Page 12 of 25
IM1.19-20 | Infective Endocarditis in Heart Failure — SDL Guide
Learning Objectives
- Describe and discuss the clinical features, diagnostic criteria (Duke criteria), and echocardiographic findings of infective endocarditis
- Enumerate the causative organisms in acute and subacute endocarditis and identify high-risk patient groups
- Discuss the pathogenesis of infective endocarditis and its complications including cardiac and embolic events
- Outline the principles of antimicrobial therapy and the indications for surgical intervention
- Demonstrate the correct technique for blood culture specimen collection in suspected endocarditis
INSTRUCTIONS
Infective endocarditis is a life-threatening infection of the endocardial surface of the heart — most often the native or prosthetic heart valves. It can present insidiously over weeks or explosively over days, and carries a mortality of 15–30% even with modern treatment. This module covers the full clinical spectrum: pathogenesis, clinical presentation, the Duke criteria for diagnosis, key investigations including echocardiography and blood cultures, and the principles of medical and surgical management.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 155 — Infective Endocarditis (textbook)
- API Textbook of Medicine, 10th ed., Ch. 9 — Infective Endocarditis (textbook)
- ESC Guidelines for the Management of Infective Endocarditis, 2023 (guideline)
- AHA/ACC Scientific Statement: Infective Endocarditis in Adults, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man with a history of injection drug use presents to the emergency department with 10 days of fever, chills, and progressive breathlessness. He has never been diagnosed with heart disease. On examination his temperature is 38.9°C, heart rate 112 bpm, and blood pressure 88/56 mmHg. A new pansystolic murmur is audible at the left lower sternal border. His fingernails show splinter haemorrhages and there are tender, erythematous nodules on the pulp of his fingers. A chest radiograph shows multiple bilateral nodular opacities. You take three sets of blood cultures and send an urgent echocardiogram request. The transthoracic echocardiogram reports a 1.2 cm oscillating vegetation attached to the tricuspid valve, with moderate tricuspid regurgitation. Blood cultures flag positive at 18 hours — two sets growing Staphylococcus aureus. The diagnosis is acute infective endocarditis of the tricuspid valve — right-sided IE in an intravenous drug user, with septic pulmonary emboli explaining the chest X-ray findings. Every clinical sign in this presentation has a name, a pathogenesis, and a diagnostic implication that you will master in this module.
WHY THIS MATTERS
Infective endocarditis sits at the intersection of cardiology, infectious disease, and surgery. It is a condition where early diagnosis literally saves lives — a delay of 24–48 hours in initiating appropriate antibiotics can be the difference between cure and irreversible valve destruction, embolic stroke, or haemodynamic collapse. In the Indian clinical context, the epidemiology carries particular importance: rheumatic heart disease remains the dominant predisposing cardiac condition (unlike the West, where prosthetic valves and degenerative disease predominate), meaning that a large proportion of Indian IE patients are young adults with previously identified or undiagnosed rheumatic valve disease. IVDU-associated IE, healthcare-associated IE (from indwelling venous catheters, haemodialysis access, and cardiac devices), and IE complicating congenital heart disease are all encountered in Indian tertiary hospitals. The NMC competency IM1.19 requires you to identify clinical features, echocardiographic findings, and therapy; IM1.20 requires you to demonstrate correct blood culture collection technique — both are assessed in practical and theory examinations.
RECALL
Activate your prior knowledge. The endocardium is the innermost layer of the heart, lining the chambers and covering the valves. Normal endothelium is thromboresistant — it does not attract platelet adhesion or bacterial colonisation. Recall the basic valve anatomy: the mitral valve (bicuspid, left AV valve) and aortic valve (trileaflet, left outflow valve) are the most commonly affected valves in IE — because the left-sided valves experience higher pressure and are more likely to be damaged by rheumatic disease. The tricuspid valve (right AV valve) is predominantly affected in IVDU-associated IE. Review the concept of bacteraemia — transient bloodstream invasion by bacteria following mucosal disruption (dental procedures, colonoscopy, urological procedures, skin infection, or IV drug injection). In a normal heart, transient bacteraemia is cleared rapidly and harmlessly. In a damaged heart, bacteria adhere to the abnormal endothelial surface and initiate infection.
Clinical Presentation: Acute vs Subacute Endocarditis
Infective endocarditis (IE) is an infection of the endocardial surface of the heart, most commonly affecting the cardiac valves, producing vegetations — masses composed of fibrin, platelets, inflammatory cells, and bacteria — that cause local valve destruction, embolism, and systemic sepsis. The clinical spectrum spans two poles that differ in tempo, organism, and presentation, and recognising which pole the patient inhabits guides the urgency of investigation and empirical therapy.
Acute infective endocarditis (AIE) presents over days to a few weeks with a fulminant, sepsis-like picture: high swinging fever, rigors, pronounced constitutional symptoms, haemodynamic compromise, and rapid valve destruction. The causative organism is almost invariably Staphylococcus aureus — a highly virulent organism capable of infecting previously normal valves. AIE is the form seen in intravenous drug users (IVDU), patients with healthcare-associated bacteraemia (central line infection, haemodialysis access, post-cardiac device implantation), and those with skin and soft tissue infections. The right-sided valves (tricuspid) are predominantly affected in IVDU, while left-sided involvement (mitral or aortic) produces more severe haemodynamic compromise and a higher risk of embolic stroke.
Subacute infective endocarditis (SIE) follows an indolent course over weeks to months, with low-grade or relapsing fever, fatigue, anorexia, weight loss, night sweats, and progressively worsening cardiac symptoms. The causative organisms are less virulent — most classically Streptococcus viridans group (oral streptococci, e.g., S. sanguis, S. mutans, S. mitis) that enter the bloodstream after dental manipulation in a patient with pre-existing valve disease. In India, rheumatic valve disease is the most important predisposing condition for SIE, as the scarred, thickened leaflets provide a nidus for bacterial adherence. Other pathogens include Streptococcus bovis/gallolyticus (associated with colonic pathology — always colonoscope these patients), Enterococcus faecalis (GI or urinary source), and HACEK organisms (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella — slow-growing gram-negative rods requiring prolonged incubation of blood cultures).
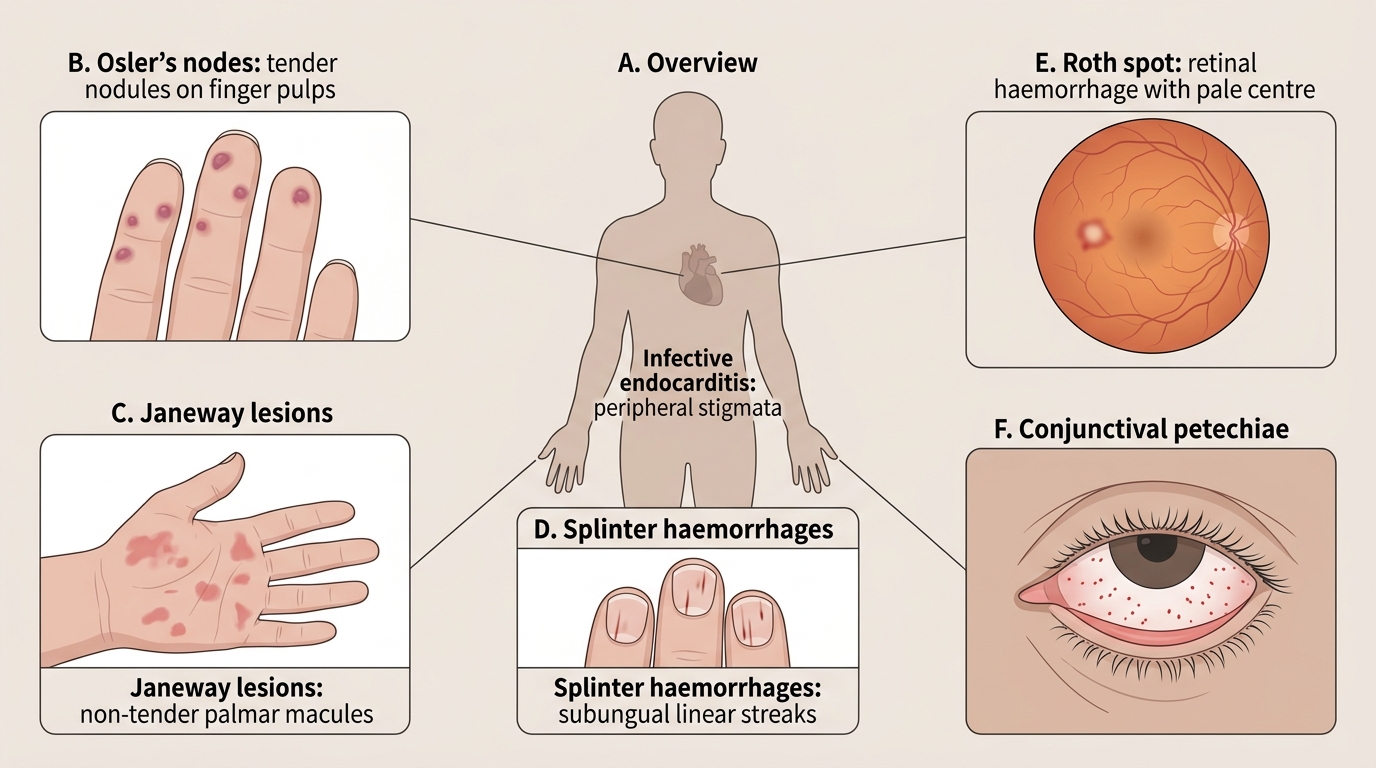
The classic peripheral stigmata of IE are the result of two mechanisms — immune complex deposition and septic microembolism — and their presence should immediately raise the diagnostic probability of IE in any febrile patient with a cardiac murmur:
- Osler's nodes: Tender, raised, erythematous nodules on the finger or toe pulps. Result from immune complex deposition and small vessel vasculitis. More common in SIE.
- Janeway lesions: Non-tender, flat, haemorrhagic macules on the palms and soles. Result from septic microemboli. More common in AIE (S. aureus).
- Roth spots: Boat-shaped haemorrhages with a pale centre on fundoscopy, caused by septic emboli to the retina.
- Splinter haemorrhages: Dark-red linear streaks under the nails (proximal position is more specific for IE; distal splinters may be traumatic).
- Finger clubbing: Appears in longstanding, subacute IE.
- Petechiae: On conjunctivae, skin, palate — from immune complex vasculitis and microembolism.
Cardiac features: a new or changed murmur is the most important auscultatory finding. The character of the murmur depends on the valve involved — a new aortic regurgitation murmur (early diastolic, decrescendo, left sternal border) in a febrile patient is infective endocarditis until proven otherwise. A new pansystolic murmur at the left lower sternal border in an IVDU = tricuspid regurgitation from right-sided IE. Heart failure may supervene rapidly in AIE from acute severe valvular regurgitation — this is the most common cause of death in IE and the most urgent indication for surgery.
Peripheral Stigmata of Infective Endocarditis
Pathogenesis of Infective Endocarditis
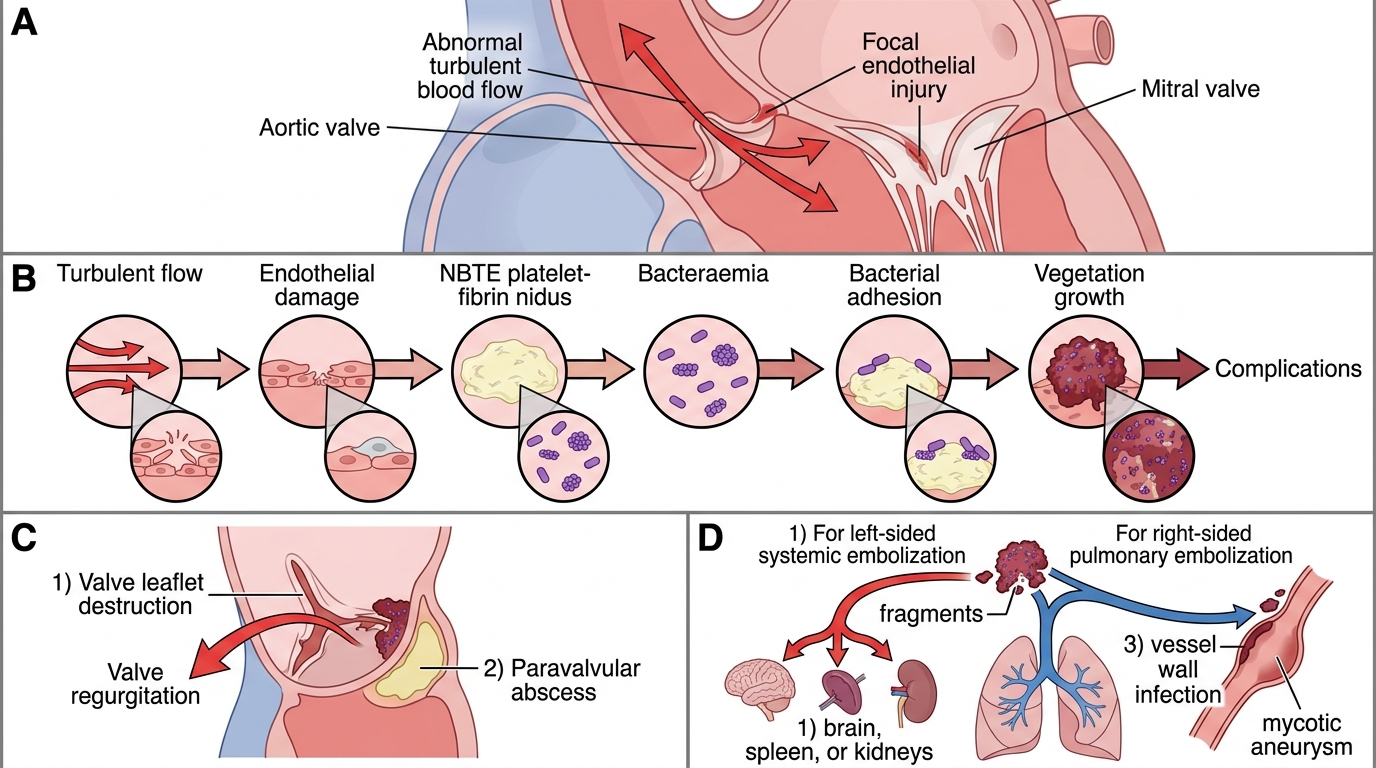
Understanding the pathogenesis of IE clarifies why certain patients are at risk, why particular valves are targeted, and how the clinical complications arise. The infection begins with a predictable sequence of events at the valve surface, progresses to vegetation formation, and then causes disease through two principal mechanisms: local structural destruction and distant embolism.
Step 1 — Endothelial injury and non-bacterial thrombotic endocarditis (NBTE): IE almost always begins with disruption of the normal thromboresistant endothelial surface of the valve. Turbulent blood flow across an abnormal valve (regurgitant jet, stenotic orifice, or the low-pressure downstream surface of a high-velocity jet) causes mechanical trauma to the endothelium, exposing the subendothelial collagen. Platelets adhere to the exposed collagen, and fibrin is deposited, forming a sterile thrombus called non-bacterial thrombotic endocarditis (NBTE) or marantic endocarditis. NBTE is the pre-existing nidus onto which bacteria subsequently colonise.
Step 2 — Bacteraemia and bacterial adhesion: During a bacteraemic episode, circulating bacteria contact the NBTE and adhere to it via surface proteins and polysaccharides. S. viridans streptococci express FimA (a surface adhesin) that binds to fibronectin on the NBTE surface. S. aureus uses fibronectin-binding proteins, clumping factor A, and coagulase to bind thrombus components and rapidly colonise even previously normal valves. The ability of an organism to adhere to NBTE is a key determinant of its virulence in IE.
Step 3 — Vegetation formation and immune evasion: Once adherent, bacteria multiply and trigger further fibrin and platelet deposition, engulfing the bacteria in a protective fibrin-platelet matrix — the vegetation. This matrix limits antibiotic penetration and protects the bacteria from phagocytosis and opsonisation. This is why bactericidal (not merely bacteriostatic) antibiotics, at high doses and for prolonged courses (4–6 weeks), are required — the bacteria within the vegetation are metabolically quiescent (stationary-phase organisms) and respond only to prolonged drug exposure.
Step 4 — Complications through destruction and embolism: The vegetation causes disease through two mechanisms operating simultaneously. (1) Local destruction: The inflammatory response and bacterial enzymes degrade the valve leaflets, producing progressive regurgitation (perforation, leaflet destruction) or rarely vegetation occlusion of the orifice (stenosis). Extension beyond the valve to the annulus or adjacent myocardium can create a paravalvular abscess — particularly common in aortic valve IE (aortic root abscess), presenting as new conduction defects (PR prolongation, bundle branch block) as the abscess extends into the conduction system. Aortic root abscess is an indication for urgent surgery. (2) Embolism: Fragments of the vegetation detach and embolise downstream. Left-sided IE → systemic arterial embolism: brain (ischaemic stroke — up to 20% of IE cases), spleen (splenic infarct, presenting as left-sided abdominal pain), kidney, and mesenteric vessels. Right-sided IE → pulmonary arterial embolism: septic pulmonary emboli manifest as multiple bilateral nodular or cavitating lung opacities on CXR/CT (as in the case vignette above). Mycotic aneurysms — infected aneurysmal dilations of arterial walls — can form at embolic sites, most dangerously in the cerebral circulation.
Predisposing cardiac conditions (high risk for IE):
- Prosthetic cardiac valves or prosthetic material used for valve repair
- Prior history of infective endocarditis
- Congenital heart disease (cyanotic CHD with unrepaired shunts, repaired CHD with prosthetic material within 6 months, repaired CHD with residual defects)
- Rheumatic valvular heart disease (high risk in Indian context)
- Hypertrophic obstructive cardiomyopathy (HOCM)
Predisposing patient conditions (high risk for bacteraemia):
- IVDU — direct inoculation of bacteria from skin flora and contaminated equipment
- Indwelling central venous catheters
- Chronic haemodialysis (arteriovenous fistula, tunnelled catheter)
- Diabetes mellitus, immunosuppression, HIV
- Poor dental hygiene or recent invasive dental procedure
Pathogenesis of Infective Endocarditis
Diagnosis: Duke Criteria, Blood Cultures, and Echocardiography
The diagnosis of infective endocarditis is established using the modified Duke criteria, which integrate the results of blood cultures, echocardiographic findings, and clinical features into a structured diagnostic framework that categorises cases as definite, possible, or rejected. The Duke criteria were originally proposed in 1994 and modified in 2000 (to add Q-fever serology as a major criterion and to refine the echocardiographic criterion); they provide a reproducible diagnostic standard that is widely used in clinical practice and research worldwide. The framework is valuable precisely because it forces the clinician to seek evidence systematically from three domains — microbiological, imaging, and clinical — before committing to a diagnosis, which prevents both over-diagnosis (treating culture-contamination as IE) and under-diagnosis (missing IE that lacks a classic vegetation). Understanding the criteria in detail is essential not only for examination success but for the real-world clinical decision of when to start empirical antibiotics, when to proceed to TOE, and when to refer for surgery.
The Duke criteria have two major categories and five minor categories:
Major criteria:
1. Positive blood cultures — bacteraemia with a typical IE pathogen:
- Two separate blood cultures growing a typical IE organism: S. viridans group, S. bovis, HACEK organisms, S. aureus, or community-acquired Enterococcus in the absence of a primary focus; OR
- Persistently positive blood cultures (≥2 drawn >12 hours apart, or ≥3 or the majority of ≥4 drawn with the first and last ≥1 hour apart) with an organism consistent with IE; OR
- Single positive culture for Coxiella burnetii or IgG antibody titre >1:800 (Q-fever endocarditis).
2. Evidence of endocardial involvement on echocardiography:
- Oscillating intracardiac mass on a valve or supporting structure or in the path of a regurgitant jet; OR
- Paravalvular abscess; OR
- New dehiscence of a prosthetic valve; OR
- New valvular regurgitation (not just worsening of pre-existing regurgitation).
Minor criteria:
1. Predisposing heart condition or IVDU
2. Fever ≥38°C
3. Vascular phenomena: major arterial emboli, septic pulmonary infarcts, intracranial haemorrhage, conjunctival haemorrhages, Janeway lesions
4. Immunological phenomena: glomerulonephritis, Osler's nodes, Roth spots, rheumatoid factor
5. Microbiological evidence: positive blood culture that does not meet major criteria OR serological evidence of active infection with an organism consistent with IE
Classification:
- Definite IE: 2 major criteria OR 1 major + 3 minor criteria OR 5 minor criteria (or pathological/histological confirmation)
- Possible IE: 1 major + 1 minor criteria OR 3 minor criteria
- Rejected: Firm alternative diagnosis, resolution with antibiotics ≤4 days, no pathological evidence at surgery/autopsy with antibiotics ≤4 days
Blood culture technique (IM1.20 — SH competency): Blood cultures are the single most important investigation in IE, and correct technique is critical to maximising sensitivity and minimising contamination. The principles are:
- Draw at least three separate sets of blood cultures from different peripheral venipuncture sites before starting any antibiotics. Each set = one aerobic + one anaerobic bottle.
- Volume is critical: each bottle requires 10 mL of blood (adults). Inadequate volume is the most common cause of false-negative blood cultures.
- Timing: ideally during a fever spike or rigor (maximum bacteraemia), but in practice the three sets should be taken over 1–2 hours to avoid delaying antibiotics. In acute haemodynamically unstable IE, take all three sets within 30 minutes and start antibiotics immediately. Do NOT wait 24–48 hours between collections.
- Aseptic technique: cleanse the venipuncture site with 70% isopropyl alcohol, then 2% chlorhexidine gluconate (or 10% povidone-iodine); allow to dry completely. Wear sterile gloves. Cleanse the bottle tops with an alcohol swab before inoculation. Blood cultures drawn through an existing central venous catheter have a high contamination rate and should NOT be used for diagnostic purposes in suspected IE.
- Prolonged incubation alert: for HACEK organisms (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) and Brucella, standard automated incubators may miss growth at 5 days — alert the laboratory to prolong incubation to 14–21 days if HACEK or culture-negative IE is suspected.
Echocardiography is the imaging modality of choice. Transthoracic echocardiography (TTE) is the first-line test — accessible, non-invasive, and diagnostic when a vegetation is clearly visualised. However, TTE has limited sensitivity for small vegetations (<5 mm), prosthetic valve IE (prosthesis creates acoustic shadowing), and paravalvular abscess detection. Transoesophageal echocardiography (TOE) is far superior: sensitivity for vegetation detection is 87–100% vs 50–63% for TTE; it is mandatory when: (1) TTE is non-diagnostic or non-adequate, (2) prosthetic valve IE is suspected, (3) perivalvular complications (abscess, fistula) are suspected, (4) IE involving intracardiac devices (pacemaker, defibrillator leads). TOE findings that drive management decisions: vegetation size (>10 mm correlates with higher embolic risk and may be an indication for early surgery), valve perforation or leaflet destruction, paravalvular abscess, fistula formation.
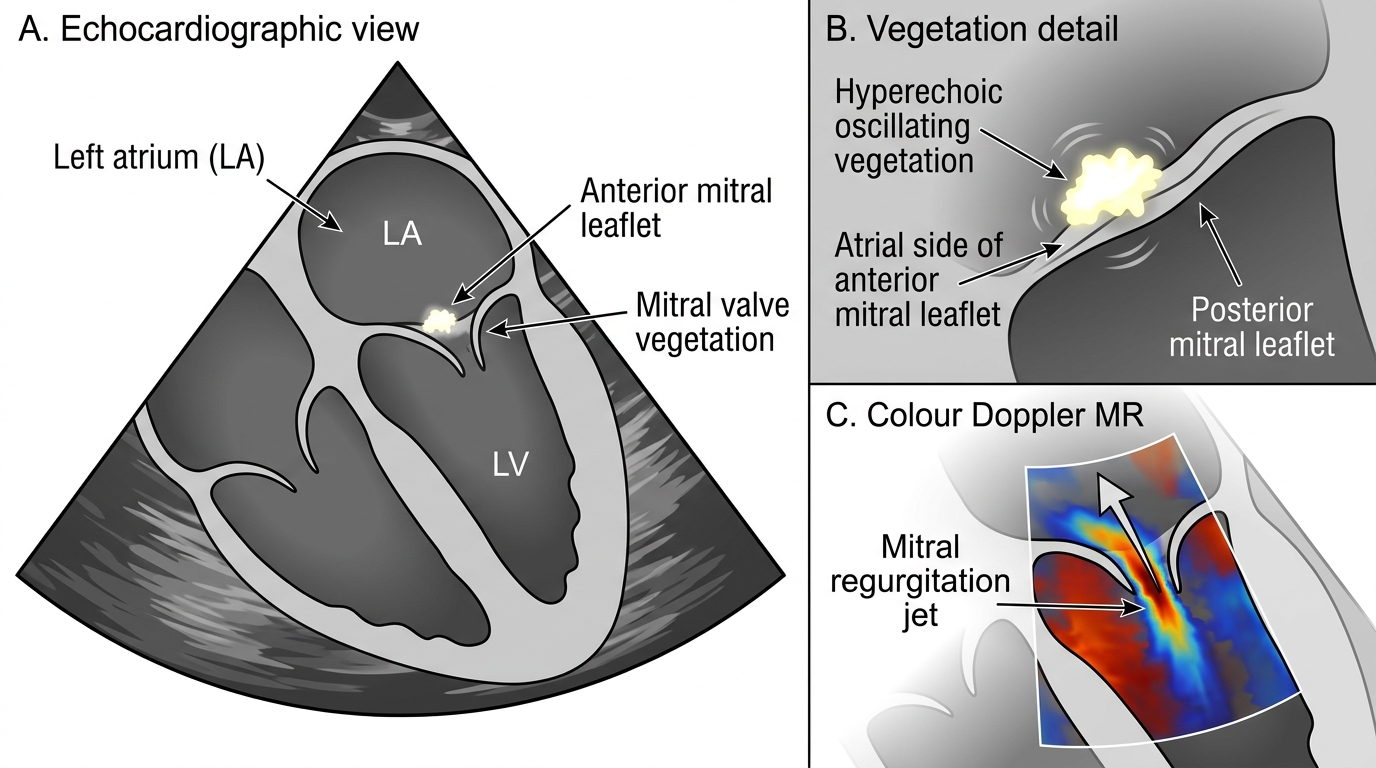
Mitral Valve Vegetation with Mitral Regurgitation
SELF-CHECK
A 35-year-old man with known rheumatic mitral valve disease presents with 3 weeks of fever, fatigue, and weight loss. On examination: temperature 38.2°C, a new systolic murmur over the mitral area, Osler's nodes on the finger pulps, and conjunctival petechiae. Three sets of blood cultures are drawn. Transthoracic echocardiogram shows a 7 mm oscillating vegetation on the mitral valve with moderate mitral regurgitation. According to the modified Duke criteria, how is this case classified?
A. Possible IE (1 major + 1 minor criterion)
B. Definite IE by pathological criteria only
C. Definite IE (2 major criteria — positive echo + positive blood cultures expected)
D. Definite IE (1 major + 3 minor criteria even before blood cultures return)
Reveal Answer
Answer: D. Definite IE (1 major + 3 minor criteria even before blood cultures return)
Before blood cultures return, the patient already has: Major criterion 1 = echocardiographic evidence of endocardial involvement (oscillating vegetation on mitral valve with new MR). Minor criteria met: (1) predisposing heart condition (rheumatic mitral valve disease), (2) fever ≥38°C, (3) immunological phenomena (Osler's nodes), (4) vascular phenomena (conjunctival petechiae). This gives 1 major + 4 minor criteria — exceeding the threshold for 'Definite IE' (requires 1 major + 3 minor). If both blood culture sets also return positive, a second major criterion is met (2 major = also Definite IE). The case is Definite IE even before cultures return, based on the echo finding plus four minor criteria.