Page 7 of 23
IM10.9-11 | Renal Failure Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit a focused history that differentiates AKI from CKD and identifies aetiology, nephrotoxin exposure, and systemic causes
- Perform a systematic clinical examination to determine volume status, oedema, uraemic features, and signs of underlying systemic disease
- Generate a prioritised differential diagnosis using the pre-renal/intrinsic/post-renal framework and clinical pattern recognition
INSTRUCTIONS
Clinical evaluation of a patient with renal failure is the foundational skill on which all diagnostic and management decisions rest. This module walks you through the structured history, systematic examination, and differential diagnosis generation that constitute the IM-skills arc for IM10.9–10.11 at the SH (Skill demonstrated with help) and KH levels.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 307–308 — AKI and CKD (textbook)
- API Textbook of Medicine, 10th ed., Ch. Nephrology — Clinical Approach to Renal Disease (textbook)
- Davidson's Principles & Practice of Medicine, 23rd ed., Ch. 17 — Clinical Assessment in Kidney Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the duty medical officer and are called to see two patients on the same ward, both with a report of 'elevated creatinine.' Patient A is a 62-year-old woman with known type 2 diabetes, on an ACEI, who was admitted yesterday for a urinary tract infection and started on IV gentamicin. Her creatinine today is 2.4 mg/dL, and the nurse reports she has passed only 150 mL of urine in the last 8 hours. Patient B is a 48-year-old man admitted for breathlessness; his creatinine is 5.8 mg/dL but he has no idea he had any kidney problem before. His legs are oedematous to the thigh, his JVP is elevated at 6 cm, and he has bilateral basal crepitations. Both patients have renal failure — but the question of whether each has AKI or CKD, what category of AKI they have, and what is driving the creatinine up, cannot be answered by looking at the creatinine number alone. It can only be answered by taking a focused history and performing a careful physical examination. The clinical evaluation is not a prelude to the real work of ordering tests — it IS the diagnostic work. Every physical finding you elicit and every historical detail you gather shapes the differential, focuses the investigation, and guides the first critical management steps.
WHY THIS MATTERS
For the NMC competencies IM10.9 (SH) and IM10.10 (SH), you must be able to elicit and document a complete history that differentiates AKI from CKD, identifies the aetiology within the pre-renal/intrinsic/post-renal framework, screens for nephrotoxins and systemic causes, and perform a clinical examination that establishes volume status, uraemic findings, and associated systemic disease. IM10.11 (KH) requires you to generate and prioritise a differential diagnosis. These are bedside skills that will be assessed in OSCEs and clinical vivas — they require rehearsal, pattern recognition, and the discipline of systematic approach under pressure.
RECALL
Before proceeding, activate your prior knowledge from the AKI and CKD foundations modules. Recall the three-category framework: pre-renal (inadequate perfusion → concentrated, sodium-poor urine), intrinsic renal (tubular/glomerular/interstitial/vascular injury), and post-renal (obstructed outflow → hydronephrosis). Recall the distinguishing feature of CKD: duration >3 months, often with small kidneys and established complications (anaemia, hyperphosphataemia, secondary hyperparathyroidism). Recall also that the kidney is often the target of systemic diseases — diabetes, hypertension, lupus, vasculitis, amyloid, myeloma — and that a patient presenting with elevated creatinine may have a primary kidney disease or a systemic disease manifesting in the kidney. The history you are about to practise is designed to disentangle these possibilities.
Clinical Indication and Approach to Renal Evaluation
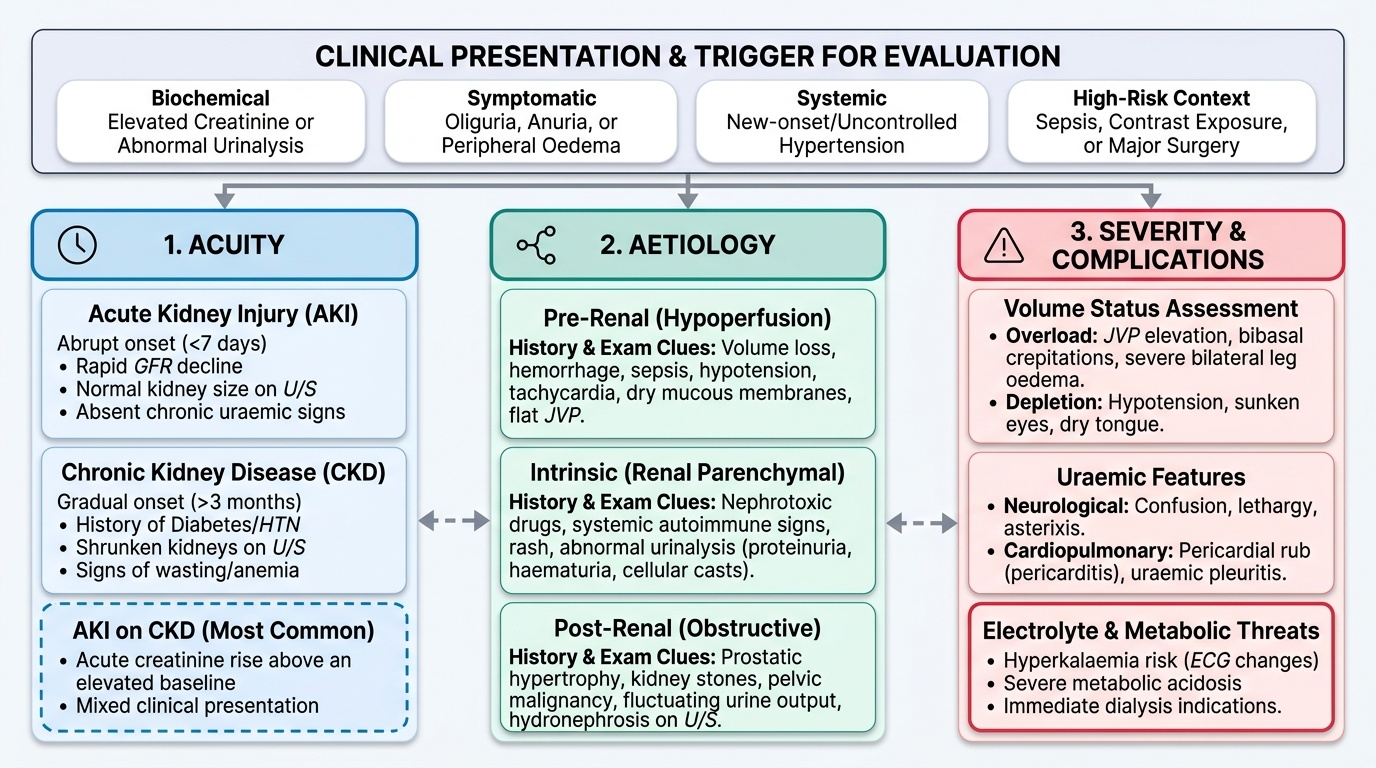
The clinical evaluation of a patient with suspected or confirmed renal failure is indicated whenever any of the following trigger presentations is encountered: an elevated serum creatinine above the laboratory reference range, new-onset oliguria or anuria, peripheral or periorbital oedema of uncertain cause, hypertension of new onset or poorly controlled established hypertension, abnormal urinalysis (proteinuria, haematuria, casts), electrolyte disturbances pointing to renal dysfunction (hyperkalaemia, metabolic acidosis with normal anion gap or high anion gap), or features of uraemia (nausea, vomiting, confusion, pericardial rub). The clinical evaluation is also essential at any point of known risk — major surgery, contrast exposure, sepsis, prolonged hypotension, or initiation of a potentially nephrotoxic drug — even before the creatinine has risen, to establish a baseline and to identify warning signs.
Provided image
The purpose of the clinical evaluation in renal failure is threefold: first, to determine acuity — is this AKI, CKD, or AKI on CKD (the most common scenario in hospitalised patients)? Second, to determine aetiology within the classification framework — which of the three categories (pre-renal, intrinsic, post-renal) is operative, and what is the specific cause within that category? Third, to assess severity and complications — is the patient volume-overloaded or volume-depleted? Are there signs of uraemia? Is hyperkalaemia threatening? Is there haemodynamic compromise? These three goals shape the structure of both the history and the examination. A clinician who addresses all three in a systematic way will arrive at the first management priorities before the investigation results return.
The general appearance of the patient provides the first diagnostic signal. A patient who is pale, lethargic, with a dull yellowish tinge to the skin, mild periorbital puffiness, and muscle wasting at the temporal fossae is likely to have advanced CKD with uraemia. A patient who is acutely unwell, hypotensive, tachycardic, with sunken eyes and dry mucous membranes is likely to have pre-renal AKI from volume depletion. A patient with massive bilateral leg oedema, elevated JVP, and bibasal crepitations has volume overload from heart failure or nephrotic syndrome — and their 'pre-renal' AKI is driven by low effective circulating volume, not absolute volume depletion. The clinical story begins the moment you enter the room.
Taking a Focused Renal History
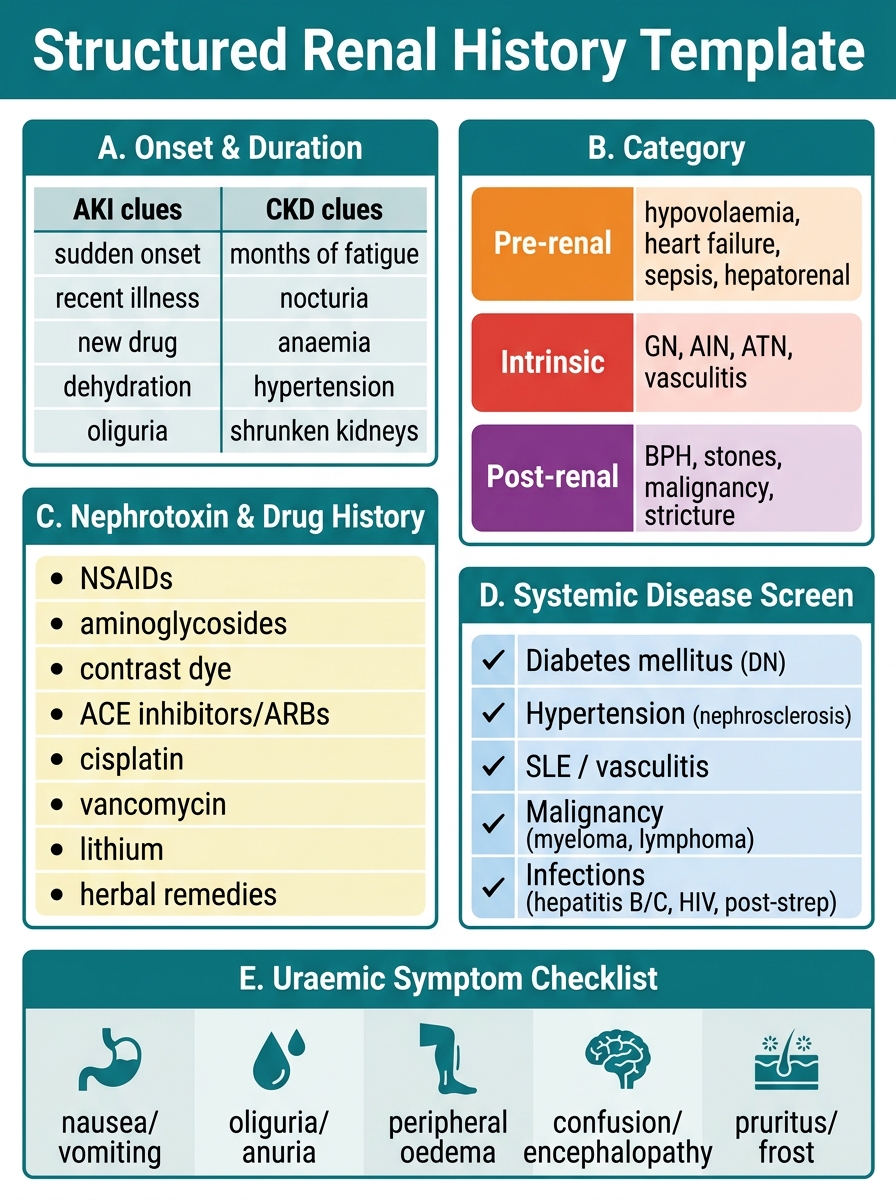
The renal history is structured around five essential domains, each contributing diagnostic information that cannot be reliably obtained from laboratory tests alone. Systematic coverage of all five domains ensures no critical information is missed. The history should ideally be taken from the patient, but corroboration from family members or treating physicians is often needed, particularly if the patient is encephalopathic.
Domain 1 — Onset and Duration (AKI vs CKD): The first question in every renal history is: how long has this been going on? AKI is defined as days to weeks; CKD requires >3 months. Key discriminating questions: Has the patient had prior creatinine or eGFR measurements? (A creatinine of 1.6 mg/dL may represent long-standing stable CKD or acute deterioration — only prior values confirm which.) When was the patient last clinically well? Was the onset sudden (hours to days — suggesting pre-renal or obstructive cause) or gradual and insidious (suggesting CKD)? Has the patient had prior kidney-related diagnoses, proteinuria on routine testing, or HTN attributed to 'kidney disease'? Symptoms that suggest chronicity include: long-standing nocturia (the failing kidney cannot concentrate urine, leading to polyuria reversed at night), long-standing pruritus, restless legs, fatigue extending over months, and previously small kidneys on imaging.
Domain 2 — Identifying the Category (Pre-renal, Intrinsic, Post-renal): For pre-renal causes: Has there been fluid loss — diarrhoea, vomiting, bleeding, burns, high fever sweating? Has the patient reduced fluid intake? Is there underlying heart failure or liver disease that could reduce effective circulating volume? Review of medications for recent ACE inhibitor or NSAID initiation is critical — both reduce intraglomerular filtration pressure. For intrinsic causes: Has the patient received a nephrotoxic drug — aminoglycoside, contrast, NSAID, cisplatin, amphotericin? Any herbal or traditional medications (a common and underreported cause in India)? Any recent illness with high fever, jaundice, rash, or dark urine (suggestive of leptospirosis, malaria, AIN, or haemolysis)? Snake bite, crush injury, or toxic ingestion? For post-renal causes: Is there a history of difficulty initiating urination, poor urine stream, dribbling, frequency (BPH in men), pelvic malignancy, retroperitoneal fibrosis, or calculi?
Domain 3 — Nephrotoxin and Drug History: Ask specifically about: NSAIDs (ibuprofen, diclofenac — widely available OTC); aminoglycosides; traditional herbal preparations and Ayurvedic/homeopathic medications (many contain nephrotoxic heavy metals or aristolochic acid); radiocontrast procedures; tenofovir (in HIV patients — proximal tubular injury); chemotherapy agents; lithium (in psychiatric patients); and illicit drug use. Recent vaccination or medication changes may suggest AIN.
Domain 4 — Systemic Disease Screen: Ask about symptoms and diagnoses that point to systemic diseases causing renal failure: long-standing diabetes and hypertension (the two most common); systemic lupus (malar rash, joint pains, photosensitivity, prior episodes of haematuria); vasculitis (nasal symptoms, haemoptysis — Wegener's/granulomatosis with polyangiitis); haematological malignancy (bone pain, fatigue, weight loss — myeloma); liver disease (jaundice, ascites — hepatorenal syndrome); and cardiac disease (angina, breathlessness — cardiorenal syndrome). In India, always ask about fever with rigors (malaria — blackwater fever and AKI), fever with jaundice (leptospirosis), prolonged cough and weight loss (TB — important for rifampicin-AIN).
Domain 5 — Functional Impact and Uraemic Symptoms: Enquire about symptoms that indicate the degree of kidney dysfunction: nausea, vomiting, anorexia (uraemic toxins affecting the gut); metallic taste in mouth (uraemic dysgeusia); decreased urine output or change in urine colour (dark brown = myoglobinuria or haematuria; frothy = proteinuria); swelling of legs or face (oedema); breathlessness (pulmonary oedema or uraemic pleuritis); confusion, memory difficulty, sleep disturbance (uraemic encephalopathy); chest pain (uraemic pericarditis); muscle cramps and restless legs; and pruritus (uraemic or from hyperphosphataemia).
Structured Renal History Template: Five-Domain Clinical Card
SELF-CHECK
A 55-year-old man presents with serum creatinine 3.8 mg/dL. His baseline creatinine 3 years ago was 1.1 mg/dL. He reports nocturia for 2 years, gradual fatigue over 6 months, and mild pruritus for 3 months. He has no recent illnesses, no new medications, and no change in urine output. Which feature MOST supports a diagnosis of AKI on pre-existing CKD rather than de novo AKI?
A. Pruritus
B. Nocturia for 2 years and gradual fatigue for 6 months
C. Creatinine 3.8 mg/dL
D. No change in urine output
Reveal Answer
Answer: B. Nocturia for 2 years and gradual fatigue for 6 months
Nocturia for 2 years and gradual fatigue for 6 months both indicate chronicity — the failing kidney's inability to concentrate urine at night (isosthenuria) and the slow accumulation of anaemia are hallmarks of long-standing CKD. The prior creatinine of 1.1 mg/dL is important context, but the clinical symptoms spanning 2 years are what most strongly confirm that this is not an acute-onset process. Pruritus, while a uraemic symptom, can occur in both acute and chronic settings. The absolute creatinine value and absence of oliguria do not distinguish AKI from CKD.
Systematic Physical Examination in Renal Failure
The physical examination in renal failure is conducted as a fully systematic head-to-toe survey, but with particular attention to three high-yield domains: volume status, uraemic features, and signs of systemic causative disease. Each domain informs a different aspect of the diagnosis and management plan, and findings in one domain often complement and validate findings in another. The examination begins with general observation — the overall appearance of the patient communicates the acuity and chronicity of renal failure before a single specific sign is elicited. A pale, sallow, muscle-wasted patient with periorbital puffiness signals months of uraemia; a hypotensive, dry-mouthed, tachycardic patient signals acute haemodynamic compromise; a blue-tinged, breathless patient with a raised venous pulse and crackles signals cardiac failure as the driver. Vital signs — pulse rate and regularity, blood pressure (lying and standing), respiratory rate, and temperature — are recorded before the detailed regional examination and provide the physiological context in which individual findings are interpreted.
Volume Status Assessment: This is the single most critical component of the examination in AKI, because the distinction between volume-depleted pre-renal AKI and volume-overloaded cardiorenal or nephrotic AKI determines the management — fluids in the former, diuresis in the latter. Volume assessment requires a multi-parameter approach because no single sign is reliable in isolation:
- Signs of volume depletion: dry mucous membranes, decreased skin turgor (test over the sternum or forehead — less reliable over the dorsum of the hand in elderly patients), sunken eyes, cool peripheries with prolonged capillary refill (>2 seconds), postural hypotension (>20 mmHg fall in systolic or >10 mmHg fall in diastolic BP on standing), tachycardia, and flat neck veins. A positive postural drop in a tachycardic patient confirms hypovolaemia with reasonable sensitivity.
- Signs of volume overload: elevated JVP (measured with patient at 45°, as vertical distance from sternal angle to the top of the venous pulsation column — normal ≤3–4 cm above the sternal angle), bibasal fine inspiratory crepitations (pulmonary oedema), peripheral pitting oedema (graded by depth of pit and height up the leg — ankle/shin grade 1–2, to thigh/sacral grade 3–4), sacral oedema in supine patients, ascites (shifting dullness, fluid thrill), and pleural effusion (reduced breath sounds, stony dull percussion). Elevated JVP combined with oedema and crepitations = volume overload with cardiac or renal cause.
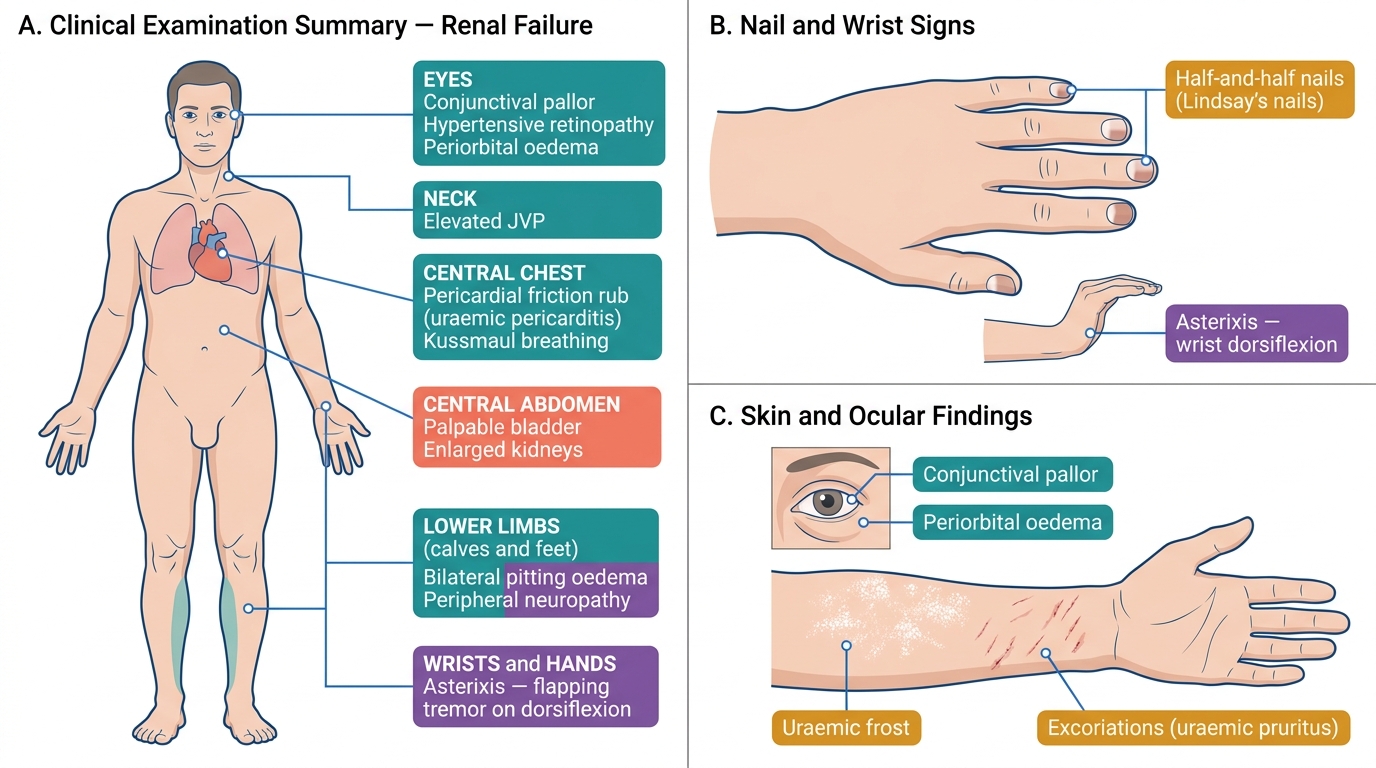
Uraemic Features on Examination:
- Skin: pallor (anaemia of CKD), yellowish tinge (sallow complexion from retained carotenoids), scratch marks (pruritus), uraemic frost (rare white crystalline deposit from urea precipitation — virtually pathognomonic of severe uraemia), ecchymoses and petechiae (platelet dysfunction), and Muehrcke's lines or Lindsay's nails (half-and-half nails — distal brown band with proximal white — associated with hypoalbuminaemia in CKD/nephrotic syndrome).
- Neurological: asterixis (hold wrists dorsiflexed, fingers spread — a flapping tremor indicates metabolic encephalopathy), cognitive impairment (disorientation, poor concentration), myoclonus, peripheral neuropathy findings (reduced ankle reflexes, impaired vibration sense in a stocking distribution).
- Cardiovascular: pericardial friction rub (three-component; louder leaning forward; uraemic pericarditis), BP (hypertension present in most CKD patients), left ventricular heave (from hypertensive LVH).
- Respiratory: Kussmaul breathing (deep, regular, sighing respirations — compensatory hyperventilation for metabolic acidosis); uraemic pleuritis (pleural rub).
- Musculoskeletal: bone tenderness (renal osteodystrophy, particularly the tibial crest and ribs in secondary hyperparathyroidism); proximal muscle weakness (1,25-dihydroxyvitamin D deficiency).
Signs of Systemic Causative Disease:
- Diabetic stigmata: diabetic retinopathy (fundoscopy — Cotton wool spots, haemorrhages, exudates; retinopathy correlates with nephropathy in type 2 DM), reduced pedal pulses and sensation (diabetic peripheral vascular disease and neuropathy).
- Hypertension: arteriovenous nipping, silver wiring on fundoscopy; left ventricular hypertrophy on apex beat.
- Connective tissue diseases: malar rash (SLE), oral ulcers (SLE/vasculitis), arthritis, alopecia, livedo reticularis.
- Enlarged kidneys (palpable or percussion-detectable): polycystic kidney disease (bilateral large knobbly kidneys), amyloidosis, lymphoma, bilateral hydronephrosis.
- Bladder distension: a palpable or percussible bladder above the symphysis pubis suggests bladder outlet obstruction — present even in an apparently anuric patient if obstruction is complete.
- Anaemia signs: conjunctival pallor, mucosal pallor, tachycardia.
Document all findings formally in a structured clinical note: general appearance → vital signs → head and neck (JVP, mucous membranes, fundoscopy) → chest (heart sounds including rub, breath sounds, crepitations) → abdomen (liver, spleen, kidneys, bladder, ascites) → lower limbs (oedema, pulses, peripheral neuropathy) → neurological (asterixis, level of consciousness, reflexes).
Clinical Examination Findings in Renal Failure
SELF-CHECK
During examination of a 68-year-old man with creatinine 6.1 mg/dL, you elicit a three-component pericardial friction rub and bilateral ankle oedema to the mid-shin. His JVP is 5 cm above the sternal angle. His hands show a flapping tremor on wrist dorsiflexion. Which uraemic complication is represented by the flapping tremor?
A. Uraemic platelet dysfunction
B. Peripheral neuropathy
C. Asterixis from uraemic encephalopathy
D. Restless legs syndrome
Reveal Answer
Answer: C. Asterixis from uraemic encephalopathy
Asterixis (flapping tremor on wrist extension) is caused by brief lapses in postural tone resulting from metabolic encephalopathy — in this context uraemic encephalopathy. It is not a tremor in the classical sense but a metabolic-induced postural lapse seen in any metabolic encephalopathy (uraemia, hepatic failure, CO₂ narcosis). The pericardial rub indicates uraemic pericarditis. Platelet dysfunction causes bleeding, not a motor sign. Peripheral neuropathy would produce reduced reflexes and sensory loss. Restless legs is a subjective symptom, not a flapping tremor.