Page 13 of 25
IM1.19-20 | Infective Endocarditis in Heart Failure — SDL Guide (Part 2)
Management: Antimicrobial Therapy and Surgical Indications
The management of infective endocarditis requires a coordinated multidisciplinary approach involving cardiology, infectious disease (or internal medicine with ID expertise), cardiac surgery, and microbiology — the so-called 'endocarditis team'. The two pillars of management are prolonged bactericidal antibiotic therapy and, in a significant minority of patients, cardiac surgery.
Antimicrobial principles: The fundamental rationale for prolonged therapy (4–6 weeks) in IE is the biology of the vegetation: bacteria within the fibrin-platelet matrix exist at extremely high density in a metabolically quiescent state, with limited antibiotic penetration and reduced susceptibility to cell-wall-active agents that require actively dividing bacteria. This is why bactericidal antibiotics (not merely bacteriostatic) are required — the objective is to achieve bactericidal drug concentrations within the vegetation throughout the treatment course.
Key empirical and pathogen-specific regimens:
Native valve IE, streptococcal (S. viridans group, penicillin-sensitive MIC ≤0.125 mg/L):
- Benzylpenicillin 12–18 MU/day IV in 4–6 divided doses for 4 weeks; OR
- Ceftriaxone 2 g/day IV or IM once daily for 4 weeks (preferred for outpatient completion).
- Gentamicin can be added for the first 2 weeks for synergy (aminoglycoside synergy) in uncomplicated cases, but nephrotoxicity must be monitored.
Native valve IE, Staphylococcus aureus (MRSA-negative/methicillin-sensitive MSSA):
- Flucloxacillin (or oxacillin) 2 g IV every 4 hours (12 g/day) for 4–6 weeks.
- For MRSA or penicillin-allergic patients: vancomycin 30–45 mg/kg/day in 2–3 divided doses (target trough 15–20 mg/L or AUC/MIC 400–600) for 6 weeks.
- Rifampicin is added in prosthetic valve IE only (not routine in native valve IE — may promote resistance).
Native valve IE, Enterococcus:
- Ampicillin + gentamicin for 4–6 weeks (gentamicin synergy essential for enterococcal endocarditis); OR
- Ampicillin + ceftriaxone (for gentamicin-resistant or high-level aminoglycoside resistance strains).
Culture-negative IE (10–15% of IE cases; caused by prior antibiotic treatment, fastidious organisms, or Coxiella, Bartonella, Tropheryma whipplei):
- Empirical: cover gram-positive cocci (including MRSA if healthcare-associated) plus HACEK organisms and Bartonella — vancomycin + doxycycline + gentamicin (modified by culture results and serology).
Prosthetic valve IE (PVE): Higher morbidity, higher surgical rate. Regimen depends on timing relative to surgery (early PVE <60 days — Staphylococcus epidermidis/aureus; late PVE >60 days — similar to native valve IE). Include rifampicin for staphylococcal PVE. Duration 6 weeks minimum.
Surgical indications in IE — surgery is the second pillar of management and is lifesaving in the following scenarios:
- Heart failure due to valve regurgitation — the most common and most urgent surgical indication. Acute severe aortic or mitral regurgitation causing pulmonary oedema or cardiogenic shock requires emergency surgery (even in the presence of active infection — surgery should not be delayed for antibiotic completion in this setting).
- Uncontrolled infection — persistent fever and bacteraemia despite 7–10 days of appropriate antibiotics, caused by resistant organisms (MRSA, fungi, Pseudomonas), paravalvular abscess, fistula, or false aneurysm.
- Prevention of embolism — vegetation size >10 mm on TOE (especially anterior mitral leaflet), particularly if recurrent embolic events occur despite adequate antibiotics. A second embolic event in the same patient while on antibiotics is a strong indication for surgery.
- Prosthetic valve IE — most cases of early PVE and many cases of late PVE complicated by paravalvular regurgitation, abscess, or persistent bacteraemia require surgery.
- Fungal IE — almost always requires surgery due to inability to achieve cure with antifungals alone.
Antibiotic prophylaxis for dental procedures is now recommended only for the highest-risk groups — those with prosthetic cardiac valves, prior history of IE, unrepaired cyanotic CHD, and certain repaired CHD within 6 months. The AHA/ESC guidelines no longer recommend prophylaxis for all patients with valvular heart disease, including rheumatic heart disease, because the evidence base is insufficient and indiscriminate prophylaxis promotes antibiotic resistance. Where recommended, the regimen is: amoxicillin 2 g orally 30–60 minutes before the procedure; clindamycin 600 mg for penicillin-allergic patients.
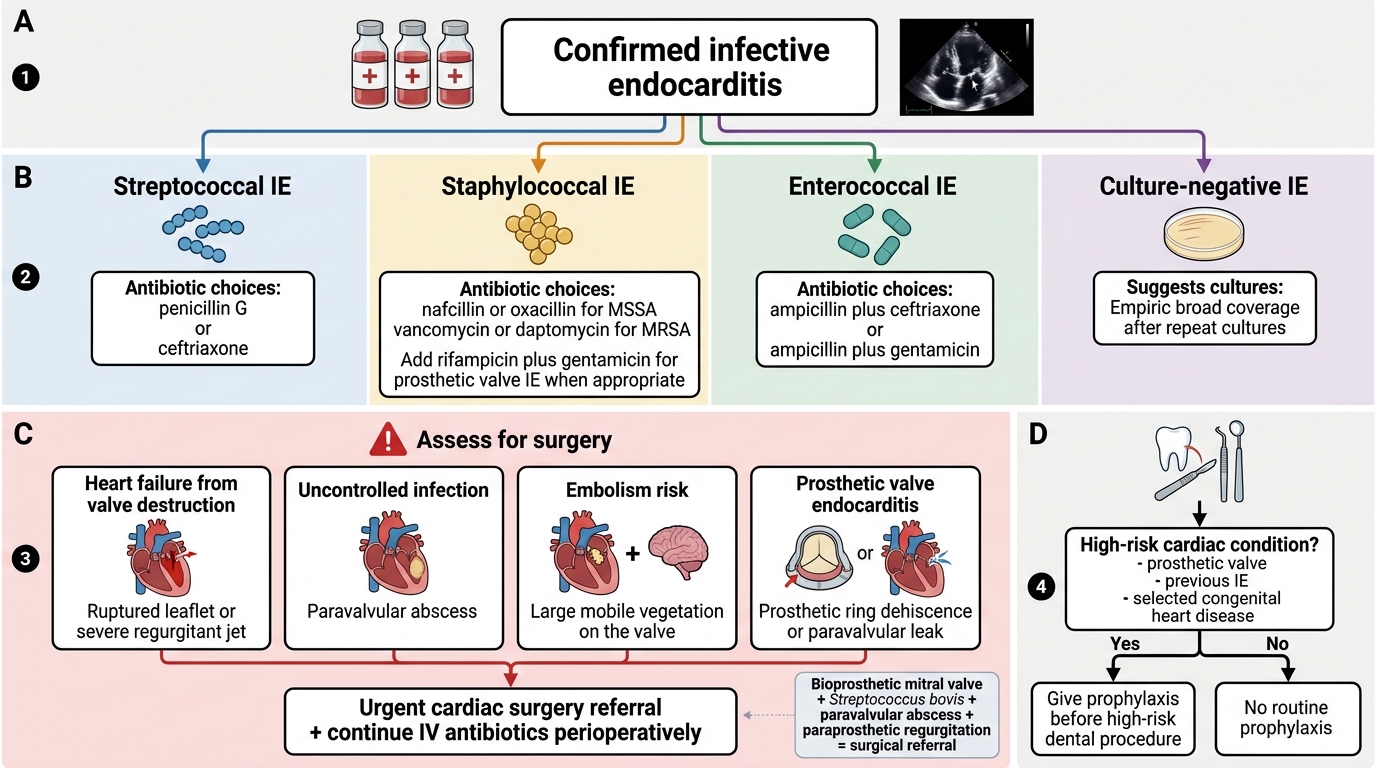
Management Algorithm for Infective Endocarditis
SELF-CHECK
A 52-year-old woman with a bioprosthetic mitral valve replacement (done 14 months ago) presents with 5 weeks of low-grade fever and fatigue. Blood cultures grow Streptococcus bovis. Transoesophageal echocardiogram shows a 6 mm vegetation on the bioprosthetic valve with a small paravalvular abscess and moderate paraprosthetic regurgitation. Which of the following management decisions is MOST appropriate?
A. Treat with ceftriaxone for 4 weeks and reassess; surgery only if she develops heart failure
B. Urgent surgical referral for prosthetic valve replacement, with antibiotics continued perioperatively
C. Start vancomycin for MRSA coverage as this is healthcare-associated prosthetic valve IE
D. Antibiotic therapy alone for 6 weeks is sufficient given the small vegetation size
Reveal Answer
Answer: B. Urgent surgical referral for prosthetic valve replacement, with antibiotics continued perioperatively
This is late prosthetic valve endocarditis (>60 days post-surgery) with a paravalvular abscess and paraprosthetic regurgitation — two surgical indications are present simultaneously: uncontrolled infection (paravalvular abscess indicating extension beyond the valve) and prosthetic valve dysfunction. The ESC/AHA guidelines recommend urgent surgery for prosthetic valve IE with abscess, new paravalvular regurgitation, or persistent infection. Antibiotic therapy alone is insufficient when a paravalvular abscess is present. While ceftriaxone is appropriate for susceptible streptococcal IE on a native valve, prosthetic valve IE requires 6-week regimens, and the structural complications mandate surgery. Vancomycin is for MRSA/penicillin allergy — organism here is streptococcal, not staphylococcal.
Complications and Prognostic Factors
Infective endocarditis is one of the few infectious conditions where the complications of the infection are as immediately life-threatening as the infection itself. Understanding the spectrum of complications allows the clinician to monitor for them actively rather than waiting for them to declare themselves late. The major complications arise from three pathological processes — local valve destruction, haematogenous seeding of distal organs, and immune complex deposition — and their relative frequency differs between acute (S. aureus dominant, rapid, embolic) and subacute (streptococcal dominant, insidious, immune-mediated) IE. Recognising complications early is critical because several of them — particularly acute heart failure from valve regurgitation, paravalvular abscess with conduction disturbance, and embolic stroke — are the primary triggers that convert a medically managed case into a surgical emergency. Serial clinical monitoring (daily auscultation for murmur change, daily ECG in aortic IE, daily neurological assessment), serial echocardiography, and serial inflammatory markers are therefore not optional extras but the core of IE surveillance during the treatment course.
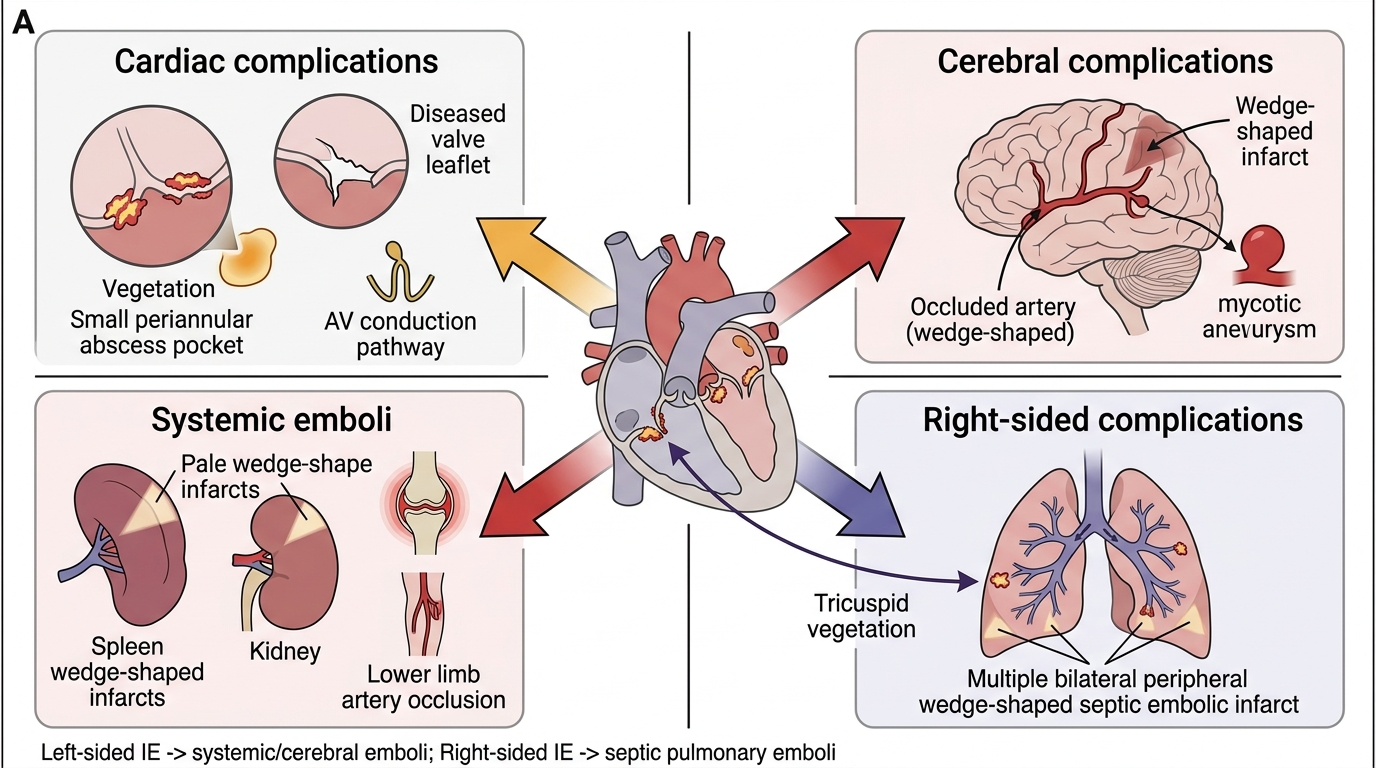
Cardiac complications:
- Acute heart failure from valve regurgitation: the most common cause of death in IE. Aortic valve IE producing acute severe aortic regurgitation is particularly catastrophic — the left ventricle has no time to accommodate the sudden volume overload (unlike chronic AR where the ventricle dilates gradually). Presents as acute pulmonary oedema. Requires emergency surgery.
- Paravalvular abscess: extension of infection beyond the valve annulus into the fibrous skeleton of the heart. Most common in aortic valve IE (aortic root abscess). Detected by TOE. New conduction abnormalities on ECG (PR prolongation, new bundle branch block) in a patient with known aortic valve IE = paravalvular abscess until proven otherwise — an urgent surgical indication.
- Pericarditis: purulent pericarditis or haemopericarditis from extension of infection.
- Intracardiac fistula: abscess rupture creating a communication between cardiac chambers or the aorta.
Embolic complications:
- Ischaemic stroke: the most feared complication, occurring in 15–20% of IE cases. Left-sided vegetations on the mitral or aortic valve are the source. Vegetation size >10 mm and S. aureus IE are independent risk factors. New stroke or TIA during IE management changes the risk-benefit calculation for surgery (CNS haemorrhage from haemorrhagic transformation is a contraindication to surgery for at least 1 month; ischaemic stroke without haemorrhage is not a contraindication).
- Septic emboli: to spleen (splenic infarct or abscess), kidney (renal infarct, haematuria), mesenteric vessels (mesenteric ischaemia), and limb vessels (acute limb ischaemia).
- Septic pulmonary emboli: right-sided IE → bilateral cavitating nodules on CXR/CT.
- Mycotic aneurysm: infected aneurysmal dilation at embolic arterial sites — most critically the intracranial circulation (cerebral mycotic aneurysm). Should be sought by CT or MRI angiography in IE with neurological symptoms.
Renal complications: Immune complex-mediated glomerulonephritis (focal or diffuse proliferative GN) causes haematuria, proteinuria, and declining renal function. Distinct from embolic renal infarcts (also causes haematuria but with loin pain). Both are common; together they explain why renal function monitoring is mandatory during IE management.
Musculoskeletal complications: Arthralgia and myalgia are common in SIE from immune complex deposition. Septic arthritis can occur from haematogenous seeding. Vertebral osteomyelitis (spondylodiscitis) — particularly in elderly patients with S. aureus IE — causes back pain and requires prolonged IV antibiotics.
Prognostic factors predicting poor outcome (high in-hospital mortality, 15–30%):
- S. aureus as the causative organism (high virulence, rapid destruction)
- Prosthetic valve IE
- Insulin-dependent diabetes mellitus
- Acute heart failure at presentation
- Periannular complications (abscess, fistula)
- Embolic stroke
- Delayed diagnosis and therapy
Self-assessment case vignette for integration:
A 40-year-old man with aortic valve IE due to S. aureus has been on IV flucloxacillin for 5 days when he develops a new first-degree AV block (PR 0.22 s) on ECG monitoring. The next morning he is more breathless and his repeat TOE shows a new small periaortic abscess with mild extension into the interventricular septum. What is the appropriate management decision?
Answer: New conduction defect (PR prolongation) in aortic IE = paravalvular abscess extending towards the conduction system. TOE confirms this. This is a surgical emergency — surgical indication: uncontrolled infection (perivalvular extension/abscess). Urgent cardiac surgery should be arranged without waiting for antibiotic completion. Continuing antibiotics alone risks further spread, complete heart block, and fatal haemodynamic compromise.
Complications of Infective Endocarditis
SELF-CHECK
A 25-year-old IVDU is being treated for right-sided Staphylococcus aureus endocarditis (tricuspid valve vegetation 14 mm) with IV vancomycin. On day 8 of treatment, he develops acute onset right-sided pleuritic chest pain and haemoptysis. His chest X-ray shows bilateral peripheral wedge-shaped opacities. He is haemodynamically stable. What is the most likely explanation for the new chest findings?
A. New left-sided IE causing systemic arterial embolism
B. Septic pulmonary emboli from the tricuspid valve vegetation
C. Paravalvular aortic abscess with pericardial rupture
D. Drug-induced pneumonitis from vancomycin
Reveal Answer
Answer: B. Septic pulmonary emboli from the tricuspid valve vegetation
This is a classic presentation of septic pulmonary emboli complicating right-sided IE. The tricuspid valve is on the right side of the heart — vegetations here embolise into the pulmonary arterial circulation (NOT the systemic circulation, which is the complication of left-sided IE). Septic pulmonary emboli classically produce bilateral peripheral, wedge-shaped opacities on CXR (pulmonary infarcts + cavitation from infected tissue). Pleuritic chest pain and haemoptysis are typical presenting symptoms. This complication does not always require a change in antibiotics; the priority is continued antibiotic therapy for the underlying IE. Haemodynamic stability is reassuring; significant haemoptysis or worsening respiratory function may prompt surgical consideration.
CLINICAL PEARL
Three critical pearls for infective endocarditis in clinical practice:
Pearl 1 — Blood cultures BEFORE antibiotics, always: The diagnostic yield of blood cultures drops precipitously once even a single dose of antibiotics has been administered. In a stable, subacute presentation, there is no clinical justification for delaying blood cultures. In a haemodynamically unstable patient with AIE, take all three sets rapidly (within 30 minutes) and then start antibiotics immediately — do not let antibiotic administration wait for cultures, but do not start antibiotics before taking the cultures.
Pearl 2 — New conduction defect + aortic valve IE = surgical emergency: A new PR prolongation, new bundle branch block, or new complete heart block in a patient with aortic valve endocarditis signals extension of infection into the periaortic fibrous tissue and the conduction system — a paravalvular abscess. This is an urgent surgical indication. Missing this sign on serial ECGs in an ICU patient risks complete heart block and cardiac arrest.
Pearl 3 — Streptococcus bovis endocarditis = colonoscopy: S. bovis (now reclassified as S. gallolyticus) endocarditis is associated with colonic pathology — adenoma and adenocarcinoma of the colon — in up to 25–80% of cases. Every patient with S. bovis endocarditis who has not recently had colonoscopy must be referred for lower GI tract evaluation to exclude colorectal malignancy, regardless of the presence or absence of GI symptoms.