failure Investigations — SDL Guide (Part 3)
Applied Practice: Case-Based Application and Common Pitfalls
The applied practice component tests your ability to map investigation findings to management decisions. Below are two case-based scenarios designed to consolidate the investigation principles covered in this module, followed by a systematic summary of common pitfalls in investigation interpretation.
Provided image
Case Scenario A — New Dilated Cardiomyopathy:
A 38-year-old man presents with 3 weeks of progressive dyspnoea. He has no prior cardiac history. He is a social drinker (approximately 30 units/week for 10 years). Examination: HR 105 bpm irregular, BP 95/65, JVP elevated 8 cm, displaced apex beat to left mid-axillary line, S3 gallop, bibasal crackles, bilateral pitting oedema to mid-shin. Investigations: ECG shows AF with rate 105 bpm and a non-specific left bundle branch block pattern (QRS 124 ms). CXR: cardiomegaly CTR 0.60, interstitial shadowing. BNP 1450 pg/mL. Echocardiogram: dilated LV (end-diastolic diameter 68 mm), LVEF 22%, global hypokinesia, trivial mitral regurgitation, no valvular stenosis. Interpretation: Dilated cardiomyopathy, likely alcoholic, with AF and NYHA class IV decompensation. AF with CHA₂DS₂-VASc 2 (male, HF, age <65) — borderline anticoagulation decision; AF with LVEF ≤35% and HF is a strong indication. Next step: coronary angiography (or CTCA) to exclude ischaemic cause. Thyroid function (AF precipitant). Consider abstinence counselling — alcoholic cardiomyopathy may partially or fully recover with alcohol cessation. QRS 124 ms — if after 3–6 months of optimal medical therapy LVEF remains ≤35% and QRS ≥150 ms, reassess for CRT. ICD after 3 months if LVEF remains ≤35%.
Case Scenario B — Rheumatic Mitral Stenosis Decompensation:
A 32-year-old woman from rural Andhra Pradesh presents with severe dyspnoea at rest and haemoptysis. She reports known rheumatic heart disease diagnosed at age 14. Examination: malar flush, low-volume pulse, AF with rate 115 bpm, prominent a/v waves on JVP, palpable P2, apical rumbling diastolic murmur with opening snap. CXR: double right heart border (LA enlargement), elevation of left main bronchus, straightened left heart border, Kerley B lines. Echocardiogram: MVA 0.85 cm² by planimetry, Wilkins score 5, no MR, LA dimension 58 mm. TOE: no LA thrombus. Interpretation: Severe rheumatic MS (MVA <1.0 cm²) with acute decompensation precipitated by AF with rapid ventricular response. Wilkins score 5 — favourable anatomy for PMBV. Plan: rate control (beta-blocker or digoxin), anticoagulation (AF in MS — high stroke risk), diuresis for decongestion, then PMBV after haemodynamic stabilisation.
Common investigation pitfalls:
1. Ordering echo before BNP in the emergency setting — BNP is faster and cheaper, and a very low BNP excludes HF, saving the echo slot.
2. Misinterpreting a normal ECG as excluding heart failure — a normal ECG reduces the likelihood of HF but does not exclude it, particularly in HFpEF.
3. Forgetting to calculate CHA₂DS₂-VASc in every patient with AF and heart failure — this directly determines anticoagulation need.
4. Confusing HFpEF for a normal heart — patients with HFpEF have diastolic dysfunction, elevated filling pressures, and exercise intolerance requiring specific management; the preserved EF is not reassuring.
5. Using exercise testing without first ensuring the patient is not in acute decompensation — exercise testing is contraindicated in decompensated HF.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
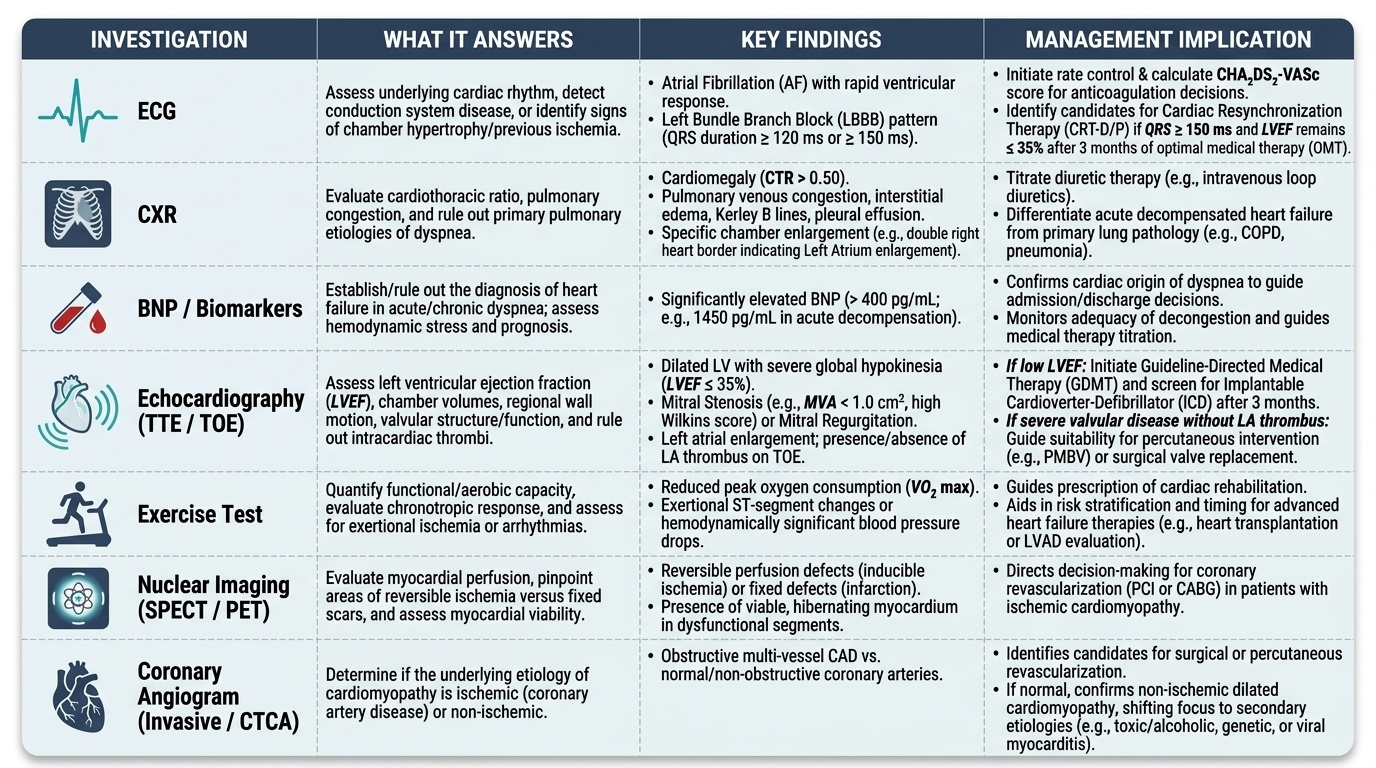
Heart Failure Investigations: Decision Support Summary
CLINICAL PEARL
The ECG in heart failure almost never shows a completely normal pattern — a truly normal ECG in a patient with suspected HF should prompt serious reconsideration of the diagnosis, particularly if the BNP is also below 35 pg/mL. The combination of a normal ECG and a low BNP has a >95% negative predictive value for ruling out heart failure as the cause of dyspnoea.
A second critical pearl: in rheumatic mitral stenosis in India, always perform TOE (transoesophageal echocardiogram) before PMBV to exclude left atrial thrombus — a thrombus in the left atrial appendage is a contraindication to balloon valvotomy and mandates anticoagulation for at least 3 months before reassessment. Missing this step can result in catastrophic systemic embolisation during the procedure.
Self-Assessment: Investigation Vignettes
At this point in the module you have covered the full investigation toolkit for heart failure: ECG interpretation, CXR analysis, BNP/NT-proBNP thresholds, echocardiographic parameters for EF classification and valvular severity, exercise testing, nuclear imaging, and coronary angiography. The self-assessment vignettes below are designed to test integration of these skills under examination-like conditions. For each vignette, formulate your investigation interpretation and management implication before reading the answer.
A note on the NMC competency framework: IM1.16 (perform and interpret a 12-lead ECG) is at the SH (Skill with Hands-on) level — meaning you must be able to physically perform an ECG (connect leads correctly, run the trace) and interpret it at the bedside. IM1.17 (enumerate indications for and describe findings of echo, BNP, exercise, nuclear, angiogram) is at the KH level — meaning you must know when to order these tests and what the expected findings mean, but you are not expected to personally perform them. This distinction guides how you approach each block in your exam preparation.
Vignette 1: An ECG shows: heart rate 78 bpm, regular rhythm, P waves absent, irregular narrow complex QRS, baseline fibrillatory waves. What is the rhythm, and what score should you calculate for anticoagulation decision-making?
Answer: Atrial fibrillation (narrow complex, irregularly irregular, absent P waves, fibrillatory baseline). Calculate CHA₂DS₂-VASc score. Anticoagulate if score ≥2 (men) or ≥3 (women).
Vignette 2: An echocardiogram reports LVEF 48%, grade II diastolic dysfunction (E/A ratio 0.8, E/e' ratio 16), LAVi 38 mL/m², LVH with wall thickness 13 mm. What type of heart failure does this represent, and which pharmacological agents have proven mortality benefit?
Answer: HFmrEF (LVEF 41–49%) with diastolic dysfunction and elevated filling pressures (E/e' 16 >14). SGLT2 inhibitors (empagliflozin, dapagliflozin) have benefit across the EF spectrum including HFmrEF and HFpEF. ACE inhibitors/beta-blockers/MRA have strong mortality evidence only in HFrEF (≤40%); evidence in HFmrEF is less robust — use based on aetiology and coexisting conditions.
Vignette 3: A patient with newly diagnosed heart failure and LVEF 25% undergoes a myocardial perfusion imaging (MPI) scan. The scan shows a fixed defect in the inferior wall and a large reversible defect in the anterior wall. What does this mean and what does it imply for management?
Answer: Fixed defect = non-viable infarcted myocardium (inferior wall — likely RCA territory, prior MI). Reversible defect = viable but ischaemic myocardium (anterior wall — LAD territory) — this myocardium can potentially recover function with revascularisation. The reversible defect is an indication for coronary angiography to assess suitability for coronary revascularisation (PCI or CABG), which may improve LVEF and symptoms. This phenomenon — improvement of LV function after revascularisation of hibernating myocardium — is called myocardial hibernation.
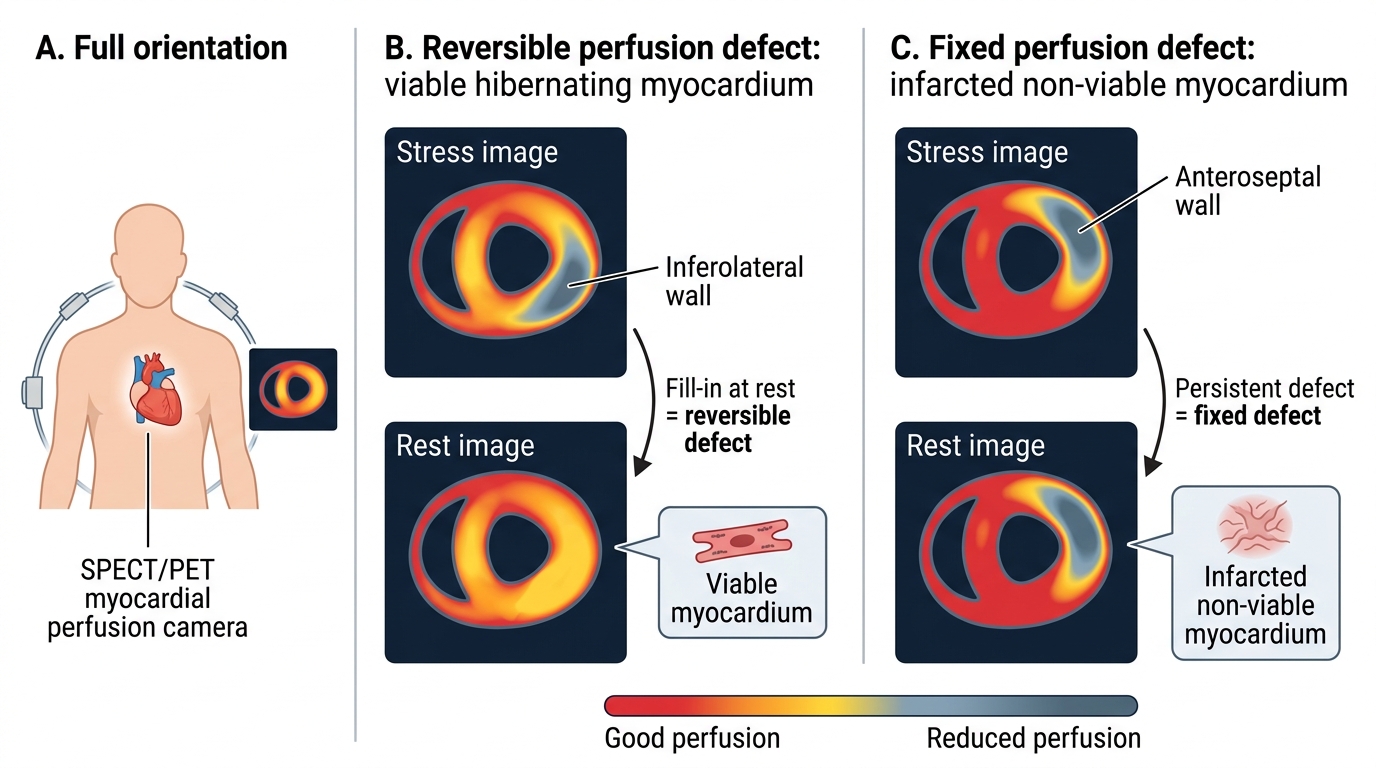
Reversible vs Fixed Myocardial Perfusion Defects
SELF-CHECK
A 70-year-old man with established HFrEF (LVEF 35%) on ACE inhibitor, carvedilol, and spironolactone presents with worsening dyspnoea over 2 weeks. His ECG is unchanged from baseline. His NT-proBNP has risen from 800 pg/mL (3 months ago) to 2800 pg/mL today. His renal function and electrolytes are stable. What does the rising NT-proBNP most directly indicate, and what is the priority management step?
A. The ECG shows new LBBB requiring CRT assessment
B. The rising NT-proBNP indicates worsening haemodynamic congestion requiring up-titration of diuretic therapy
C. The patient needs urgent coronary angiography for suspected new ischaemia
D. The LVEF has likely improved to HFmrEF range, reducing medication need
Reveal Answer
Answer: B. The rising NT-proBNP indicates worsening haemodynamic congestion requiring up-titration of diuretic therapy
NT-proBNP is a direct biomarker of ventricular wall stress caused by haemodynamic congestion. A 3.5-fold rise from baseline in a patient with worsening dyspnoea indicates increased filling pressures — the hallmark of cardiac decompensation. The priority is to address the congestion, which requires up-titration of diuretic therapy (loop diuretic dose increase, with monitoring of renal function and electrolytes). CRT assessment requires LBBB with QRS ≥150 ms — not mentioned here. Coronary angiography is not indicated without ECG changes or other ischaemia markers. Rising NT-proBNP indicates worsening, not improvement, of cardiac function.